
Abstract
Objectives:
The aim of this study was to evaluate outcomes of transperitoneal and retroperitoneal approaches in laparoscopic adrenalectomy (LA) for pheochromocytoma.
Methods:
We retrospectively compared the results of transperitoneal LA (TLA) with that of retroperitoneal LA (RLA) in 99 patients with unilateral pheochromocytoma (<6 cm in diameter). Age of patients ranged from 20 to 63 years (42 men and 57 women; 56 in right and 43 in left). The mean operation time, blood loss, mean hospital stay after operation, fluctuation range of blood pressure, blood pressure after operation, complication, mortalities, and recurrences were considered.
Results:
There were significant differences between RLA and TLA in terms of duration of surgery 84 ± 17 minutes versus 117 ± 24 minutes (p < 0.05), intraoperative blood loss 200 ± 22.5 ml versus 340 ± 41.7 ml (p < 0.05), mean hospital stay after operation 4.8 ± 1.6 days versus 7.8 ± 2.2 days (p < 0.05), and complication 12.5% versus 6.7% (p < 0.05). There was no significant difference between RLA and TLA in terms of fluctuation range of blood pressure (p > 0.05) and blood pressure after operation (p > 0.05). There were no mortalities or recurrences of tumors in all patients during follow-up.
Conclusions:
Compared with TLA, RLA is safer, more quick, and effective for patients with unilateral pheochromocytoma (< 6 cm in diameter).
Introduction
Pheochromocytoma is a rare disorder and functioning tumor composed of chromaffin cells that secrete catecholamines. Patients with a pheochromocytoma “crisis” have a high mortality despite aggressive therapy. 15,16 The effects associated with catecholamine release render LA more challenging, although with comparable morbidity to other diseases of the adrenal gland for LA. 17,18
Although LA is a promising alternative to open surgery, concerns exist with respect to laparoscopic treatment of pheochromocytoma. 19,20 It is reported that LA for pheochromocytoma is a feasible, safe, and effective treatment. 17,21 But few reports showed differences between the results of TLA and RLA in pheochromocytoma.
In this study we compare the outcome of 40 patients who underwent TLA with that of 59 patients who underwent RLA for pheochromocytoma retrospectively, particularly with respect to intraoperative hemodynamic stability, blood loss, operation time, complication, and postoperative patient comfort.
Patients and Methods of Operation
Patients
LA was first carried out in June 1996 at our department. Since 1999 to 2008, a total of 99 patients with unilateral benign pheochromocytoma <6 cm in diameter have undergone LA for pheochromocytoma. Patients with bilateral pheochromocytoma or malignancy were not included in this retrospective study. TLA for pheochromocytoma was carried out in 40 patients and RLA was carried out in 59 patients. There were three patients with Multiple Endocrine Neoplasia syndrome. There was no significant difference between the two groups in sex, age, body mass index, diameter of tumor, and side of tumor (Table 1).
Patients who underwent TLA versus patients who underwent RLA with respect to sex (p 1), age (p 2), BMI (p 3), diameter of tumor (p 4), and side of tumor (p 5). TLA = transperitoneal laparoscopic adrenalectomy; RLA = retroperitoneal laparoscopic adrenalectomy; BMI = body mass index.
Diagnosis
In our retrospective study, all patients with paroxysmal hypertension were examined. Diagnosis of pheochromocytoma relied on clinical signs associated with one or more of the following criteria: increased plasma and urinary catecholamines or their metabolites, magnetic resonance imaging scan, 64-slice spiral computed tomography scan, and iodine 131 iobenguane (iodine 131 metaiodobenzylguanidine) scan. 22,23 All 99 patients in our study underwent this serial examination. All cases were pathologically diagnosed as pheochromocytoma after operation.
