
Abstract
Purpose:
We aim to determine whether end-fire probe orientation (and therefore image orientation and biopsy needle direction) during transrectal ultrasonography-guided prostate biopsy has an effect on the prostate cancer (PCa) detection rate, the number of positive biopsy cores, the proportion of diseased tissue in the samples obtained, and the Gleason score. We compared two different axial image protocols and a sagittal image protocol for PCa yield. We hypothesize that axial probe methods direct more of the biopsy needle through the peripheral zone, the principal site for PCa, and therefore improve PCa yield.
Patients and Materials:
A total of 441 patients underwent systematic 12-core biopsy using three different methods by six radiologists at our institution. An axial method using probe angulation, an axial method using probe rotation, and a sagittal method were compared.
Results:
The axial-angulation method was used in 166 men, the axial-rotation method was used in 125 men, and the sagittal method was used in 150 men. Overall, 58.3% had PCa detected. Axial-rotation techniques showed a 17% greater PCa yield and significantly increased the number of positive biopsy cores relative to the sagittal method (P < 0.001) for all patients and for those with a prostate-specific antigen level <10ng/mL. Of those with PCa, the number of positive cores, proportion of diseased tissue, and Gleason score were also significantly elevated using this technique (P < 0.05).
Conclusion:
This study suggests that axial techniques have the potential to increase carcinoma yield and Gleason score, through a greater yield in positive core number and proportion of diseased tissue in the samples obtained.
Introduction
Therefore, new strategies have been investigated to improve the prostate carcinoma (PCa) detection rate. Most investigators have focused on different biopsy strategies, such as increasing the number of cores taken (it is suggested that 8 to 10 biopsies will improve diagnosis by 20% to 30% over the traditional sextant protocol), 2 use of contrast-enhanced color flow Doppler ultrasonography, 3 elastography, 4 histoscanning, 5 or sampling from distinct regions of the prostate, with the aim to increase peripheral zone sampling. Indeed, improved rates of cancer detection have also been described with more laterally placed systematic sextant biopsies, 2,6 suggesting that the originally described anteriorly directed trajectories of the traditional sextant model undersampled the peripheral zone.
Several techniques are available to sample the prostate, including end- and side-fire probes. Some data suggest that end-fire probes show improved rates of cancer detection over side-fire probes. 7 The suggested reason for this is improved sampling of the most lateral part of the peripheral zone.
To our knowledge, there is little published evidence regarding probe orientation and cancer detection rates. We aimed to evaluate whether using an axial or sagittal probe orientation made a difference to PCa detection rates, the number of positive cores, the proportion of diseased tissue obtained, and the Gleason score.
We postulate that axial techniques allow the biopsy needle to traverse a greater proportion of the peripheral zone when compared with the sagittal technique, and therefore the amount of diseased tissue and therefore detection rates and grade could be higher using this technique. We also aimed to compare two different axial techniques: An axial-rotation and an axial-angulation technique that show varying degrees of peripheral obliquity through the peripheral zone. We speculate that the axial-angulation technique allows the biopsy needle to obliquely traverse more peripheral zone and therefore detection rates may be higher using this technique.
Patients and Methods
We evaluated 441 men who underwent TRUS-guided biopsy because of elevated prostate-specific antigen (PSA) levels and/or abnormal digital rectal examination over a 2-year period (2008 and 2009 inclusive). The study was performed in line with local audit guidelines.
All patients underwent a systematic 12-core (six 18-gauge biopsies performed in each lobe of the prostate) biopsy using three different methods by six radiologists at our institution. An axial method using probe angulation, an axial method using probe rotation, and a sagittal method were compared. Two radiologists used the axial-angulation method, two radiologists used the axial-rotation method, and two radiologists used the sagittal method. Clinical experience in TRUS-guided prostate biopsy was in excess of 10 years and 2 years, respectively, for radiologists using the axial-angulation method, in excess of 10 years and 6 months, respectively, for operators in the axial-rotation group, and both operators had more than 10 years of experience in the sagittal group. Consecutive patients were referred for biopsy by two consultant urologists who share management of prostate disease at our institution, using the same referral guidelines, with each radiologist receiving referrals from both urology clinics on a next appointment basis. The referral pattern was recorded as was interoperator variation in biopsy number and cancer yield for each method to ensure equivalent rates between operators.
