
Abstract
Purpose:
The purpose of this study was to present our initial clinical experience with laparoendoscopic single-site surgery (LESS) for ureteropelvic junction (UPJ) obstruction.
Patients and Methods:
Between May and October 2009, 14 consecutive patients underwent LESS-pyeloplasty (LESS-P) by the same surgeon at our institution. All patients underwent single port transperitoneal Anderson-Hynes laparoscopic dismembered pyeloplasty using the single incision laparoendoscopic surgery port, inserted through a transumblical incision. Ultrasonography, intravenous urography (IVU) or diuretic renal scan was performed at the third month and semiannually thereafter. Patients were examined clinically every 3 to 6 months, depending on the symptoms. Radiographic success was defined as improvement of hydronephrosis with a patent UPJ on IVU, or improved drainage on diuretic renal scan.
Results:
Anterior crossing vessels, high insertion, and severe adhesion were found in seven (50%), five (35.7%), and two (14.3%) cases, respectively. The mean operating-room time, which includes cystoscopy with retrograde ureteral catheterization and open-end stent placement, was 204.5 minutes (range 160–300 min), and the mean estimated blood loss, including urine, was 102 mL (range 80–170 mL). Mean hospital stay was 2 days (range 1–3 d). Wound infection occurred in one patient. The mean follow-up period was 6.2 months (range, 3–8 mos). The success rate was 100%.
Conclusion:
With the advent of the single port and laparoscopic instrument technology, the LESS-P, as minimally invasive surgery, would take the place of the standard laparoscopic pyeloplasty, and it may be a new choice for the management of UPJ obstruction.
Introduction
There has been a trend toward minimizing the number of incisions and ports needed, and this has led to the description of laparoendoscopic single-site surgery (LESS). There are theoretical advantages to this approach, including less postoperative pain, a faster convalescence period, and better cosmesis. In the published literature, various terms have been used for this procedure, but the LESS Consortium for Assessment and Research coined the term LESS as acceptable for all single-incision procedures to avoid confusion with multiple terminologies. 4 Since the initial report of single-port nephrectomy in 2007 by Rane and associates, 5 single-port laparoscopic procedures, such as donor nephrectomy, 6 pyeloplasty, 7 and ureterolithotomy, 8 have been performed.
The first LESS-pyeloplasty (LESS-P) was described in 2008 by Desai and colleagues. 7 Recently, a study that compared LESS-P with conventional laparoscopic pyeloplasty has been reported. 9 Tracy and coworkers 9 reported, following their comparative study, that LESS-P was feasible and that all the perioperative outcomes were similar to those of conventional laparoscopic pyeloplasty.
The purpose of the present study was to present an initial experience, representing 14 LESS-Ps with a mean follow-up time of 6.2 months, and to better define potential benefits of LESS-P.
Patients and Methods
Patient selection
From May to October 2009, 14 LESS-P procedures were performed by an experienced laparoscopic surgeon (VT). Patients included 10 men and 8 women aged 19 to 65 years (mean age, 39 y). UPJ obstruction was right sided in 9 patients and left sided in 5 (Table 1). All patients had radiographic evidence of UPJ obstruction on diuretic renography, or of hydronephrosis with delayed function on excretory renography in conjunction with deterioration of renal function or appropriate clinical signs or symptoms. All patients had surgery after obtaining İnstitutional Review Board approval from the ethical committee and informed patient consent.
Unless otherwise indicated.
Surgical procedures
At the beginning of the procedure, all patients underwent cystoscopy with retrograde ureteral catheterization to more precisely define the stricture length and location and rule out obstruction distal to the UPJ. After retrograde open-end stent placement was performed cystoscopically, this stent was attached to a Foley catheter that was inserted into the bladder. All procedures were carried out transperitoneally under intubated general anesthesia.
