
Abstract
The lateral repair is an accepted method for the reconstitution of paravaginal defects. Several open or vaginal approaches have been described, but there is still a deficit of reproducible laparoscopic approaches. Thus, only a few clinics perform the laparoscopic approach although it offers several advantages compared to open or vaginal surgery. This article describes our modified laparoscopic approach with inlay of a polypropylene mesh. Operation time will go on about 50 minutes using the here-presented modified approach. The inlay of a mesh with induction of connective tissue may increase long-term stability.
Introduction
In 1909 White 1 described another type of cystocele with sustained rugae. This defect is found more lateral, leads to elapsed sulci, and is called “lateral” or “paravaginal” defect. The anatomic correlate is a rupture of the arcus tendineus and the adjacent fascia. The paravaginal defects have been described isolated or combined with other defects. 2,3 The right side is more often affected, but mostly a bilateral manifestation is found.
Meanwhile, various open and vaginal approaches have been reported. 4,5 The vaginal approach is sophisticated and requires a dilatable vagina. The open approach is associated with a scar and a higher degree of morbidity. The laparoscopic approach came into focus during the last decade. In the few reported laparoscopic approaches, success rates of about 90% have been reported. 6 –8
Meshes have been used successfully for different defects of the pelvic floor. 8 Most authors emphasize the advantages of monofilament meshes, as the risk of mesh erosion is reduced. 8 Meshes provide a matrix and boost the invasion of fibrocytes. This induces a more stable connective tissue. The use of meshes for the lateral repair has been reported only by Rivoire et al 8 and Dubuisson et al. 9 Both studies reported on good intermediate-term outcome of patients.
We here describe our modified laparoscopic lateral repair with a mesh inlay. With our modifications the lateral repair can be performed within 50 minutes. We intend to present an easy and reproducible method of laparoscopic lateral repair.
Technique
Indication
In general, the laparoscopic approach should be considered as an alternative to the open approach. Thus, the indication for a lateral repair operation should be the same as for an open approach.
The paravaginal defect often does not appear as prominent as the midline defects. Patients, in general, report about symptoms related to the vaginal protrusion (vaginal pressure, lower back pain, and sexual difficulty) or associated symptoms of the urinary bladder (urinary incontinence or urinary retention). A perineal ultrasonography helps to distinguish this form from other forms of vaginal prolapse. 11 It is important to use reproducible reference points to compare the pre- and postoperative situation. Thus, the extension of the paravaginal defect is assessed via ultrasonography by the relation of the vesical floor and the lower edge of the symphysis pubis as a reference point. Additionally to the perineal ultrasonography a physical examination is required. The patient should be examined as well in a laying as in a sitting position to assess the influence of pressure. This preoperative assessment is important to prevent an over- or undercorrection and maybe gives information about the quality of tissue.
The loss of the lateral vaginal fixation and symptoms related to a vaginal wall descensus are indications for a lateral repair. Finally, the subjective symptoms of the patient are at least as important as the measurable factors for the decision of an operative intervention.
Preoperative considerations
No special diet or bowel preparation is necessary. Antiembolic compression stockings and a subcutaneous injection of an antithrombosis agent are given routinely starting one evening before operation. There is no need for prophylactic antibiotics.
Operative procedure
The patient is placed in a dorsal lithotomy position with both arms tucked to her side. A 16F catheter with a 10-mL balloon tip is inserted into the bladder and attached to a continuous drainage. Operation is done under general anesthesia.
We routinely perform an incision of the inferior margin of umbilicus and insert a 12-mm access port to introduce the laparoscope. The abdomen is insufflated with CO2 up to 12-mm-Hg intraabdominal pressure. Two additional 5-mm access ports are placed 2 to 4 cm medial and inferior to the anterior superior iliacal spine at both sides. One further 12-mm access port is placed 2 to 3 cm superior to the symphysis (Fig. 1).