All biopsies were performed on the same ATL ultrasound machine using a standard end-fire transrectal 7.5 MHz probe. Each procedure was undertaken in the left lateral position with antibiotic prophylaxis (ciprofloxacin 500 mg), with periprostatic local anesthetic (10 mL of 1% lidocaine) infiltration and with rectal application of Instilagel.
Age, PSA levels, and prostate volume as measured at TRUS were analyzed to ensure comparable populations. The histology and, where applicable, immunohistochemistry reports were then analyzed. A positive result was counted as one describing adenocarcinoma. Prostatic intraepithelial neoplasia (PIN) was recorded as a secondary outcome. Further outcomes that were assessed included the number of positive cores for all patients. Of those with a diagnosis of cancer, the number of positive cores, the proportion of positive tissue of the samples obtained, and the Gleason score were compared between techniques.
Statistical analysis
Data were compared using the Smith Statistical Package, 2005. The chi-square test was used to assess: Referral pattern and interoperator rates of cancer detection The incidence of positive biopsy for PCa The incidence of PCa in patients with a PSA level <10 ng/mL The incidence of PIN The incidence of positive cores in all patients and those with PCa
Analysis of variance was used to compare: Age, PSA level, and prostate volume The proportion of positive tissue and the Gleason score for patients with PCa
Description of techniques
The axial-angulation method involves oblique biopsy of the peripheral zone with more extreme angulation to sample the left lobe peripheral zone, while the probe position is maintained in other planes (Fig. 1). The trajectory of the biopsy needle is therefore anterolateral. The axial-rotation method involves peripheral zone sampling of the right lobe in a manner similar to that seen in the previously described technique. The probe is then rotated 180 degrees to sample the left lobe (Fig. 2). Again, the trajectory of the needle is anterolateral, although it is less oblique. A comparison of the two axial techniques is illustrated in Figure 3. The sagittal technique involves imaging the gland in sagittal and parasagittal sections. The trajectory of the needle is, therefore, superiorly orientated (Fig. 4).
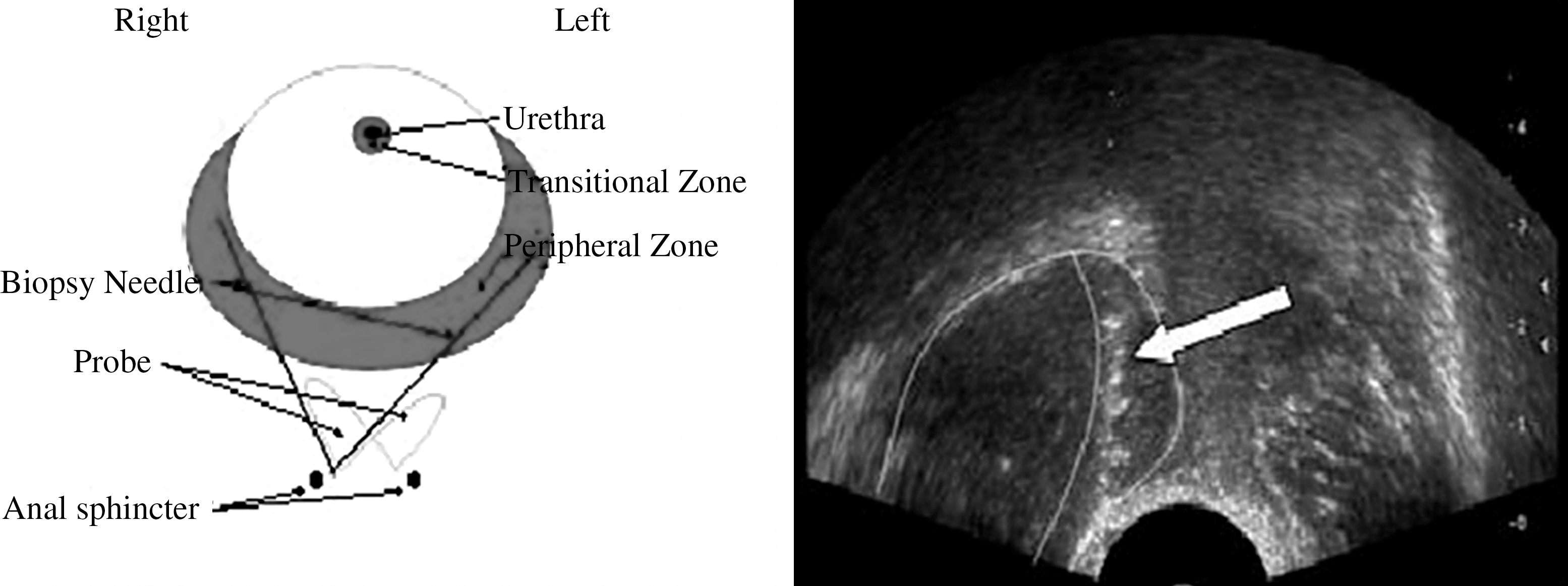
Schematic image showing the axial-angulation technique (left). Axial transrectal ultrasonography image (right) shows biopsy of the left peripheral zone using the axial angulation technique. The arrow highlights the needle trajectory.
