
Abstract
Ureteral stent placement during adult laparoscopic pyeloplasty for ureteropelvic junction obstruction can be performed preoperatively or intraoperatively either in a retrograde or antegrade approach. Intraoperative retrograde stent placement is the most commonly used technique. Comparative studies, however, suggest that there is a significant component added to the overall operative times because of the need for patient repositioning from the lithotomy to the flank position before pyeloplasty. During our laparoscopic pyeloplasty surgery, we position the patient in the lateral decubitus position and incorporate a lower extremity support device for female patients. This allows initial open-ended catheter placement and subsequent access to the perineum and final stent placement throughout the procedure without need for patient repositioning. In addition, our technique allows for intraoperative fluoroscopy to delineate the complete ureteral anatomy. Since 2004, we have used this approach in 111 consecutive patients without complications. We describe our technique for intraoperative ureteral stent placement in the flank position during adult laparoscopic pyeloplasty without need for patient repositioning.
Introduction
Retrograde stent placement in the dorsal lithotomy position is the most familiar approach to urologists and can be performed before or in conjunction with the pyeloplasty. One limitation to preoperative stent placement is the resultant decompression of the renal pelvis, which may make clear delineation of the obstructing segment and anatomy difficult. In addition, excision of the obstructed segment as well as suture closure of the ureteropelvic anastomosis, particularly during the posterior repair, may be more difficult in the presence of the preplaced stent. 1
Alternatively, antegrade stent placement is typically performed after the completion of the posterior ureteropelvic anastomosis repair via the introduction of the stent through an existing laparoscopic port site or through a needle puncture site through the abdominal wall. 2 While this technique avoids many of the limitations of preplaced stent placement, there may be a learning curve associated with the antegrade approach, and confirmation of the distal stent curl location in the bladder can also be difficult without additional procedures. Similarly, evaluation of the distal ureter to rule out coexisting ureteral stricture cannot be performed without previous retrograde pyelography.
Intraoperative retrograde stent placement combines the benefits of the preoperative and antegrade approaches. Placement of an open-ended catheter in a retrograde fashion at the time of pyeloplasty allows for clear delineation of the ureteral anatomy as well as aids in identification of the ureter during laparoscopic dissection, which is especially of value in secondary reoperative repairs. Injection or withdrawal of fluid through the open-ended catheter is useful to aid in the mobilization of the UPJ. Intraoperative access to the catheter allows for direct handling during anastomotic suturing and the exchange to a ureteral stent under direct visualization at the time of anastomotic completion. This minimizes the probability of subsequent stent damage or migration.
Comparative studies, however, suggest that intraoperative retrograde stent placement adds a significant component to overall operative times. 2 This time increase is largely because of the need for patient repositioning and subsequent redraping from the dorsal lithotomy position to the flank position for the pyeloplasty.
We describe our technique for intraoperative retrograde ureteral stent placement and manipulation in the flank position during laparoscopic pyeloplasty without need for patient repositioning. Wayment and coworkers 3 recently reported a flank positioning technique for stent placement during robot-assisted pyeloplasty. Unlike other methods, our technique incorporates fluoroscopy for initial ureteral anatomy delineation and uses a lower extremity support device that, particularly in female patients, allows for complete bed maneuverability during subsequent pyeloplasty.
Between February 2004 and October 2009, we have used this approach in 111 consecutive patients (46 male, 65 female). The mean patient age was 39 years (18–78) and the mean body mass index (BMI) was 26.5 (18–51). The mean total operative time was 236 minutes (range 143–434 min) and did not differ significantly between men and women (P = 0.97). One man needed repositioning to the dorsal lithotomy position for final stent placement after the pyeloplasty because of edema at the ureteral orifice and the need for ureteral dilation. Two additional women underwent initial intraoperative stent placement in the dorsal lithotomy position; one because of an increased BMI and inability to safely secure the ipsilateral leg and one potentially needing distal ureteral treatment.