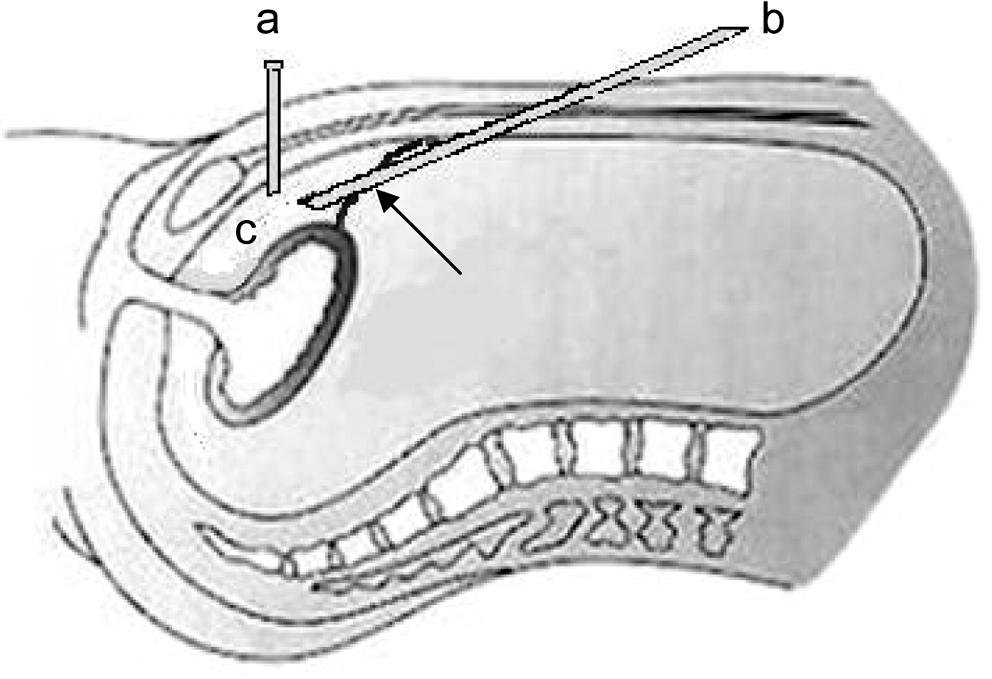
Space of Retzius. A 12-mm access port (a) and laparoscope (b) are placed at the space of Retzius (c). The arrow indicates the retrograde penetration of peritoneum with the laparoscope.
Step one: intraperitoneal survey and preparation of retrograde transperitoneal access to the space of Retzius
After insufflation and intraabdominal survey the suprapubic 12-mm port is retracted and sited outside of the peritoneum. The remaining peritoneal orifice is enlarged to 15 mm and used later as an entrance for the laparoscope (Figs. 1 and 2a).

Intraoperative situation. (
The 12-mm port is used to detect the pubic ramus. The retropubic place is developed by separating the layers. Insufflation with CO2 via the 12-mm port and blunt dissection with the port itself helps to prepare the retropubic space. Both lateral ports are placed under visual control into the space of Retzius.
Step two: preparation of the iliopectineal ligament and the defects of white line
The pubic symphysis and bladder neck are identified in the midline (Fig. 2b). The bladder is dissected from the fatty tissue. The iliopectineal ligament is prepared to its complete length up to the oblique muscle. The lateral margin of the pubocervical fascia is detached from the pelvic sidewall and the white line with the lateral defect(s) is observed bilaterally along the pelvic sidewall using a blunt instrument and a bipolar clamp (Fig. 2b, c).
Step three: suture
A 2-0 nonabsorbable suture of 50-cm length with attached needle is inserted through the 12-mm port. The suture is started on the right side. The first stitch is placed in the iliopectineal ligament as lateral as possible (Fig. 2c). A polypropylene mesh of 6 × 4 cm is inserted and placed to cover the defect (Fig. 2d). The surgeons' left hand is now inserted into the vagina and elevates the anterior vaginal wall with the adjacent pubocervical fascia to the physiological position. The assistant supports the observation of the pubocervical fascia laparoscopically from the space of Retzius and additionally bluntly protects the bladder. The pubovesical fascia is first attached on the level of the cervix. Iliopectineal ligament and pubovesical fascia are then sutured consecutively along the paravaginal defect starting laterally and ending toward the urethrovesical junction (Fig. 2e). To avoid a displacement of the mesh a fixation with one or more stitches is useful.
