
Abstract
Purpose:
To assess the long-term outcome of early endoscopic realignment (EER) of complete posterior urethral disruption.
Patients and Methods:
The study included 11 consecutive patients with complete posterior urethral disruption secondary to a road accident (n = 9) or a falling impact (n = 2). EER was performed using a simultaneous endoscopic transvesical and transurethral approach under fluoroscopic guidance. An 18F Foley urethral catheter was left for 4 weeks. All patients were evaluated postoperatively for incontinence, erectile dysfunction, and urethral strictures.
Results:
The patients' mean age was 32 years (range 20–62 y). The mean duration of the realignment procedure was 40 minutes (range 30–60 min), and it was performed within an average of 48 hours (range 3–72 h) from hospitalization. Efficient erection was maintained in five (45%) patients, and incontinence did not develop in any patient. Five (45%) patients in whom urethral strictures developed were treated initially by endoscopic urethrotomy (EU), which was successful in one patient. Three of the four in the EU failure group remained on periodic urethral dilation, refusing to undergo urethroplasty, and one patient with interposition of a pubic bone fragment underwent successful urethroplasty. There were no other complications during a mean follow-up of 4.3 years (range 2–7 y).
Conclusions:
EER is a valuable alternative to long-term suprapubic drainage and delayed urethroplasty. Realignment failure did not interfere with the results of open urethroplasty. A further search for prognostic factors should improve the selection of patients for the early or the delayed approach.
Introduction
Patients and Methods
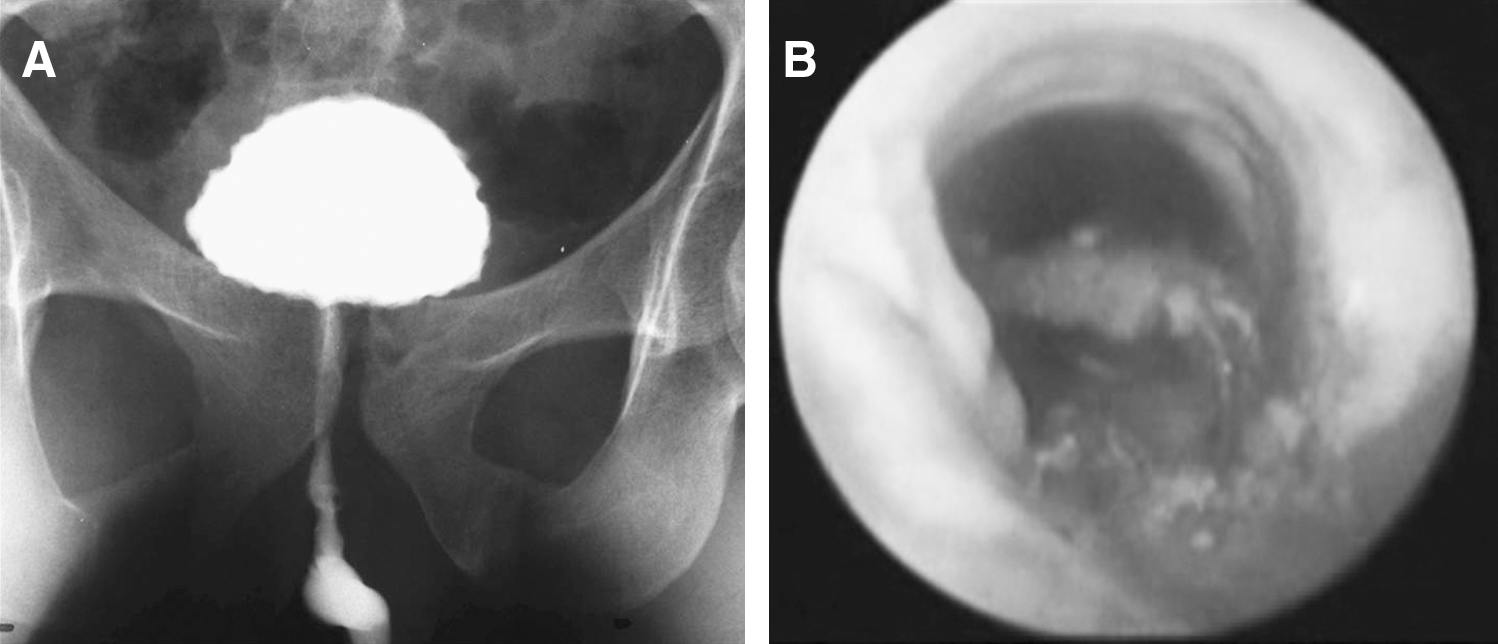
The study included 11 consecutive patients who presented with grade III complete posterior urethral disruption and who were treated by EER. 7 Their mean age was 32 years (range 20–62 y). The posterior urethral ruptures were caused by a motor vehicle accident (n = 9) or a fall impact (n = 2). Patients were approached on presentation according to the advanced trauma life support principles. 8 Following initial survey, care, and stabilization, CT scans and complementary radiographic studies that specifically addressed the affected anatomic sites were performed. Posterior urethral injuries were suspected based on clinical signs, and they were confirmed by retrograde urethrography and antegrade cystography (Fig. 1).

