
Abstract
Background and Purpose:
Fibrotic or neoplastic obstruction of the terminal ureter and ureterovesical junction can preclude internal drainage with a Double-J catheter. Some minimally invasive alternatives are described in the literature to avoid a percutaneous nephrostomy. We present a pure endourologic technique.
Patients and Methods:
In six patients with an obstructed upper urinary tract, after the introduction of iodine contrast, the ureter was punctured with a needle to introduce a guidewire in the urinary tract under cystoscopic and fluoroscopic control. The alternative path between the bladder and ureter was then dilated up 10F to facilitate the Double-J catheter introduction.
Results:
All six patients had their obstructed urinary tract drained with a Double-J catheter inserted above the level of obstruction. No complication was verified.
Conclusion:
Internal urinary tract drainage with a Double-J catheter was accomplished using endourologic principles in six patients, avoiding a percutaneous nephrostomy or other more invasive procedures.
Introduction
We propose a cystoscopic technique of insertion of the Double-J catheter in patients in whom the catheter could not be inserted either by the ureteral orifice or by percutaneous renal access. The new path between the bladder and ureter, above the obstruction, avoids the bothersome nephrostomy tube or other more invasive kinds of drainage.
Patients and Methods
Six patients with an obstructed upper urinary tract underwent the procedure. The patient received general or regional anesthesia and was placed in the position proposed by Valdivia-Uria for combined percutaneous and ureteroscopic procedures (lithotomy position with the body at a 20-degree oblique angle, with the side to be treated elevated). 3
The urinary tract was contrasted antegradely with iodine injected by a renal puncture under fluoroscopic control. Occasionally, the urinary tract could be contrasted retrogradely by a ureteral catheter or intravenous injection.
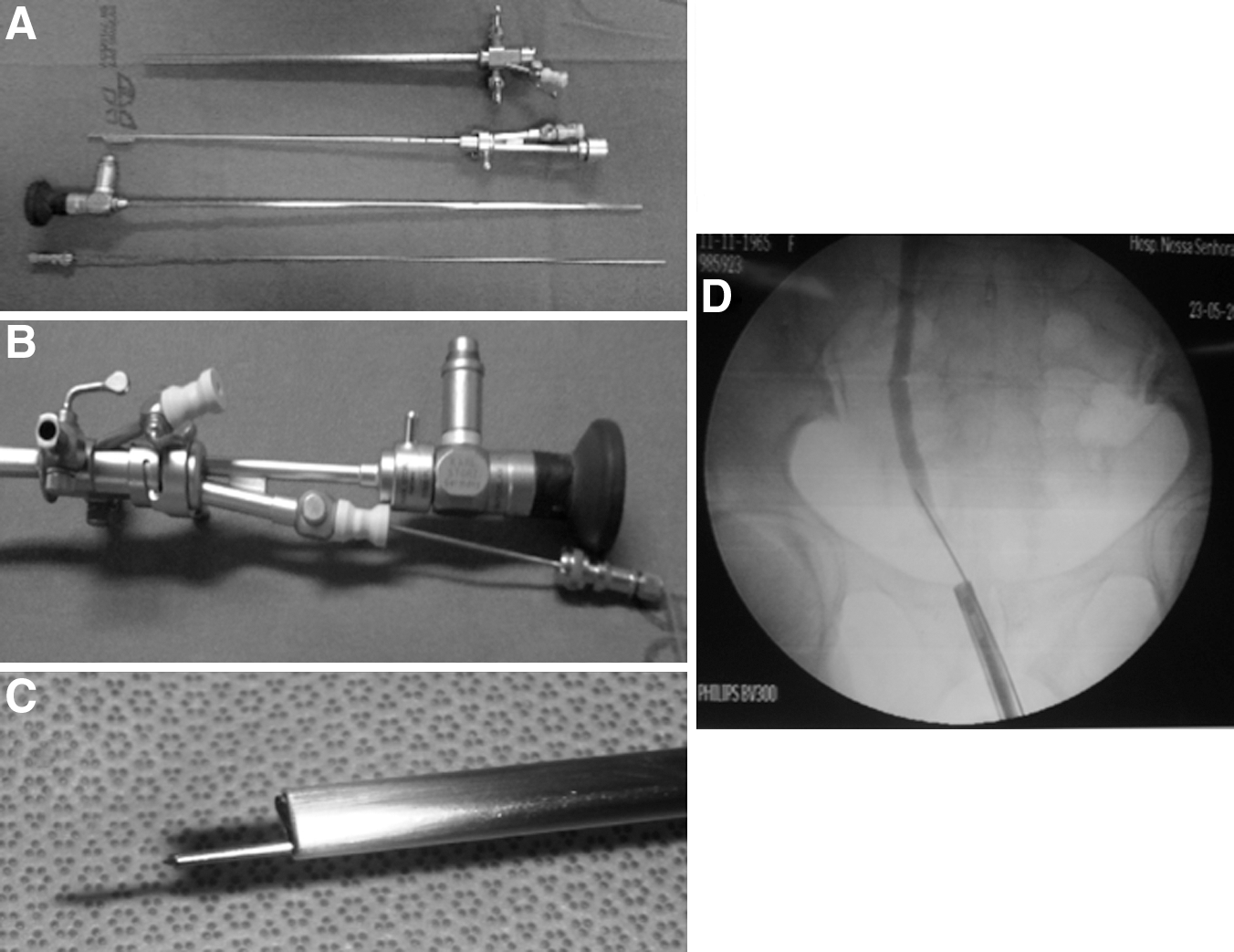
After filling the bladder with saline, an 18-gauge needle, 35 cm in length, (Russer Brasil Ltda, Indaiatuba, Sao Paulo, Brazil) was introduced into the bladder along the Sachse urethrotome through the bridge generally used for laser fiber (Karl Storz GmbH & Co. KG, Tuttlingen, Germany) (Figs. 1 and 2). Under fluoroscopic and cystoscopic orientation, the needle reached the ureteral lumen through the bladder wall and above the obstruction, confirmed by drops of urine from the needle. In sequence, a 0035” guidewire was introduced, and the pathway was dilated up to 10F with a fascial ureteral dilator (Karl Storz GmbH & Co. KG, Tuttlingen, Germany) (Fig. 3) before Double-J catheter introduction and its position fluoroscopically confirmed. A Foley catheter was left in place for 24 hours.

Results