In general, four to six stitches at the ligament and at the fascia, respectively, are used for a stable tissue approximation. The physiological position of the lateral vagina should be reconstituted with a moderate degree of tension. For this purpose a fine adjustment of the consecutive suture is possible. Suture is completed by the use of an intracorporal knot-tying technique.
For the left side the suture procedure is repeated basically, but, in general, we start medially at the urethrovesical junction and end laterally (Fig. 2f).
Step four
Needles are removed via the 12-mm port. There is no need for a suture of the peritoneal incision. Ports and CO2 are removed from the space of Retzius after a careful hemostasis.
Postoperative treatment
Continuous urinary drainage is removed after 24 hours. Urinary retention is checked via ultrasonography 6 hours later. Nonsteroidal antiphlogistics will be sufficient to reduce postoperative pain.
Follow-up
Patients who underwent laparoscopic lateral repair with mesh inlay between February 2005 and June 2008 were included (n = 85) in our follow-up. Intraoperative complications (bleeding, bladder, or bowel injury) and postoperative complications (infections, urinary retention, and others; Table 1) were analyzed using the stationary and operative reports.
Patients were invited for re-evaluation (vaginal examination and perineal ultrasonography) in June 2009 (73% participation; mean follow-up, 30 months; range, 12–52 months).
Equipment
Access ports: 2 × 5 mm and 2 × 12 mm
Instruments: 1 Metzenbaum scissors, 2x universal (blunt) grasping forceps, 1 bipolar forceps, and 1 needle holder
Full HD Camera 0°
Polypropylene mesh 6 × 4 cm
2 sutures (2-0 nonabsorbable suture of 50 cm length with attached needle)
Role in Urologic Practice
Our method differs from conventional lateral repair concerning the following aspects: We use a very small peritoneal incision for the retrograde laparoscopic access to the space of Retzius. A suture is not necessary. Operation time is reduced. Pubic bone is used consequently as a leading structure for the preparation of the layers. This might help to reduce bladder injury and bleeding. There is no need to fill up the bladder intraoperatively. We prefer a combined suture/mesh technique (polypropylene mesh). Mesh is fixed by one or more stitches. The mesh may induce connective tissue and supports the stability resulting from suture.
The lack of reproducible and standardized operation methods is reflected in the rare use of laparoscopic lateral repair operation. 6 –8 Our method simplifies the laparoscopic approach, resulting in a reduced operation time and good reproducibility. It offers advantages concerning postoperative comfort, recovery time, scars, postoperative pain, and duration of hospitalization (Table 1). Complication rate of our method is acceptable and seems to be better than after vaginal approach (Table 1). 6,8,10,12,13 In accordance to other authors 8,9,14 we used monofilament polypropylene meshes to induce a stable connective tissue. In the follow-up no mesh erosion or other mesh-associated complications were found. Postoperative results were good (Table 1). In a further study, we investigated sexual impairment after endoscopic sacropexy using two validated sexual questionnaires (International Consultation on Incontinence Modular Questionnaire [ICIQ]-vaginal symptoms, sexual part and ICIQ-sex). 15 Eighteen patients underwent simultaneous lateral repair. Fifteen patients reported sexual activity before operation. All sexually active patients reported of an improved sexuality after operation (ICIQ-vaginal symptoms: preoperative sexual score 28.5; postoperative sexual score 10.5; p = 0.001; ICIQ-sex: preoperative score 3.6; postoperative score 1.9, p not significant, two-sided paired t-test). Single-item analysis revealed a maximum benefit concerning pain during intercourse, urinary incontinence during intercourse, interference of sex life because of worries, and affected partnership.
We consider our laparoscopic lateral repair with a combination of suture and mesh inlay as a good instrument for a durable repair. Although our modifications make the laparoscopic lateral repair easier and more secure, the surgeon should be experienced in the anatomical characteristics of the bladder region and in intracorporal laparoscopic suture and knotting techniques. Further studies will show whether the use of meshes elevates the long-term stability of repair.
Footnotes
Disclosure Statement
No competing financial interests exist.
Abbreviation Used
*
A video demonstrating this technique is available at
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.