The LESS-P procedure was performed with the patient positioned in a 45-degree flank position for transperitoneal surgery. A 2-cm semilunar-shaped skin incision was concealed completely within the umbilicus (Fig. 1) and deepened to the anterior rectus fascia, where a 2.5-cm midline fascial incision was made, the peritoneum was incised, and the single incision laparoendoscopic surgery (SILS™) Port (Covidien, Norwalk, CT) was deployed. The SILS Port was placed into the peritoneal cavity with the help of a clamp (Fig. 2). Then, pneumoperitoneum was established.
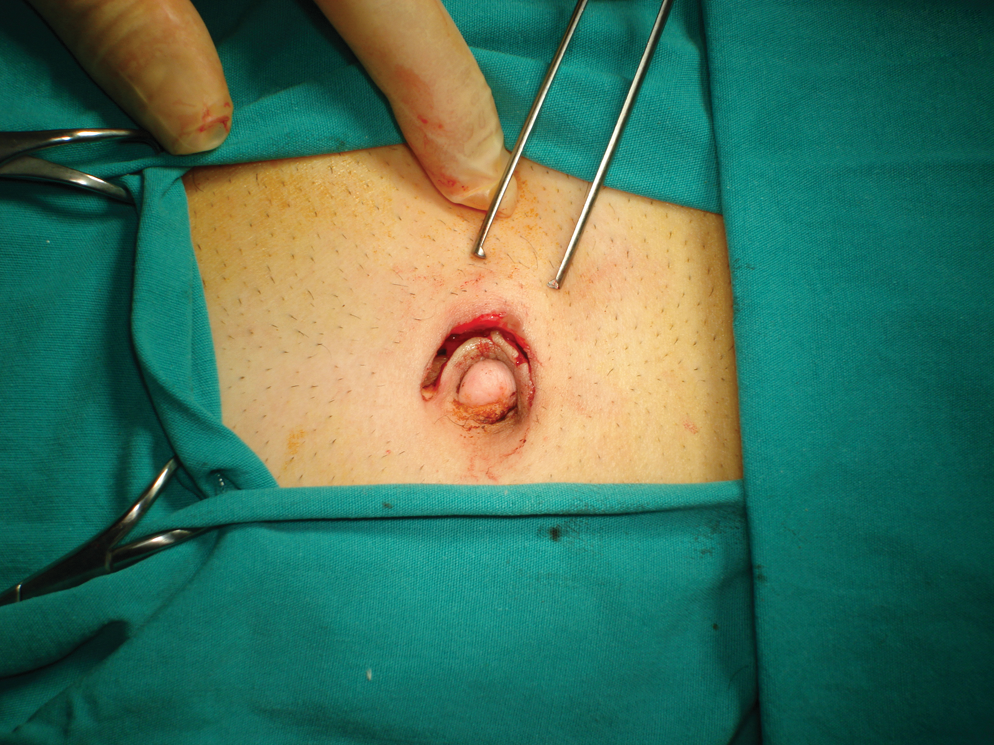
2.5-cm semilunar-shaped umblical skin incision.

The SILS Port was placed into the peritoneal cavity with the help of a clamp.
The instruments were inserted through one of the 5-mm channels and the 12-mm channel of the SILS Port. A 5-mm 30-degree high-definition rigid laparoscope with an integrated camera (Karl Storz, Tuttlingen, Germany, or Gimmi, Tuttlingen, Germany) was used along with two working instruments. During the procedure, a combination of flexible forceps and scissors (Cambridge Endoscopic Devices, Cambridge, MA, and Tyco Healthcare Group, LP) and conventional laparoscopic (straight) instruments (eg, scissors, ultrasound scissors, bipolar forceps) were used to perform the procedures as necessary.
The dissection was began by mobilizing the colon on the affected side medially by incising along the avascular line of Toldt. The straight instrument in the left hand was used to dissect the tissue while the peritoneal incision along the line of Toldt was performed with a roticulating laparoscopic scissor hold in the right hand (Cambridge Endoscopic Devices, Cambridge, MA). After the Gerota fascia was opened, dissection was carried down to the level of the kidney. The adventitia around the proximal ureter and UPJ was cleared. After complete laparoscopic mobilization of the UPJ, the renal pelvis and the proximal ureter were brought out to the abdominal wall by hitching the redundant pelvis.