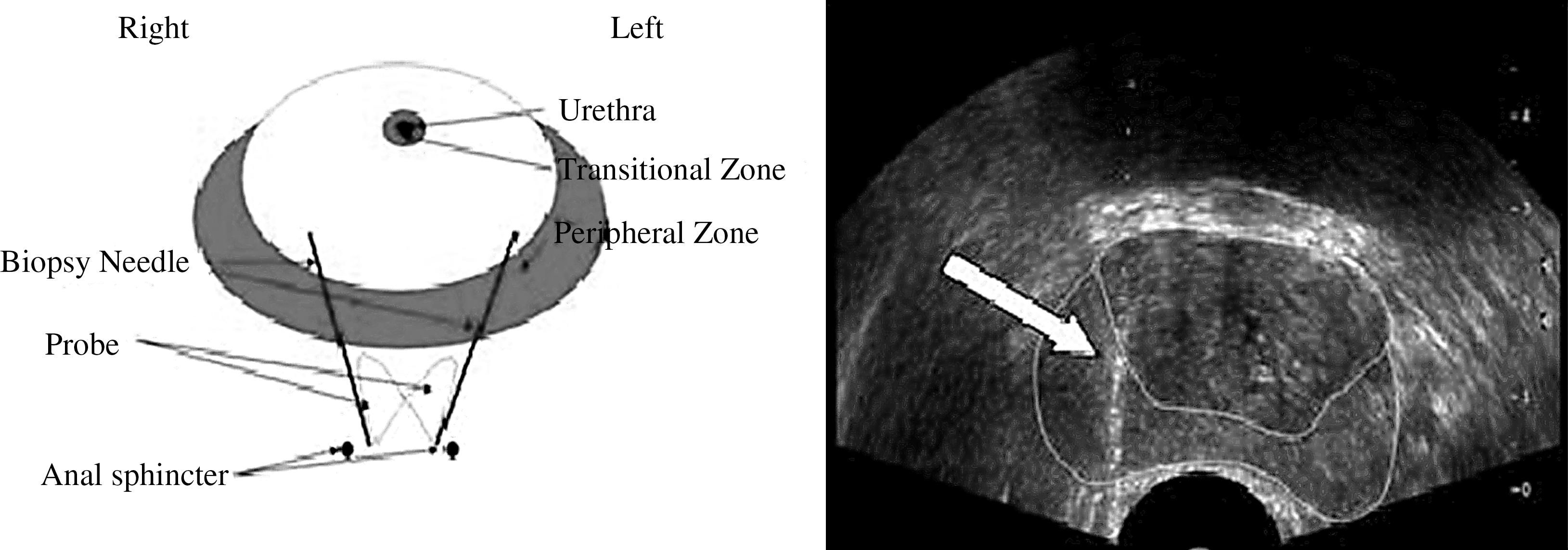
Schematic image demonstrating the axial–rotation technique (left). Axial transrectal ultrasonography image (right) shows anteriorly orientated trajectory (arrow) of the biopsy needle.