Preoperative preparation for pheochromocytoma
Preoperative preparation was started 10 to 14 days before surgery. Oral phenoxybenzamine 30 to 120 mg/day was given along with infusion intravenously fluids to stabilize arterial blood pressure (<130 and 90 mm Hg, respectively) and to maintain optimum intravascular volume. Patients with tachycardia were given β-adrenergic blockers (oral metoprolol 50–100 mg) to stabilize heart rate <100 beats per minute. Patients were considered adequately prepared for surgery when they had a sense of well-being, had no paroxysms of hypertension, were euglycemic, and had a normal hematocrit. Oral phenoxybenzamine and metoprolol were continued until the day of surgery. Oral phenoxybenzamine was given in the night before and on the morning of surgery as normal dose. 24,25
Methods of operation
There were two groups of surgeons engaging in LA. One group took the method of transperitoneal approach and another group took the method of retroperitoneal approach in LA. There was no change in operative method by each surgeon. Learning curves of those two groups are shown in Figure 1.
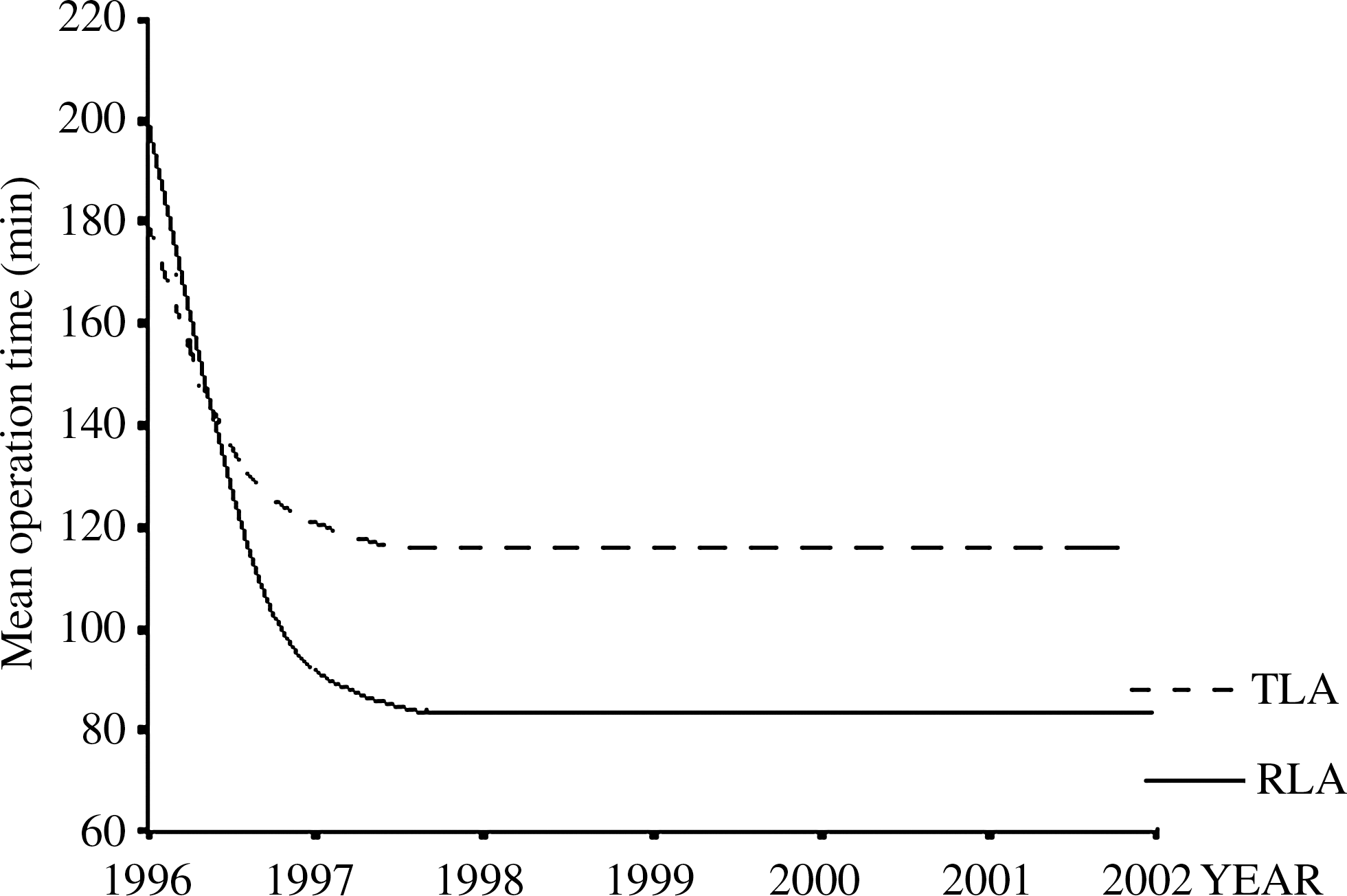
Learning curves of TLA and RLA group surgeons. TLA = transperitoneal laparoscopic adrenalectomy; RLA = retroperitoneal laparoscopic adrenalectomy.