There were no occurrences of postoperative neuropathy, deep vein thrombosis, or perioperative complications related to positioning. One woman was noted to have stent migration out of the urethra necessitating stent manipulation. Postoperatively, there were two occurrences of urine leak and two patients with prolonged ileus. Mean duration (range) of stent placement was 46 days (14–76 d) with subsequent removal during office cystoscopy.
Technique
The patient is placed in the lateral decubitus position as is standard during kidney procedures. The surgical bed is manipulated with the kidney rest partially raised and the bed varied in the flexion and Trendelenburg positions to allow for maximal flank exposure. Dorsal brackets and padding are used at the shoulder and iliac crest levels for additional support to allow near supine roll of the table. In female patients, the ipsilateral leg is carefully placed in a padded Yellofin Elite stirrup (Allen, Acton, MA) angled to allow direct access to the perineum (Fig. 1). Particular attention is made to carefully pad the elevated leg. The flank and perineum are prepped and draped in the usual sterile fashion.
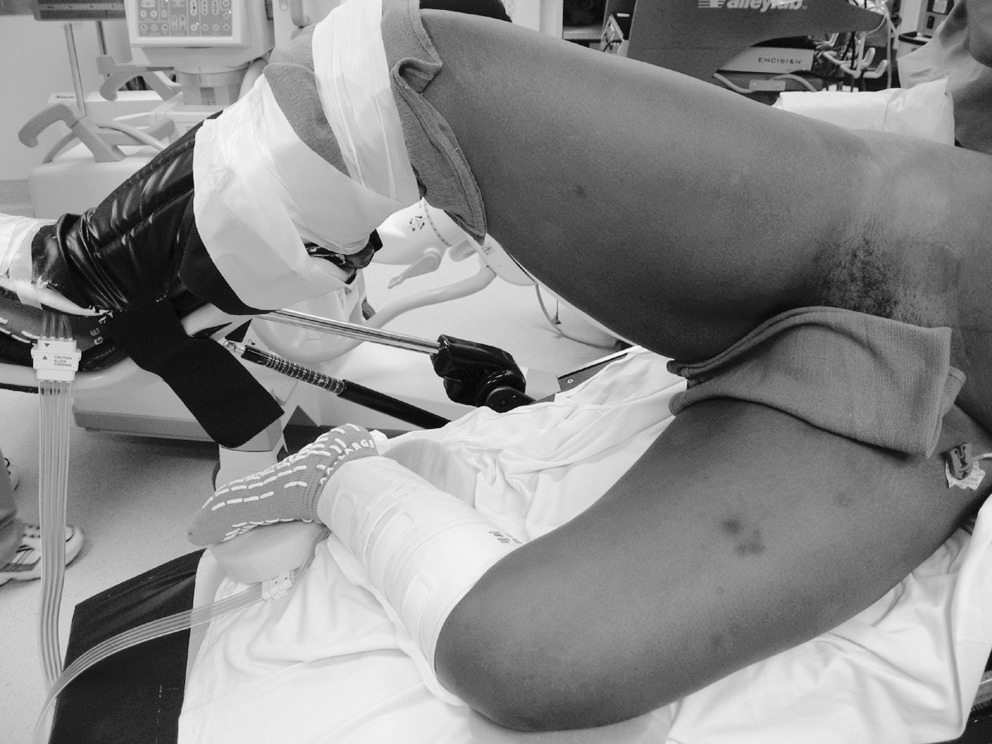
Patients are placed in the lateral decubitus position. In female patients, the ipsilateral leg is placed in a padded stirrup that is angled to allow direct access to the perineum.
Flexible cystoscopy is performed at the beginning of the procedure with a 5F open-ended angiographic catheter placed over a super-stiff guidewire into the distal ureter (Fig. 2). The fluoroscopic C-arm is inverted and rotated so that the beam generator device and image intensifier are positioned from the vertical to horizontal axis (Fig. 3). Retrograde pyelography is then performed through the open-ended catheter to fully delineate the segment of obstruction as well as distend the renal pelvis. The wire is then replaced into the open-ended catheter just distal to the UPJ, and both are secured externally to the surgical drape. A Foley catheter is placed for bladder drainage during surgery.