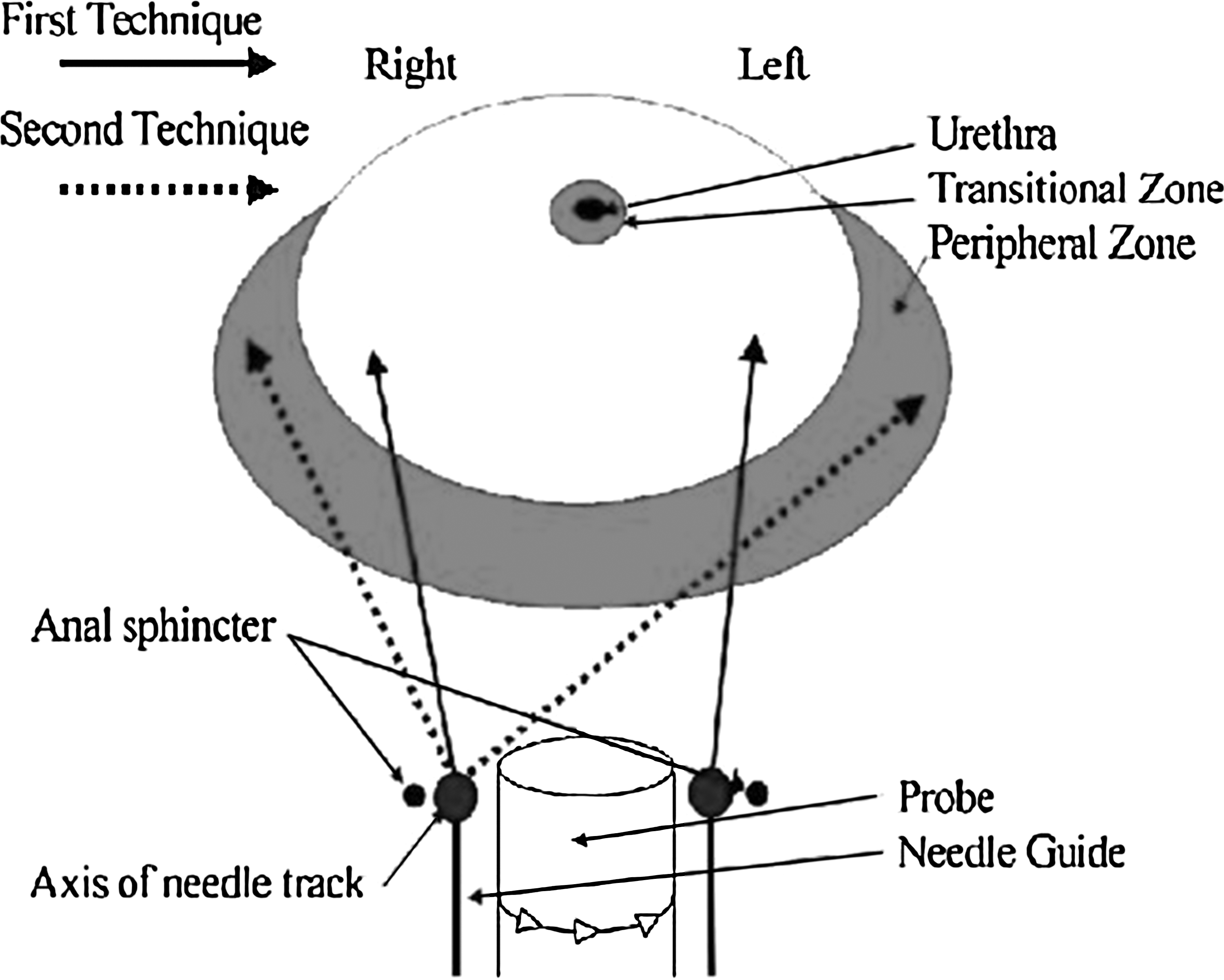
Schematic representation of the two axial techniques. First technique: axial-rotation; second technique: axial-angulation.