The transperitoneal approach in LA for pheochromocytoma
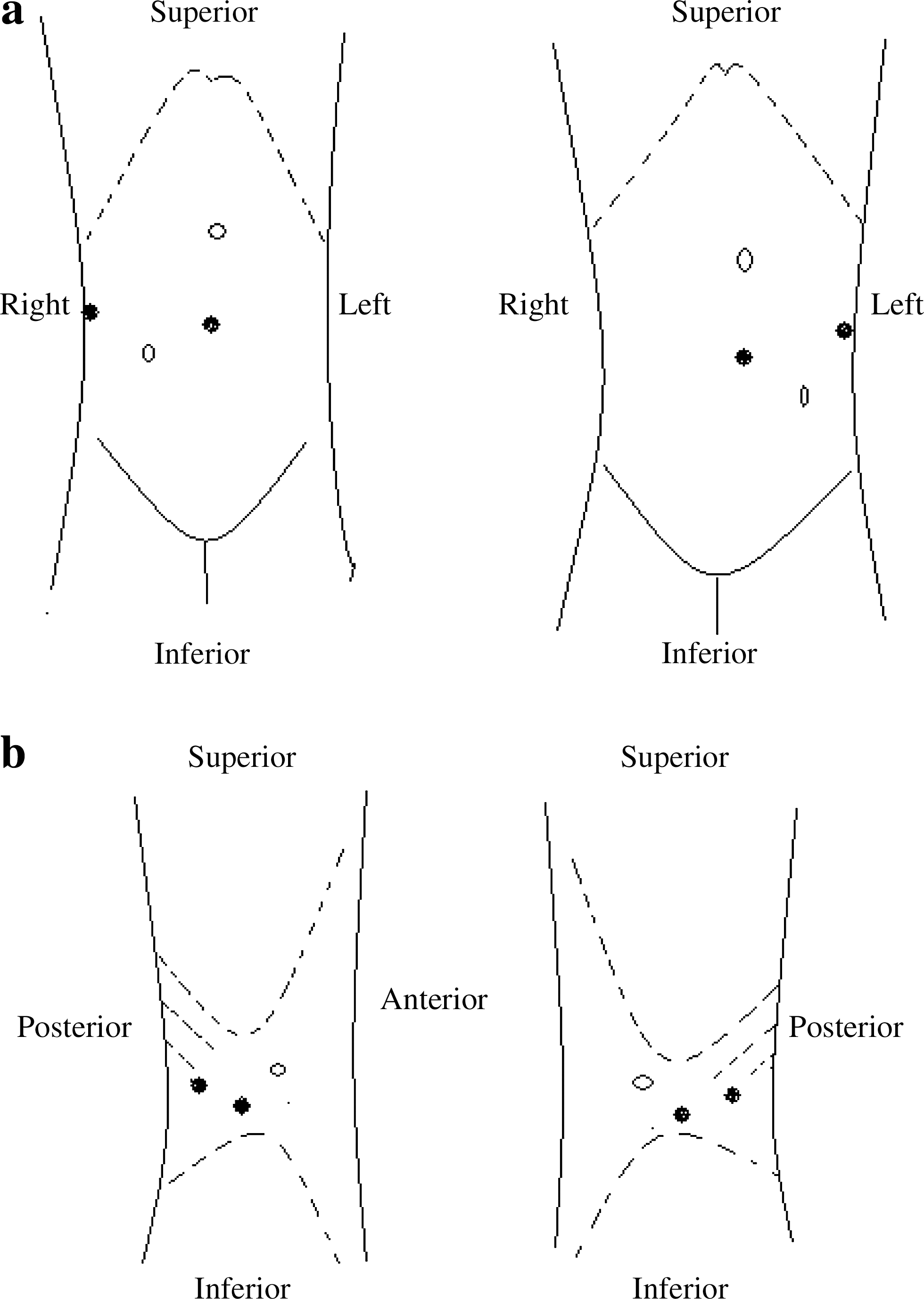
The transabdominal approach to LA was used for 40 patients with pheochromocytoma. For right adrenalectomies, a 1-cm incision was made in the anterior axillary line, and the trocar was inserted. A 10-mm, 30° laparoscope was inserted through this incision, and three other ports (midclavicular line, umbilicus, and anterior medina line) were inserted under direct visualization. A Senn retractor was used to retract the liver. Using electrocautery, the adrenal gland was exposed, and the adrenal vein was doubly clipped and divided. The remaining vessels were clipped and divided, and the gland was removed intact within a laparoscopic retrieval bag via the umbilical incision. For left-sided tumors, the procedure was similar, with the exceptions that the spleen was partially mobilized to expose the gland 26 (Fig. 2a).
(
The retroperitoneal approach in LA for pheochromocytoma
The retroperitoneal approach to LA was used for 59 patients with pheochromocytoma. For the technique of RLA, a 1.5-cm incision was performed in the midaxillary line below the 12th rib. After insufflating the retroperitoneal space with CO2, a trocar was inserted. A 10-mm, 30° laparoscope was inserted through this incision and two other retroperitoneal 10-mm trocars were inserted, respectively, below the costal margin, abdominally and dorsally, under direct vision. For right adrenalectomy, the dissection was effected along lumbar muscle to renal upper pole. Once the adrenal gland was observed, exposing it with electrocautery, the adrenal vein was doubly clipped and divided. The remaining vessels were clipped and divided, and the gland was removed intact within a laparoscopic retrieval bag via the midaxillary line incision. For left adrenalectomy, the procedure was similar 27 (Fig. 2b).