Combined simultaneous transvesical cystography and retrograde urethrography: (
The posterior urethral realignment was performed under general anesthesia after stabilization of other life-threatening injuries. Flexible 15F cystoscopes were simultaneously introduced transurethrally and transvesically under fluoroscopic multiplanar guidance. The transurethral scope was advanced to the distal edge of the disruption, while the transvesical scope was used to pass a guidewire through the bladder neck into the retropubic space. The cystoscopes were gradually advanced toward each other to enable endoscopic-controlled passage of a guidewire through the disrupted urethral segment down to the urethral orifice. An 18F Councill catheter was railroaded on the guidewire into the bladder and left for 4 weeks (Fig. 2).

Fluoroscopic aspects of early endoscopic realignment: (
Urethral patency and functionality were evaluated by retrograde urethrography performed immediately after removal of the catheter (Fig. 3) and by flowmetry and urinary residual scanning every 3 months thereafter. Erectile function was evaluated by the International Index of Erectile Function questionnaire, 9 and continence by anamnestic and physical assessment.
Retrograde urethrography 4 weeks after early endoscopic realignment: (
Results
On presentation, all patients failed to pass urine, six (55%) exhibited bloody discharge from the urethral meatus, and eight (73%) had pathognomonic butterfly-shaped perineal hematoma. A floating prostate on digital rectal examination and pelvic bone fractures on imaging assessment were found in all cases. Urethral catheterization was attempted in four (36%) patients, but it failed. Emergency department bedside retrograde urethrography that was performed in these four patients revealed posterior urethral disruption, and percutaneous suprapubic cystostomy was performed. Seven (64%) patients underwent urgent interventions (surgical, orthopedic, ophthalmologic, etc.) to achieve hemodynamic stability and intra-abdominal damage control. Primary open cystostomy was performed in these patients during the laparotomy (Table 1).
MVA = motor vehicle accident; PEF = pelvic external fixation; ED = erectile dysfunction.
The realignment was accomplished in an average of 48 hours (range 3-72 h) from hospitalization, and it was associated with complementary orthopedic interventions in four (36%) patients. The average time of the intraoperative urethral manipulation was 40 minutes. There were no complications that were related to the procedure.
Continence was maintained in all patients. Erectile function was preserved in five (45%) patients. Statistical analysis revealed no significant correlation between postoperative erectile function and time to surgery, age, and associated injuries (P > 0.05) (Table 1).
Urethral strictures developed in five (45%) patients. The length of the stricture was shorter than 5 mm in three patients and measured an average of 15 mm (10–20 mm) in two patients (Table 1). Strictures occurred within an average period of 8 months (range 3–12 mos) since the traumatic event. These five patients were treated initially by holmium laser urethrotomy, which was successful in one (20%) patient. Open urethroplasty was recommended in the other four patients: three refused, preferring to remain on periodic urethral dilation, and one of the three regained permanent urethral patency after 1 year of periodic dilation. One patient with a pelvic bone interposing fragment underwent successful open urethroplasty.
There were no other complications during a mean follow-up of 4.3 years (range 2–7 y).
Discussion
Most posterior urethral injuries are caused by blunt trauma that is associated with a pelvic fracture or straddle injury. The mechanism of these injuries involves major shearing forces at the prostatomembranous junction, resulting in avulsion of the urethra from the fixed urogenital diaphragm. Other potential mechanisms of posterior urethral injury are shearing forces between a fixed prostate and a mobile bladder, resulting in bladder neck injury and direct laceration by pelvic bone fragments or urethral distraction/compression between the symphysis and pubic rami. 3 Cadaver studies suggest that the prostate, membranous urethra, and urethral sphincter are one anatomic unit, and so urethral disruption may also occur at the bulbomembranous junction. 6,10,11
The intensity and complexity of the impact that causes pelvic fracture and urethral injuries are often so great that these injuries are typically associated with multiple organ injuries (including spleen, liver, and bowel), and have mortality rates as high as 30%. 3 After resuscitation and management of life-threatening associated injuries, the first step in the management of the injured urethra is bladder drainage to avoid further soft-tissue infiltration by urine and to allow urinary output monitoring.
