
Abstract
Background and Purpose:
Laparoendoscopic single-site surgery (LESS), an attempt to further enhance the cosmetic benefits of minimally invasive surgery while minimizing the potential morbidity associated with multiple incisions, has been developed recently. Our aim was to compare LESS simple nephrectomy (LESS-SN) and conventional transperitoneal laparoscopic simple nephrectomy (CTL-SN).
Patients and Methods:
In this randomized study that was conducted between December 2008 and September 2009, 27 patients who needed simple nephrectomy were randomized to either LESS-SN or CTL-SN. All procedures in both groups were performed by the first author, who is experienced in laparoscopic surgery. Patient characteristics, perioperative details, and time to return to work were recorded. Postoperative evaluation of pain and use of analgesic medication were recorded.
Results:
There was no difference in median operative time (117.5 vs114 min, P = 0.52), blood loss (50.71 vs 47.15 mL, P = 0.60), transfusion rates (0% for both), and hospitalization time (2.07 vs 2.11 days, P = 0.74) between the LESS-SN and CTL-SN groups. Time to return to normal activities was shorter in the LESS-SN group compared with the CTL-SN group (10.7 vs 13.5 days, P = 0.001). Both the visual analogue scale and the postoperative use of analgesics were significantly lower during postoperative days 1, 2, and 3 in patients who underwent LESS-SN, compared with patients who underwent CTL-SN. There were no intraoperative or postoperative complications in both groups. Compared with CTL-SN, LESS-SN was more expensive, but all patients undergoing LESS-SN were very pleased with the cosmetic outcome (no visible scars).
Conclusion:
The early experience described in this study suggests that LESS-SN is a safe and effective alternative to CTL-SN that provides surgeons with a minimally invasive surgical option and the ability to hide the surgical incision within the umbilicus; however, a larger series is necessary to confirm these findings and to determine if there are any benefits in pain, recovery, or cosmesis.
Introduction
Since the introduction of laparoscopy in the early 1990s that ushered in a new area in the surgical management of human diseases, there has been a trend toward minimizing the number of incisions and ports necessary, and this has led to the description of laparoendoscopic single-site surgery (LESS). In the published literature, various terms have been used for this procedure, but the LaparoEndoscopic Single-Site Surgery Consortium for Assessment and Research coined the term LESS as acceptable for all single-incision procedures to avoid confusion with multiple terminologies. 2
Since the initial report of single-port nephrectomy in 2007 by Rane and associates, 3 single-port laparoscopic procedures, such as donor nephrectomy, 4 pyeloplasty, 5 and ureterolithotomy, 6 have been performed. Only a few retrospective studies that compare the results of the LESS-nephrectomy procedure to the conventional laparoscopic nephrectomy technique are currently available. 7,8
To our knowledge, there is no published randomized controlled study to compare the outcomes of LESS-nephrectomy with those of conventional laparoscopic nephrectomy. The aim of this prospective randomized study was to better define potential benefits of LESS-simple nephrectomy (LESS-SN) and compare it with conventional transperitoneal laparoscopic-simple nephrectomy (CTL-SN).
Patients and Methods
Patient selection
Between December 2008 and September 2009, 27 patients who needed simple nephrectomy were randomized to either LESS-SN or CLT-SN. Fourteen patients were assigned to LESS-SN, and the rest underwent CTL-SN. All procedures in both groups were performed by the first author (VT) who is experienced in laparoscopic surgery. Patients were included in the groups consecutively—one patient to the LESS-SN group and the next to the CTL-SN group—for randomization.
The indications for the LESS-SN and CTL-SN groups were similar benign disease of the kidney. Both groups of patients had surgery after obtaining Institutional Review Board approval from the ethical committee and informed patient consent.
Surgical procedures
All the procedures in both groups were performed under general anesthesia. The LESS-SN procedure was performed with the patient in a 45-degree flank position for transperitoneal surgery; a 2-cm semilunar-shaped skin incision was concealed completely within the umbilicus (Fig. 1), and deepened to the anterior rectus fascia, where a 2.5-cm fascial incision was made; the peritoneum was incised, and the SILS-Port (Covidien, Norwalk, CT) was deployed. The SILS-Port was placed intraperitoneally with the help of a clamp.