Statistics
The mean operation time, blood loss, mean hospital stay after operation, fluctuation range of blood pressure, blood pressure after operation, complication, mortalities, and recurrences were considered.
Data of levels of mean operation time, blood loss, and hospital stay after operation were expressed as mean ± standard deviation. Comparison between two groups was made by comparing means followed by one-way analysis of variance.
Data of fluctuation range of blood pressure, complication, and blood pressure after operation were expressed in distribution of frequencies. It was carried out by chi-square test and the Fischer exact analysis.
The statistical analysis was done with SPSS 11.5 statistical analysis software. p < 0.05 was considered statistically significant.
Results
The mean operation time is 84 ± 17 minutes in RLA and it is 117 ± 24 minutes in TLA (p < 0.05). It is shown that RLA takes less time in operation than TLA.
The mean blood loss is 200 ± 22.5 ml in RLA and it is 340 ± 41.7 ml in TLA (p < 0. 05). It is shown that RLA lost less blood in operation than TLA.
Mean hospital stay after operation is 4.8 ± 1.6 days in RLA and it is 7.8 ± 2.2 days in TLA (p < 0.05). It is shown that RLA takes less time in hospital after operation than TLA.
Regarding fluctuation range of blood pressure in RLA, there were 40 patients with blood pressure < 20 mm Hg, 9 patients with blood pressure 20 to 50 mm Hg, and 10 patients with blood pressure > 50 mm Hg. There were 27 patients with blood pressure < 20 mm Hg, 8 patients with blood pressure 20 to 50 mm Hg, and 5 patients with blood pressure > 50 mm Hg in TLA. There was no statistically significant difference between the two groups of patients who underwent RLA and TLA (p > 0.05).