The definitive management options include primary suture repair, primary surgical or endoscopic realignment, and suprapubic cystostomy with delayed repair (SCDR). 1 Their aim is to reestablish urethral continuity while maintaining continence and sexual function. The historic approach of pelvic exploration and primary repair was associated with significant complications, including bleeding from disruption of contained pelvic hematoma, infection, aggravation of the initial urethral injury, and high rates of incontinence and erectile dysfunction. 1,12 Today, this approach is reserved only for rare cases of bladder neck laceration (grade IV injury) associated with severe dislocation of the prostatomembranous urethra, and pelvic vascular or rectal injury. SCDR has been the general standard of care for posterior urethral disruption since the late 1970s. While it provides better continent and erectile functionality compared with primary suture repair, it does have the drawback of a 97% to 100% rate of urethral stricture formation necessitating complex reconstructions. 1,4,6
The concept of immediate surgical realignment was described in the early 1930s, 13 but it gained popularity only some 50 years later when it was shown that, in comparison with delayed repair, realignment provides equivalent or better outcome without the need for multiple surgical procedures. 6,14 –16 The introduction of endoscopic instrumentation significantly reduced the invasiveness of the treatment. It avoids the risks that accompany complex open urethral manipulations while preserving its advantages of reducing stricture rates, shortening the time to spontaneous voiding, and eliminating the morbidity that is associated with suprapubic cystostomy. 3 –5
In a series of 29 patients with urethral disruption, Moudouni and associates 17 demonstrated that EER was associated with minimal morbidity, and the failure of endoscopic realignment did not compromise delayed urethral reconstruction. It should be noted that this relatively large series of patients with long-term follow-up included six patients (21% of the total) with partial disruption, a percentage that could have positively influenced the overall outcome.
In a recent study, Hadjizacharia and colleagues 4 compared their experience with EER performed by a retrograde transurethral approach with SCDR following a crossover algorithm, aimed to initially perform EER in all patients. This study comprised a hybrid series of 21 patients with complete (N = 7; 33%), partial (N = 14; 67%), anterior (N = 11; 52%) and posterior (N = 10; 48%) urethral disruptions. The authors were able to perform EER in 14 (78%) of the candidates for realignment. The stricture rate for the EER and SCDR groups was 14% and 100%, respectively (P < 0.001), and all patients referred for delayed repair underwent urethroplasty 6 ± 3 months after the trauma. Although limited by the study design and the patients' clinical characteristics, this study concluded that, in comparison with the traditional SCDR approach, EER resulted in a markedly reduced time to spontaneous voiding and a lesser risk of urethral stricture, decreasing the need for surgical urethroplasty and long-term suprapubic urinary diversion.
Another significant concern after urethral disruption is the risk of erectile dysfunction occurrence. Several series on posterior urethral injury clearly support the etiology as being the injury itself and not the method chosen for management of this complication. 3,16 A number of studies showed that when compared with SCDR, immediate surgical urethral realignment and EER result in equivalent or better erectile function preservation. 4,6,15,16
Our series included only complete, grade III, posterior urethral disruptions, which are more complex and severe than those reported in the above citations. 4,17 Our 100% success rate with EER was probably because of the simultaneous transurethral and transvesical approach with the aid of multiplanar fluoroscopy. As is well known, the most expected and troublesome complication related to these kinds of injuries is the occurrence of a urethral stricture. While this, indeed, occurred in 45% of our cohort, one patient responded well to holmium laser urethrotomy, and another regained permanent urethral patency after urethrotomy and 1 year of periodic dilations.
Interestingly, most of the patients with urethral strictures in whom urethrotomy failed refused to undergo open urethroplasty, preferring to continue periodical urethral dilation. This should sound an alarm for the physician about the advisability of asking the patient for his agreement to undergo SCDR in the acute state when, most likely under sedation and on assisted ventilation, he is unable to consider treatment options.
In our opinion, all patients should initially be offered EER, because our experience and that of others has demonstrated that failure of EER does not affect the success of an eventual open urethroplasty. 4,17 In view of some reports that previous failed railroading or urethral manipulation may significantly decrease the success of subsequent anastomotic urethroplasty in the strictured urethra, 18 and the fact that EER can be performed up to a few days after the injury, patients should be referred to urologists who are proficient in the procedure and who have the requisite instrumentation.
There is some concern that endoscopic attempts at realignment may induce or predispose the pelvic hematoma to infection as a result of irrigation. We did not encounter such a complication and, to the best of our knowledge, it has never been reported in the literature. 3 Moreover, suprapubic tubes can compromise anterior exposure for internal fixation of the pelvis and may increase the rate of pelvic infection. 19 There is evidence to show that EER of posterior urethral injuries that are associated with pelvic fractures, particularly acetabular fractures, should be attempted to avoid the increased morbidity that is associated with conservative management of the concurrent orthopedic injuries. 20
Conclusions
Based on the success of early EER in our study, we conclude that this procedure offers a valuable alternative to SCDR. Realignment failure did not interfere with the results of open urethroplasty at a later date. A comparative analysis of the prognostic factors related to the two approaches should help in determining which patients are most suitable for the early and the delayed approaches.
Footnotes
Disclosure Statement
No competing financial interests exist.