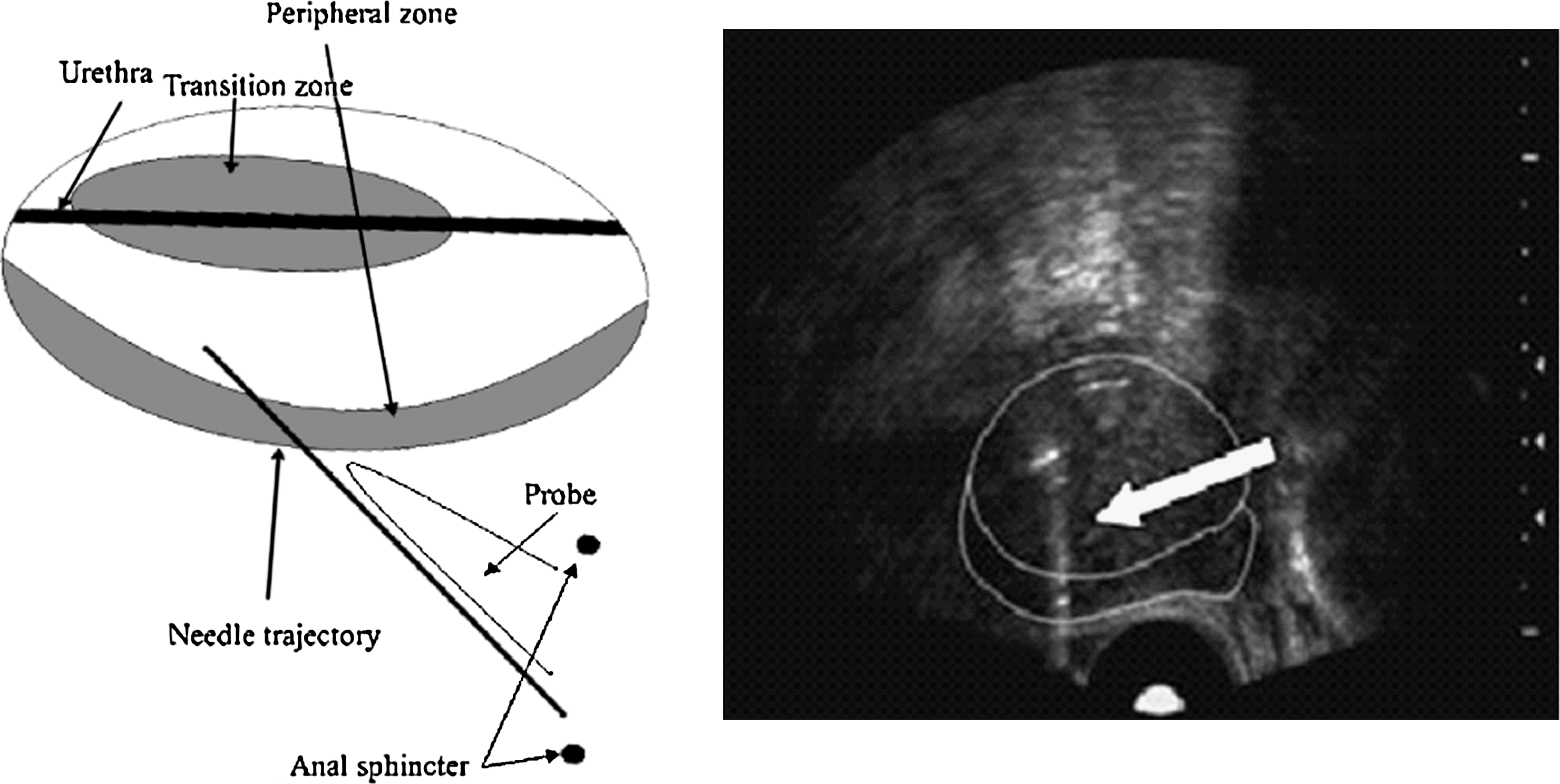
Schematic representation of the sagittal technique (left). Sagittal transrectal ultrasonography image (right) shows superiorly orientated trajectory (arrow) of the biopsy needle.
Results
The axial-angulation method was used in 166 men, the axial-rotation method was used in 125 men, and the sagittal method was used in 150 men. Age, PSA levels, and prostate volume in axial and sagittal groups are shown in Table 1. The breakdown of number of biopsies performed by each radiologist in the study period, interoperator PCa yield, and ratio of referrals from each urologist is shown in Table 2. No significant difference in PCa yield was demonstrated between operators using the same technique (Table 2). Likewise, no significant difference in the ratio of referrals from the different urologists to each of the biopsy techniques was seen (Table 2).
SD = standard deviation; CI = confidence interval; PSA = prostate-specific antigen.