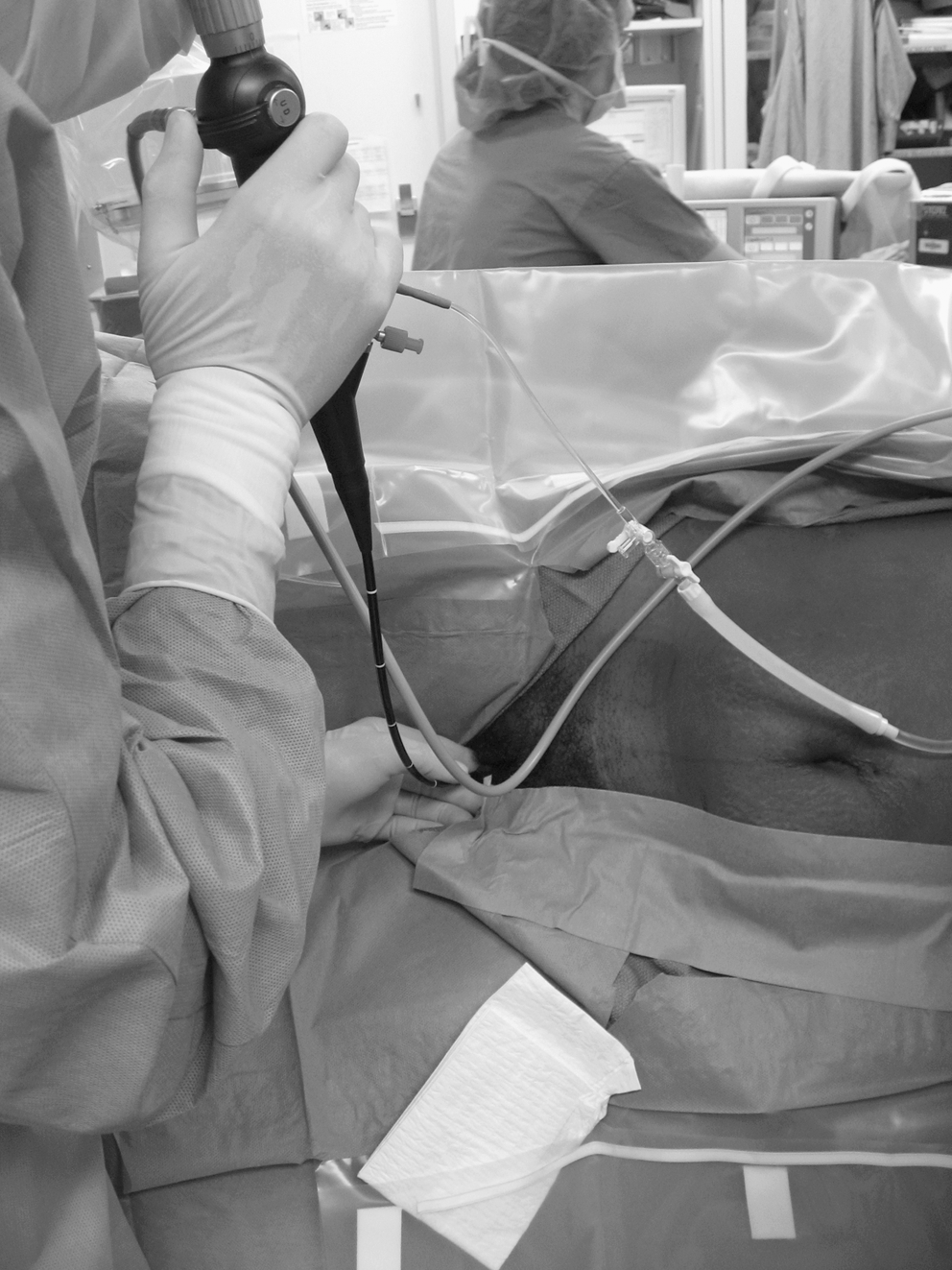
After draping, flexible cystoscopy is performed using a 5F open-ended angiographic catheter over a super-stiff guidewire into the distal ureter.