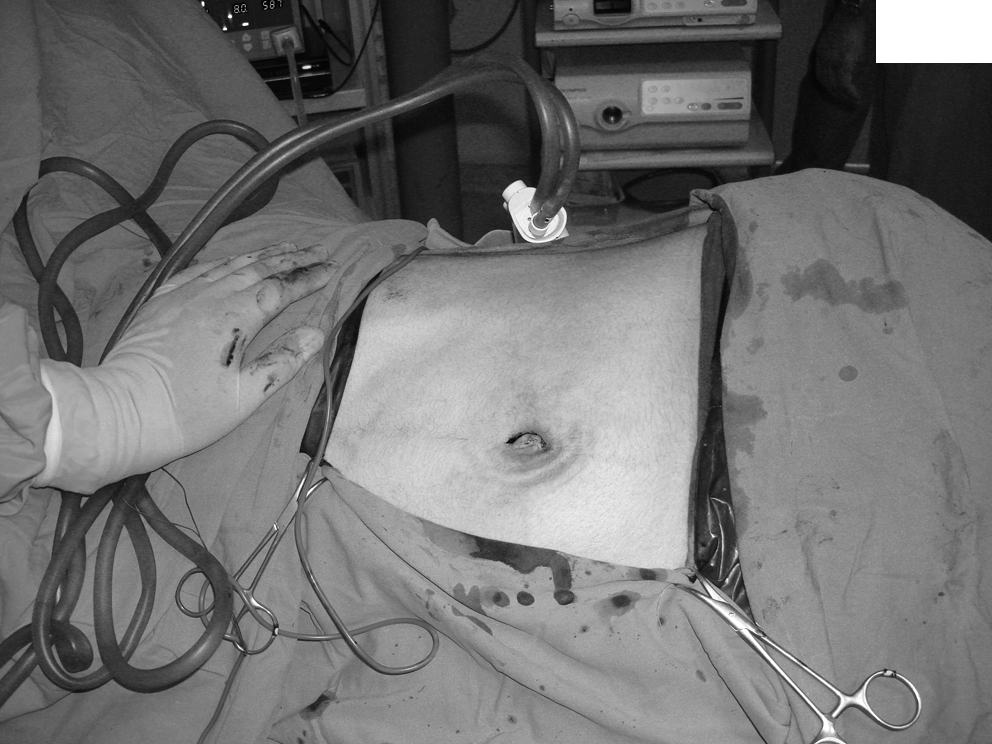
Semilunar-shaped skin incision, concealed within the umbilicus.
For the CTL-SN procedure, an open access (Hasson) technique was used to establish pneumoperitoneum. Pneumoperitoneum was created by carbon dioxide insufflation, and the pressure was kept at 10 to 15 mm Hg. A camera port was placed instead of the SILS-Port, and two or three additional ports were used. For LESS procedures, a 5-mm 30-degree high-definition rigid laparoscope with integrated different cameras (Karl Storz, Tuttlingen, Germany, and Gimmi, Tuttlingen, Germany) was used along with two working instruments. During LESS procedures a combination of flexible forceps and scissors (Cambridge Endoscopic Devices, Cambridge, MA, and Tyco Healthcare Group, LP, Mansfield, MA) and conventional laparoscopic (straight) instruments (eg, scissors, ultrasound scissors, bipolar forceps) were used to perform the procedures as necessary.
All LESS procedures were performed through an intraumbilical single-access multichannel laparoscopic port, the SILS-Port (Covidien, Norwalk, CT).
No additional port was used for tissue retraction, and all procedures were performed through the SILS-Port. In this procedure, an additional polypropylene mesh was designed as a hammock and attached to the abdominal wall with the help of sutures and Hem-o-Lok clips were used for liver retraction for right-side nephrectomies. Sutures for liver retraction were passed transabdominally by a 60-mm, straight needle (Caprosyn, Covidien, Norwalk, CT). In the CTL-SN group, when necessary for right-side nephrectomies, an additional 5-mm subxyphoid port is placed for liver retraction.
The various operative steps were similar in both groups. In the LESS-SN group, the straight instrument in the left hand was used to dissect the tissue while the peritoneal incision along the line of Toldt was performed with a roticulating laparoscopic scissor held in the right hand (Cambridge Endoscopic Devices, Cambridge, MA).
The morcellated specimens were removed through the first port incision via the umbilical incision in the CTL-SN group and the umbilical incision in the LESS-SN group. Histopathologic examination was performed for all specimens. The drain was removed the morning after the procedure. Routine postoperative care for standard laparoscopic cases was followed.
Operative time, blood loss, transfusion rates, postoperative pain, perioperative complications (occuring within the first month of the nephrectomy procedure), hospitalization time, and time to return to normal activities were the main perioperative parameters evaluated to compare LESS-SN and CTL-SN.
The visual analogue scale (VAS) and the necessary analgesic during the postoperative course were used to evaulate postoperative pain. The evaluation of pain was achieved with the documentation of the patient's perceived pain on an analogue pain scale that ranged from 1 to 10. VAS was measured at 3 days and 3 months postoperatively. The consumption of analgesic medication for the first 2 postoperative days was recorded. The medication used for analgesia was morphine sulfate equivalent and was administered intramuscularly at 50 mg doses, if necessary. Patient satisfaction was assessed postoperatively. The cost of all surgical instruments used in both procedures has been reported according to the current price in Turkey. Postoperative assessments (Fig. 2) included ultrasonography, urinalysis, and serum creatinine assay, which were performed routinely after the operation on the first month postoperatively.