Overall, 58.3% of the studied population had PCa detected. The axial-rotation technique yielded 64.0% and the axial-angulation technique yielded 57.2%, whereas the sagittal technique yielded 54.7%. These values, however, did not achieve statistical significance (Tables 3 and 4). When axial techniques were combined, the axial methods (n = 291) showed a 5.4% difference (60.1% vs 54.7%) in detection rate, resulting in a 9.9% improvement in PCa detection, but this was not statistically significant (P = 0.2696) using the chi-square formula. When individual lobes were considered, surprisingly, the axial-rotation technique demonstrated significantly greater yield for the left lobe relative to the axial-angulation technique (P = 0.0275). No other significantly different values were seen in yields for individual lobes. No significant difference in the yield of PIN was seen between techniques (P > 0.05). The axial-angulation technique yielded 15.1%, the rotation technique yielded 9.6%, and sagittal technique yielded 8%.
PSA = prostate-specific antigen.
PSA = prostate-specific antigen; PIN = prostatic intraepithelial neoplasia; ax = axial.
Although the cancer detection rates did not achieve statistical significance, the axial-rotation technique yielded a greater number of positive cores (33.8% vs 24.1%) relative to the sagittal technique (P < 0.001). The axial-angulation method also yielded a significantly larger number of positive cores relative to the sagittal technique (P < 0.05). Furthermore and surprisingly, the axial-rotation method yielded a significantly greater number of positive cores relative to the axial-angulation method (P < 0.001). No significant difference in cancer yield was noted for patients with a PSA of <10 ng/ml; however, both axial techniques yielded a greater number of positive cores in this group compared with the sagittal technique (P < 0.05).
Of the patients who received a diagnosis of PCa, the number of positive cores was greater using the axial-rotation technique relative to the sagittal technique (P = 0.001) and the axial-angulation technique (P < 0.05) (Table 5).
When the proportion of the sample exhibiting disease in each lobe (Table 6) was compared between techniques, both axial techniques demonstrated significantly increased disease volume relative to sagittal techniques (axial-angulation vs sagittal: P < 0.05; axial-rotation vs sagittal: P < 0.001). No significant difference was noted between axial techniques (P = 0.1356).
SD = standard deviation.
In keeping with these findings, the Gleason score (Table 6) was significantly greater using the axial-rotation technique relative to the sagittal technique (P < 0.05). A larger number of patients exhibited Gleason scores of 8 and 9 using the axial-rotation technique. The axial-angulation technique showed no significant difference in Gleason score relative to the sagittal technique (P = 0.21). No significant difference between axial techniques was seen for the Gleason score (P = 0.27). The distribution of Gleason score for each technique is displayed in Figure 5.