All cases were followed up from 6 to 36 months. Postoperative blood pressure was normal at 2 months for 41 of 59 patients who have undergone RLA and for 27 of 40 patients who have undergone TLA. There was no statistically significant difference between two groups of patients who have undergone RLA and TLA (p > 0.05).
There were five cases with complication in patients who underwent TLA (two cases of pneumothorax, one case of colon injury, one case of spleen injury, and one case of hematoma) and four cases with complication in patients who underwent RLA (two cases peritoneum injury, one case of pleura injury, and one case of retroperitoneal hematoma). There were more cases with complication in patients who underwent TLA than in patients who underwent RLA (p < 0.05).
We followed up by examination of plasma and urinary catecholamines or their metabolites, magnetic resonance imaging scan, or 64-slice spiral computed tomography scan. During the follow-up for 6 to 36 months (mean: 21.3 months) in 99 cases, there were no mortalities or recurrences of tumors in all patients who underwent RLA or TLA for pheochromocytoma (Table 2).
Patients who underwent TLA versus patients who underwent RLA with respect to operation time (p 1), blood loss (p 2), hospital stay after operation (p 3), fluctuation range of blood pressure (p 4), and complication (p 5).
Discussion
LA has been reported as the gold standard treatment for adrenal masses in many studies. LA can be safely and effectively performed in patients with pheochromocytoma. The advantages of low morbidity, fewer complications, shorter operation time, less blood loss, and quick recovery, along with cure of hypertension and lack of hormonal recurrence, make LA a preferable option in patients with pheochromocytoma. However, it is wise to consider a traditional open operation when the mass is large, adherent, and hypervascular and has retrocaval extension. 17 Retroperitoneal and transperitoneal approach LA is the most popular technique used for pheochromocytoma.
Transperitoneal approach LA for pheochromocytoma
The transperitoneal approach is being used first and is still the most popular technique as it provides more ample working cavity, greater visibility, and better instrument mobility in LA. 28 It is easy to learn and maneuver. By this approach, it is easy to localize the adrenal and mass, control center vein of the adrenal, clip, and divide it.
But there are some complications in transperitoneal approach LA for pheochromocytoma. It can arouse complication of abdominal organs with interference of the intraabdominal organs. It may take longer time in operation than retroperitoneal approach. It can cause trauma of liver and pancreas in course of operation.
Retroperitoneal approach LA for pheochromocytoma
The retroperitoneal approach offers the advantage of dissection without the interference of the intraabdominal organs, avoiding the respiratory and hemodynamic effects of CO2 pneumoperitoneum and giving direct access without the need to mobilize abdominal organs. It rarely causes complication of abdominal organs as the interference of the intraabdominal organs is avoided. For direct access without maneuver in the peritoneal, it may take less time in operation than transperitoneal approach.
However, with this technique, it is difficult to create a retroperitoneal space for insertion of trocar and the laparoscopic surgeon does not have the anatomic landmarks to proceed with the dissection. In addition, the working space is restricted. 27
Comparison between retroperitoneal and transperitoneal approach LA for pheochromocytoma
As discussed earlier, for unilateral pheochromocytoma <6 cm in diameter, retroperitoneal approach LA for pheochromocytoma showed the advantages of less operation time, less blood loss, shorter hospital stay after operation, and less complication than transperitoneal approach of LA for pheochromocytoma. As fluctuation range of blood pressure, blood pressure after operation, mortalities, and recurrences were considered, there was no statistically significant difference between retroperitoneal and transperitoneal approach of LA for pheochromocytoma. So, although it is difficult to learn, compared with transperitoneal approach of LA for pheochromocytoma, retroperitoneal approach of LA is a safer, more quick, and effective treatment in patients with pheochromocytoma.
Conclusion
Retroperitoneal approach of LA is safer, more quick, and effective than TLA for patients with pheochromocytoma.
Footnotes
Acknowledgment
The authors thank all members of the Urology Department of First Affiliated Hospital of Binzhou Medical University for their work on LA from 1996.
Disclosure Statement
No competing financial interests exist.