A standard Anderson-Hynes dismembered pyeloplasty was performed. The strictured region was excised sharply. The ureter was spatulated on its lateral aspect, and if necessary, the redundant renal pelvis was excised. The excision of strictured region and the ureteral spatulation were performed using a roticulator scissors (Fig. 3). When UPJ obstruction was caused by a crossing vein or small artery, the vessel was dissected free. If the crossing vessel was a large arterial branch, however, the renal pelvis and ureter were transposed anterior to the vessel. The anastomosis between the ureter and the renal pelvis was performed with a 4-0 polyglactin suture with an atraumatic needle in a running fashion.
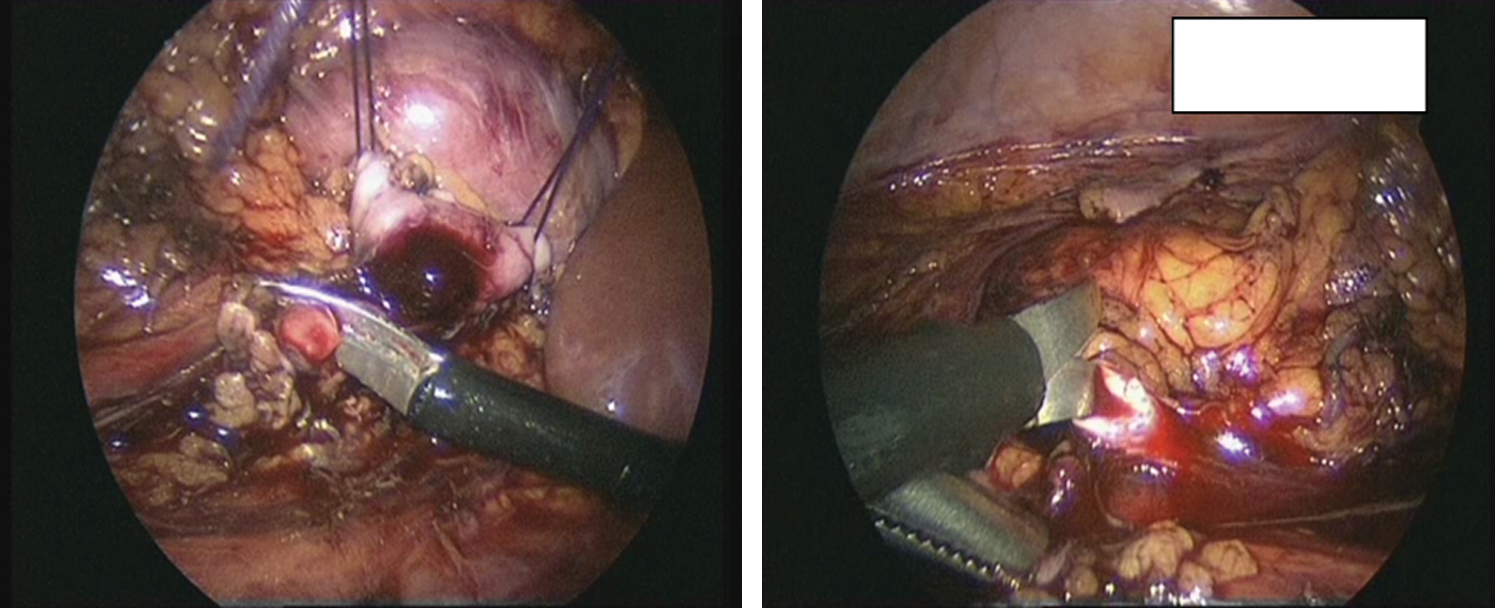
Excision of the renal pelvis and ureteral spatulation performed using a roticulating scissor.