Incision site after LESS-SN on postoperative day 30. LESS-SN = laparoendoscopic single-site surgery-simple nephrectomy.
Statistical analysis
The two groups were analyzed using the Mann-Whitney U test and chi-square test to determine whether a statistically significant difference was available; P < 0.05 was considered significant.
Results
Baseline characteristics and perioperative data of patients in the LESS-SN and CTL-SN groups are shown in Tables 1 and 2, respectively. The two groups were comparable with regard to age, sex, body mass index (BMI), and the affected side. All LESS-SN procedures were completed successfully with no conversions to conventional laparoscopic or open surgeries, and all CTL-SN procedures were performed with no conversion to open surgery. There was no mortality in either the LESS-SN or CTL-SN group. All patients were ambulatory and accepted oral food on the day after the operation.
Results of two groups were shown as mean values ± standard deviation. Statistical analyses of the gender evaluation were carried out by the chi-square test, and other data were analysed by the Mann-Whitney U test.
LESS-SN = laparoendoscopic single-site surgery-simple nephrectomy; CTL-SN = conventional transperitoneal laparoscopic-simple nephrectomy; BMI = body mass index.
Results of two groups were shown as mean values ± standard deviation. Statistical analyses of the data were analysed by the Mann-Whitney U Test.
LESS-SN = laparoendoscopic single-site surgery-simple nephrectomy; CTL-SN = conventional transperitoneal laparoscopic-simple nephrectomy.
In the CTL-SN group, procedures were successfully completed through three or four ports. In the LESS-SN group, the SILS-Port was used for all procedures. The drainage tube was removed the next morning in all cases, while we did not place any drain in two patients. The patients who had no drain had abdominal pain and discomfort in the early postoperative period. Both the VAS and the postoperative use of analgesics were significantly lower during postoperative days 1, 2, and 3 in patients who underwent LESS-SN, compared with patients who underwent CTL-SN (Table 3).
Data were shown as mean values ± standard deviation.
Mann-Whitney U test.
Administered intramuscularly.
LESS-SN = laparoendoscopic single-site surgery-simple nephrectomy; CTL-SN = conventional transperitoneal laparoscopic-simple nephrectomy.
There was no difference in the median operative time (117.5 vs 114 min, P = 0.52), blood loss (50.71 vs 47.15 mL, P = 0.60), transfusion rates (0% for both), and hospitalization time (2.07 vs 2.11 day, P = 0.74) between the LESS-SN and CTL-SN groups (Table 2). The time to return to normal activities was shorter in patients who underwent LESS-SN compared with patients who underwent CTL-SN (10.71 vs 13.50 day, P = 0.001). No significant intraoperative or postoperative complications occurred in either group.
LESS-SN was more expensive than CTL-SN, with costs ranging from $1600 to $2000 for LESS-SN and from $450 to $600 for CTL-SN (Table 4). Compared with CTL-SN, LESS-SN had a better cosmetic result and patient satisfaction.
LESS-SN = laparoendoscopic single-site surgery-simple nephrectomy; USD = United States dollars; CTL-SN = conventional transperitoneal laparoscopic-simple nephrectomy.
Nephrectomy was performed for benign kidney diseases in all cases consistent with chronic pyelonephritis and interstitial fibrosis without evidence of malignancy. The mean period of follow-up in the LESS-SN and CL-SN groups was 3 months. Postoperative assessments were normal. On follow-up, all patients were symptom free.
Discussion
In the past few years, the laparoscopic aproach to nephrectomy has gained widespread acceptance in the management of benign and malignant kidney diseases. New techniques have been developed to decrease the number of ports needed for safe laparoscopic surgery. As a result, interest in the introduction of LESS in various urologic surgeries has increased. 2,9
Recently, a few retrospective studies that compare laparoendoscopic single-site surgery-nephrectomy with conventional laparoscopic nephrectomy have been reported. 7,10 The purpose of the present study was to compare the feasibility of LESS-SN with CTL-SN, and to better define potential benefits of LESS-SN.
Raman and colleagues
10
compared a series of 11 LESS-Ns with a group of CTL-Ns. Nephrectomy was performed for both nonfunctioning kidney and enhancing renal mass. No differences in operative time, complication rate, narcotic analgesic use, postoperative hospitalization time, or transfusion requirement were observed between LESS-SN and CTL
In the present study, there was no difference in median operative time, blood loss, transfusion rates, and hospitalization time between the LESS-SN and CTL-SN groups. In contrast to the studies mentioned above, postoperative pain was significantly lower in patients who underwent LESS-SN, compared with patients who underwent CTL-SN.