The fluoroscopic C-arm is rotated from the vertical to the horizontal axis, allowing for retrograde pyelography in the lateral position.
Standard laparoscopic pyeloplasty is performed without need for repositioning through three 5-mm ports or a “hybrid 2.5-mm trocar microlaparoscopic” approach with medial reflection of the colon along the line of Toldt, isolation of the proximal ureter, and identification of the UPJ. The ureteral catheter can be manipulated to aid in identification of the ureter as well as alter the degree of renal pelvic distention during dissection. Before dismemberment of the ureter and renal pelvis, the ureteral catheter and wire are retracted distally into the ureter to prevent involvement during incision. The wire can be subsequently extended and grasped with the laparoscopic forceps to maintain ureteral orientation and stabilization during spatulation.
After lateral spatulation of the ureter and any needed reduction of the renal pelvis, suture closure of the dependent dismembered pyeloplasty anastomosis is performed. The posterior wall anastomosis is started at the dependent lateral pelvis and the lateral caudal apex of the spatulation using a running 4-0 absorbable polyglactin suture on a RB-needle with intracorporeal knots. With a second suture, the anterior closure is begun at the lateral apex of the spatulation.
After completing approximately two-thirds of the anterior repair, attention is turned to stent placement. The Foley catheter is removed. The proximal end of the guidewire is identified in the renal pelvis, grasped, and held taut using the laparoscopic grasping forceps/needle holders; the Double-J ureteral stent is placed retrograde over the guidewire (Fig. 4). The length of the ureteral stent placed is determined based on the height of the patient.
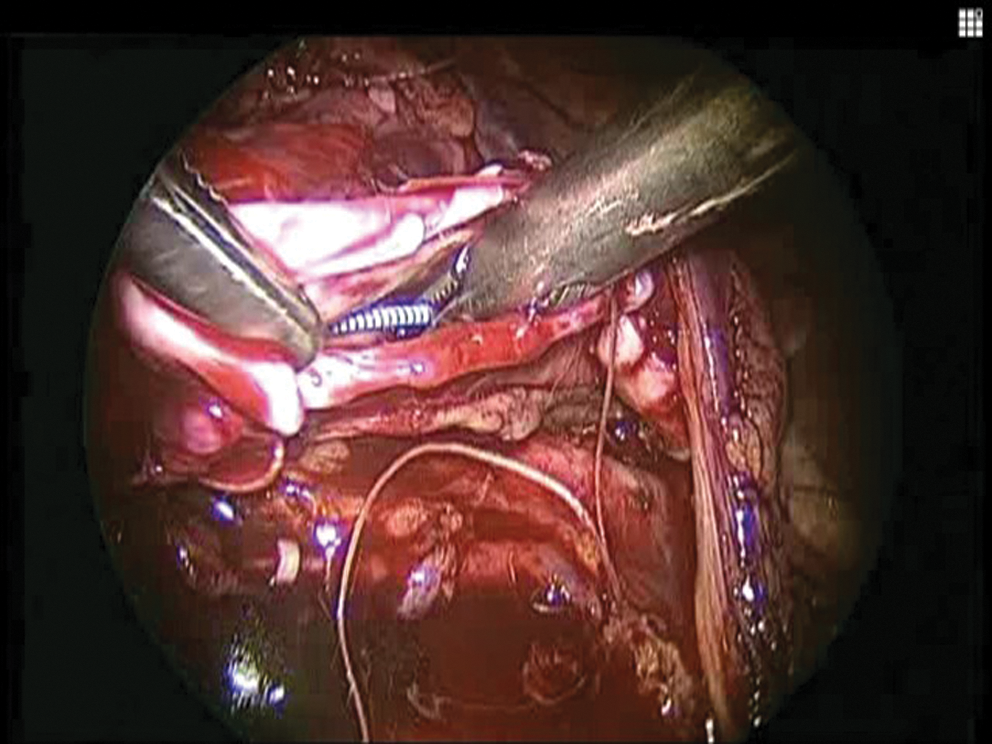
The laparoscopic surgeon holds the proximal end of the guidewire taut as a Double-J ureteral stent is placed retrograde over the guidewire under direct visualization.