After the completion of the posterior wall anastomosis and before the completion of the anterior wall anastomosis, a retrograde Double-J stent was advanced over the previously placed 0.035-inch guidewire, and the proximal end of the Double-J stent was passed into the renal pelvis. After the anastomosis was completed, a closed-suction drain was placed into the operation area through the SILS-Port site (Fig. 4). The pneumoperitoneum was reduced, a drainage tube was left, and the port site was closed. Within a few days after the procedure, the drain was removed. The bladder catheter was left until the morning after the procedure. The medication used for analgesia was meperidine and was administered intramuscularly at 50 mg doses each time, if necessary. The Double-J catheter was removed under cystoscopic visualization after 1 month in all cases.

At the end of the procedure, a closed-suction drain was placed into the operation area through the SILS Port site.
Assessment of surgical outcome
Ultrasonography (US) und imaging (USG), intravenous urography (IVU) or diuretic renal scan were performed at the third month and semiannually thereafter. Patients were examined clinically every 3 to 6 months depending on symptoms. Radiographic success was defined as improvement of hydronephrosis with a patent UPJ on IVU, or improved drainage on the diuretic renal scan.
Results
All procedures were technically successful without conversion to standard laparoscopy or open surgery. No additional port was used for tissue retraction, and all procedures were purely performed through the SILS Port. An additional polypropylene mesh was designed as a hammock and attached to the abdominal wall with the help of sutures and Hem-o-lok clips for liver retraction, for right-sided procedures. Sutures for liver retraction were passed transabdominally by 60-mm straight needle (Caprosyn, Covidien, Norwalk, CT).
An Anderson-Hynes dismembered pyeloplasty was performed in all patients. Anterior crossing vessels, high insertion, and severe adhesion were found in seven (50%), five (35.7%), and two (14.3%) cases, respectively. In two cases, the UPJ obstruction was caused by a crossing vein or small artery. In five cases, the crossing vessel was a large arterial branch. Patient characteristics and cause (s) of UPJ obstruction are listed in Table 1.
The mean operating-room time, which includes cystoscopy with retrograde ureteral catheterization and open-end stent placement, was 204.5 minutes (range 160–300 min) for the procedure (Table 2). The mean blood loss (Table 2), including urine, was 102 mL (range 80–170 mL). The mean hospital stay was 2 days (range 1–3 d). There was only one minor complication (wound infection at port site) that was managed with oral antibiotic therapy. The success rate was 100%. The mean follow-up period was 6.2 months (range 3–8 months).
Unless otherwise indicated.
Discussion
UPJ obstruction is the most common congenital malformation of the ureter, and the dismembered pyeloplasty described by Anderson and Hynes 10 is the most widely used procedure, providing a success rate higher than 90%. With the advent of endourology, several minimally invasive procedures for approaching the renal pelvis have been described, including antegrade or retrograde endopyelotomy. 11,12 The success rate of these minimally invasive procedures, however, has been consistently less than with open pyeloplasty by 10% to 30%. 13 –15 Morever, all of these procedures would be compromised in kidneys with high insertion of ureters, extensive hydronephrosis, or polar crossing vessels. The bleeding rate is significantly higher when compared with the open procedure. These procedures are also associated with a risk of perioperative hemorrhage necessitating blood transfusion. 16,17
Schuessler and associates 3 first described the Anderson-Hynes dismembered pyleloplasty by a laparoscopic approach. Laparoscopic dismembered pyleloplasty has developed worldwide as the first minimal option to match success rate of open procedures. 18 It has also several advantages over tradional open surgery, including decreased postoperative pain, improved cosmesis, and reduced hospital stay.
Refinement and modification of laparoscopic instrumentation has resulted in a substantial increase in the use of LESS in urology over the past 3 years. Since the initial report of single-port nephrectomy in 2007, various procedures with LESS, including partial nephrectomy, ureterolithotomy, and adrenalectomy, have been performed successfully.