The clinical parameters of the patients who underwent endoscopic stented ureterocystostomy and follow-up are shown in Table 1. The transvesical insertion of a Double-J catheter was successful in all patients. Patients with a previous nephrostomy had it removed at the end of the procedure. No complication was verified.
DJ = Double-J catheter; RUC = right ureterocystostomy; LDJ = left ureter Double-J; LFU = left urinary tract follow-up.
Discussion
Independent of the etiology, obstruction of the terminal ureter and/or ureterovesical junction can severely compromise the renal function of one or both kidneys. Urinary drainage is necessary for pain relief, to reduce the risk of infection, and, above all, to restore adequate renal function.
Generally. such obstructions are acute situations, and the two more frequent techniques of drainage are ureteral catheterization and percutaneous nephrostomy. 2,4,5 Both offer safe and efficient urinary drainage. 2,5 Percutaneous nephrostomy, however, is considered the second option after unsuccessful internal catheterization. 4
When the ureteral orifice can be recognized during cystoscopy, retrograde insertion of a Double-J catheter is tried initially. When the guidewire does not progress upward, another possibility is a percutaneous antegrade attempt to insert a guidewire and the Double-J catheter. If for any reason the Double-J catheter cannot be inserted, generally a nephrostomy tube is the minimally invasive alternative for preserving renal function.
The nephrostomy has a negative impact on patient quality of life. It is uncomfortable for the patient and, in addition, can be associated with infection, 1 obstruction, or accidental removal. In this situation, the patient needs a new percutaneous nephrostomy tube insertion with its inconvenience and costs.
Other invasive procedures are ureterovesical reimplantation, with or without antireflux mechanism, using or not using the psoas muscle fixation of the bladder, or a bladder patch. Transuretero-uretero anastomosis may be considered as another surgical alternative for unilateral obstruction.
The cystoscopic incision of bladder and ureter followed by a Double-J catheter insertion was first described in a renal transplant recipient with an ureterovesical junction stricture. 6 A combined antegrade and retrograde approach was used for cystoscopic ureteral meatotomy. 7 Miskowiak 1 proposed the transurethral ureterocystostomy, performed by direct vision using resectoscope and Colling knife in combination with fluoroscopic radiographic control.
Similarly, we propose a technique that creates a bypass above the obstruction, between the bladder and the ureter, maintained by a Double-J catheter that drains the urine from the upper urinary tract to the bladder. A Double-J catheter with a longer retention life should be chosen to reduce its exchange needs. Different from minimally invasive previous internal drainage procedures described, the technique proposed is totally endourologic, making cystoscopic knives or scissors unnecessary. Cystoscopy and fluoroscopy orient the needle puncture, dilation up to 10F, and the introduction of the Double-J catheter.