Canes and associates 8 recently reported a retrospective comparison of LESS and standard laparoscopic left donor nephrectomy. Their preliminary data suggest that LESS donor nephrectomy shortens convalescence, as measured by pain medication requirement after discharge, time off work, and time to resolution of physical symptoms. Although the limitation of this study is inherent in its retrospective nature, LESS donor nephrectomy is certainly comparable or preferable to conventional laparoscopic nephrectomy with regard to the subjective cosmetic results and objective surgical results.
In the present study, because all nephrectomies were performed for benign lesions or nonfunctioning kidneys, the specimen was manually morcellated. Therefore, there was no need to enlarge the incision of the SILS-Port.
In our study, there was no significant difference between the mean operative time for patients undergoing LESS-SN or CTL-SN. All nephrectomy procedures in both groups were entirely performed by the first author (VT) who is experienced in laparoscopic surgery. In addition, the use of instruments that were developed for LESS (roticulating forceps, flexible instruments) has also been attributed to a lack of difference in operative time. Along with the development of appropriate instruments, LESS-SN may also provide shorter operative time. Because of perirenal inflammation, scarring, and loss of anatomic landmarks, it is especially difficult to perform hilar dissection in these cases. Correspondingly, several authors have emphasized the higher conversion and complication rate in such cases of nonfunctioning kidneys with underlying stone and/or infectious pathologies. 11 Therefore, in such cases, we did not open the Gerota fascia to avoid complications and conversion to an open procedure. This may be another factor that contributed to shorter operative time.
From the technical point of view, there are two approaches to laparoscopic simple nephrectomy (the transperitoneal and the retroperitoneal approach). In retroperitoneal laparoscopy, the kidney and its blood vessels are relatively easier to reach, but the working space is smaller, the orientation is difficult, and the ergonomy of the procedure is less than optimal because of the smaller working space and limitations by bony structures, such as the ribs and iliac crest. Because it is obviously clear that transperitoneal LESS-SN is easier to perform compared with the retroperitoneal approach, all LESS-SN procedures were performed transperitoneally in our study. We also preferred the transperitoneal aproach for all the conventional laparoscopic nephrectomies.
Operative complications related to trocar insertion, such as epigastric vessel injury, visceral organ damage, and herniation, might be reduced by eliminating the need for ancillary ports. In the present study, there was no complication in patients in either group.
Canes and colleagues 8 reported, after their comparative study, that patients undergoing LESS donor nephrectomy benefited from decreased pain, reduced hospitalization time, less blood loss, and rapid convalescence. Postoperative pain, which results from skin incision and penetrating muscle and fascia with the trocar, might be reduced in patients undergoing LESS donor nephrectomy. Similarly, in our study, both the VAS and the postoperative analgesic requirements were significantly lower during postoperative days 1, 2, and 3 in patients who underwent LESS-SN, compared with patients who underwent CTL-SN.
In addition to the advantages mentioned above, a better cosmetic result may also be obtained by a single incision. The single incision has the potential to decrease other complications related to surgical incisions, such as bleeding, internal organ damage, wound infection, and incisional hernia. 7,10
The present study showed that LESS-SN is more expensive than CTL-SN, because of the use of a disposable SILS-Port and other flexible instruments designed for LESS, such as the roticulating forceps. The costs of the LESS-SN and CTL-SN were around $1600 and $500, respectively. The major factor responsible for the operative cost was the SILS-Port in patients undergoing LESS-SN. The additional cost related to use of this special disposable device, the SILS-Port, can be ruled out by reusing this instrument in the developing countries. The operative complications related to trocar insertion, such as epigastric vessel injury, visceral organ damage, wound infection, and port-site herniation, would bring patients excessive suffering and cost. These intraoperative and postoperative complications might be reduced by performing the LESS-SN procedure. In addition, LESS-SN shortens convalescence, as measured by pain medication requirement after discharge, time off work, and time to resolution of physical symptoms.
There are a few limitations to this study. Our study has a small number of patients and compares two small sample groups. The present study should have been enhanced to a larger series of patients. Standardized quality-of-life scores could also have been used to assess patient satisfaction. Although our patients seem extremely satisfied with their postoperative cosmetic outcomes, scar satisfaction was not questioned in the present study. We have not yet quantified or compared scar satisfaction with a validated questionnaire.
Conclusion
The results of our study suggest that LESS-SN is a safe and effective alternative to CTL-SN that provides surgeons with an alternative minimally invasive surgical option and the ability to hide the surgical incision within the umbilicus; however, further prospective studies with higher numbers of patients are still needed.
Footnotes
Disclosure Statement
No competing financial interests exist.