The first clinical experience of dismembered pyeloplasty with LESS was reported by Desai and colleagues. 7 Recently, a study that compared LESS-P with conventional laparoscopic pyeloplasty was reported by Tracy and coworkers. 9 They compared a series of 14 LESS-P to a group who underwent conventional laparoscopic pyeloplasty. No differences in minor or major complication rate, narcotic analgesic use, or postoperative hospitalization time was observed between LESS-P and conventional laparoscopic pyeloplasty. The operative time and the estimated blood loss were significantly lower in patients undergoing LESS-P, however.
In the present study, the mean operating-room time was 204.5 minutes for the procedure, and this is similar to that reported by Tracy and associates. 9 The mean estimated blood loss was 102 mL in our study and significantly higher than in the study by Tracy and colleagues. 9 The estimated blood loss in the present study also included urine, however. Two minor complications (hematuria) and three major complications, including urine leak and acute clot obstruction, have been reported by Tracy and coworkers. 9 In the present study, there was no major complication. In one case, wound infection occurred in the port site in the early postoperative period.
Laparoscopic pyeloplasty may be performed via a retroperitoneal or transperitoneal approach with similar results. 19 The transperitoneal approach provides more space for working, which is very important in reconstructive laparoscopic surgery, such as pyeloplasty. 20 In addition, the transperitoneal approach has some advantages: The surgical trauma is mild, insufflation is easy to perform, and the anatomic mark is obvious. 18 In our series, all procedures were performed transperitoneally.
The incidence of crossing vessels is variable, but in the adult population, it is approximately 50%. 21 We found crossing vessels over the UPJ in seven (50%) cases. In two cases, the UPJ obstruction was caused by a crossing vein or small artery, and these vessels were dissected free. In five cases, the crossing vessel was a large arterial branch; therefore the renal pelvis and ureter were transposed anterior to the vessels.
The dismembered pyeloplasty is typically associated with a 90% to 95% success rate. 22,23 With a mean 6.2-month follow-up period of LESS-P, our success rate was 100%, and it was equivalent to that reported by Tracy and associates. 9 To date, there has been no failure with LESS-P in the published literature.
The retrograde placement of a Double-J catheter during the LESS-P procedure was performed in all cases. The bladder catheter was left in for 2 days, with the purpose of ensuring low intravesical and renal pressures, thereby avoiding Double-J urinary reflux during micturition. Although the previous insertion of a Double-J catheter by means of cystoscopy increases the surgical time, it may prevent the failure of antegrade placement of a Double-J catheter intraoperatively. Some authors advocate not to insert a ureteral catheter before surgery, because they think that antegrade placement of a ureteral catheter involves no great technical difficulty and that having a distended pelvis at the time of surgery facilitates dissection of the UPJ. Some authors think, however, that antegrade placement of a ureteral catheter during laparoscopic pyeloplasty is technically demanding and time consuming.
Our study has a small number of patients, and this is a limitation for this study. The present study would have been enhanced by a larger series of patients. A standardized quality-of-life scoring would also have been used to assess patient satisfaction. Although our patients seem extremely satisfied about their postoperative cosmetic outcomes (Fig. 5), scar satisfaction was not evaluated in the present study. We have not yet quantified or compared scar satisfaction with a validated questionnaire.

Healing of the semilunar incision seen postoperative 1 month later.
Conclusion
Pyleloplasty is a reconstructive procedure that is performed typically in a younger patient population, which may place more importance on the better cosmesis offered from a single incision hidden in the umblicus. With the advent of single port and laparoscopic instrument technology, the LESS-P, as minimally invasive surgery, may take the place of the standard laparoscopic pyeloplasty, and it may be a new choice for the management of UPJ obstruction. Further studies are needed, however, with larger groups of patients to determine whether there are clear advantages to the LESS-P procedure.
Footnotes
Disclosure Statement
No competing financial interests exist.