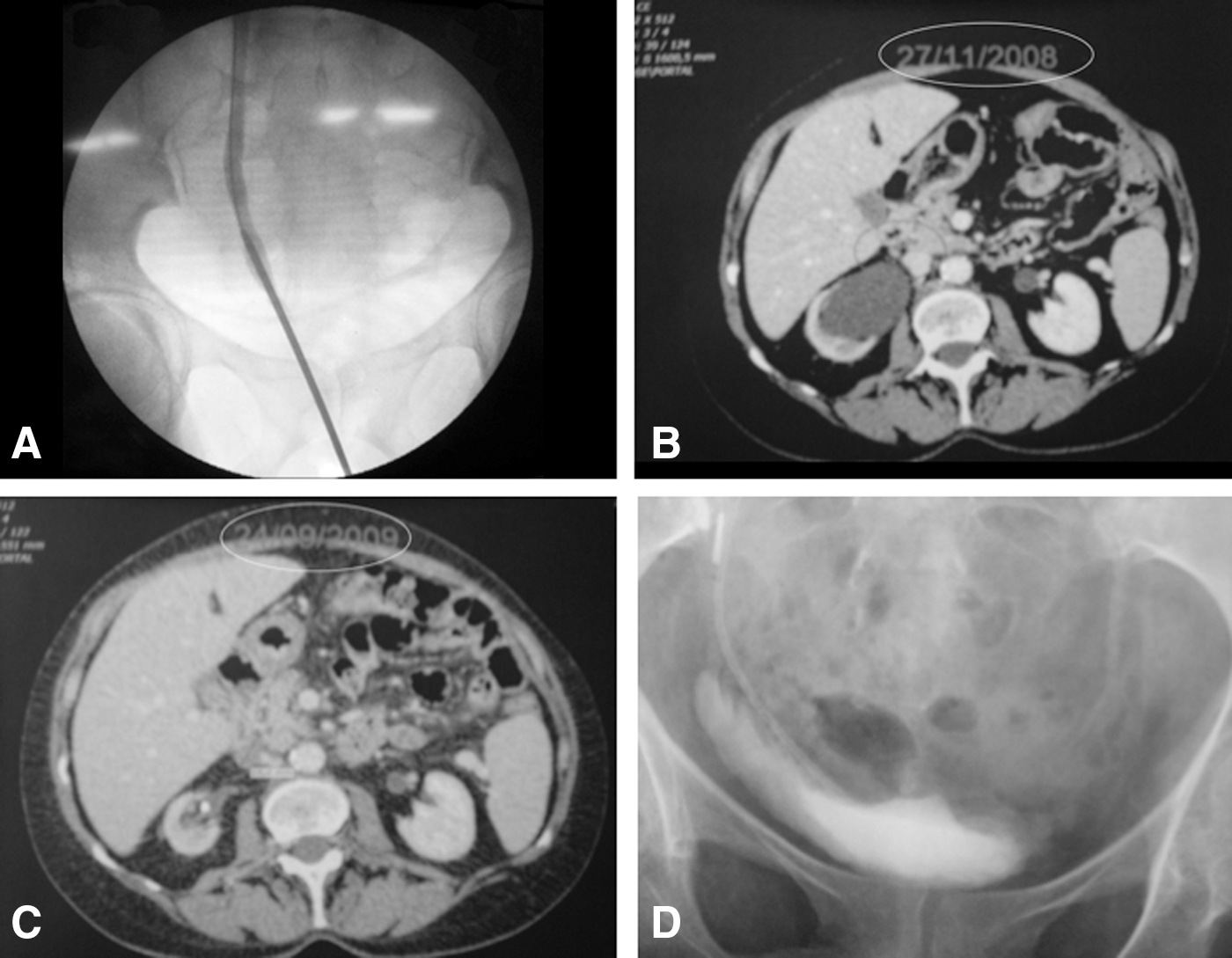
The contiguity of the distal ureter to the bladder is a necessary condition and observed when the bladder is filled with saline that may explain the undetectable extravesical collection of urine or blood (Fig. 1A). 6
Coincidentally, in all patients, the side of the urinary tract affected was the right side. Results for the left urinary tract side obstruction are still to be verified.
Endoscopic lateral view equipment with a linear work channel (cystoscope or nephroscope) may be an equipment alternative. A plastic sheath that is designed for insertion of the second guidewire during percutaneous surgery, when introduced into the bladder parallel to the cystoscope, may represent an alternative for the introduction of the needle in women.
A more extensive experience is necessary to confirm the initial results and to compare the results on both sides and in both sexes.
Conclusion
A purely endourologic procedure was described and successfully used to relieve ureterovesical obstruction, therefore avoiding a nephrostomy or other more invasive urinary drainage techniques.
Footnotes
Disclosure Statement
No competing financial interests exist.