The proximal aspect of the stent is visualized in the laparoscopic field entering the renal pelvis, and the proximal curl is positioned into the renal pelvis (Fig. 5). In female patients, the distal curl of the stent is created by guidance of the stent to the level of the external urethral meatus before removal of the guidewire. In male patients, the ureteral stent is advanced over the guidewire with the aid of the pusher, and flexible cystoscopy is simultaneously performed to determine the appropriate positioning of the distal curl.
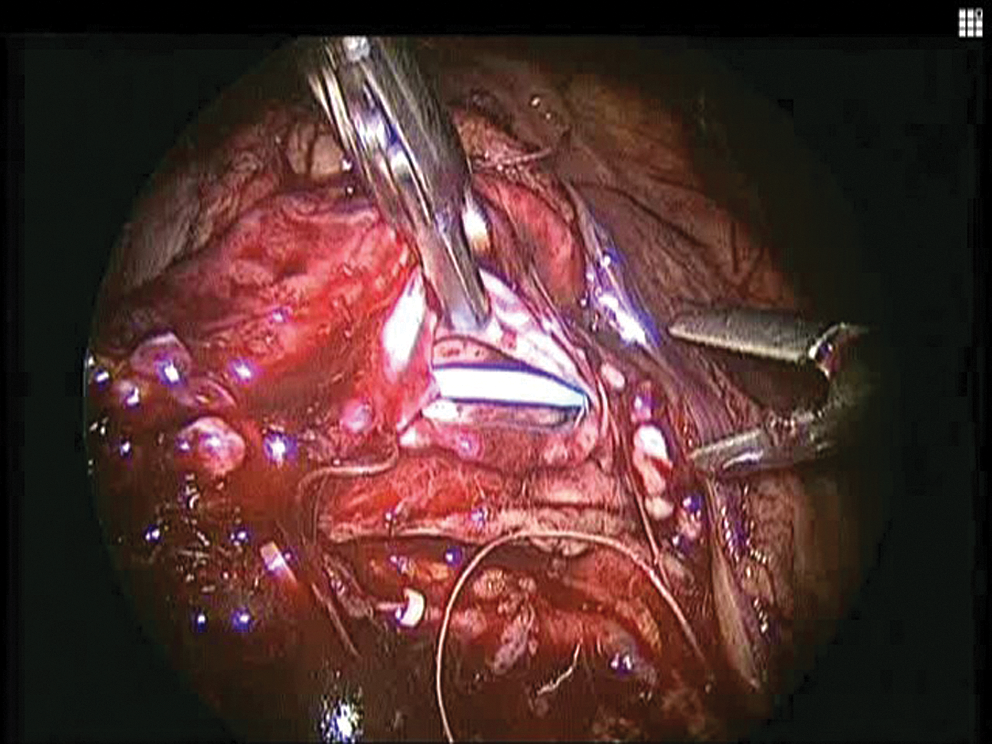
Within the laparoscopic field, the proximal curl of the ureteral stent is positioned into the renal pelvis. The distal curl is created in female patients by guidance of the stent to the external urethral meatus and using flexible cystoscopy in male patients.
Once the stent is fully positioned, the remaining portion of the anterior ureteropelvic anastomosis is completed. The line of Toldt is reapproximated to the side wall using Hem-o-lok clips (Teleflex Medical, Research Triangle Park, NC) for re-retroperitonealization of the repair. At the conclusion of the procedure, a 10F drain is placed through a trocar site, and the Foley catheter is replaced. The ureteral stent position can be confirmed using intraoperative fluoroscopy or plain abdominal radiography as needed.
Footnotes
Disclosure Statement
No competing financial interests exist.