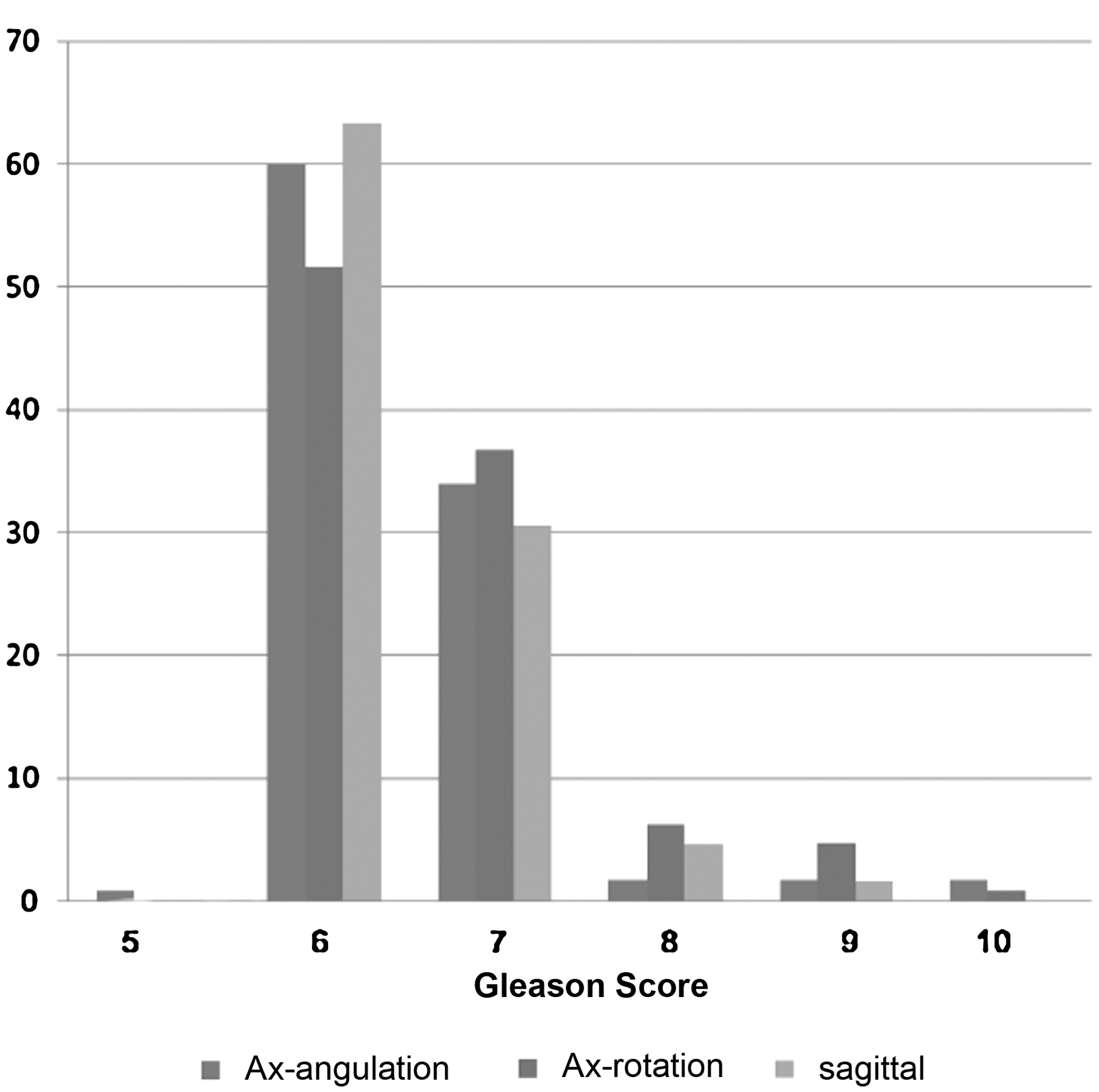
Distribution of Gleason scores obtained using the different techniques.
Discussion
Our results show that axial techniques showed greater yields in PCa detection relative to sagittal techniques, with an approximately 10% improvement in cancer detection rate when both axial techniques were combined, rising to a 17% improvement when the axial-rotation technique alone was compared with the sagittal technique. Although these values did not achieve statistical significance with the samples studied, when the number of positive cores was compared, axial techniques showed statistically greater yields for all patients and for those patients with a PSA level below 10 ng/mL, with the axial-rotation technique achieving a greater number of positive cores relative to the axial-angulation technique as well as the sagittal technique for all patients. Of those patients with a diagnosis of PCa based on this biopsy sample, the axial-rotation technique demonstrated a significantly greater number of positive cores, greater proportion of diseased tissue in the cores obtained, and greater Gleason score.
Additional findings included a significantly greater carcinoma yield for the left lobe using the axial-rotation technique relative to the axial-angulation technique, which is surprising, because we presumed that the biopsy needle would traverse a greater distance through the peripheral zone using the angulation method and therefore the amount of diseased tissue, cancer yield, and possibly grade would be greater using this technique. No significant difference in the PIN detection was seen between techniques.
We are surprised that the results for carcinoma detection did not reach statistical significance, because we believe that the scientific basis 2 for the difference in detection is sound. Perhaps a larger study group may be necessary to achieve statistical significance. Indeed, improved rates of cancer detection have been described with more laterally placed biopsies, 2,6 and end as opposed to side-fire probes 7 that are presumed to sample more of the lateral part of the peripheral zone. The number of positive cores was significantly greater using the axial techniques, however, suggesting that there is some basis for this hypothesis. Furthermore, when adenocarcinoma was present, the proportion of positive tissue within the acquired sample, number of cores (and for the axial-rotation technique, Gleason score) was significantly increased. This evidence further supports the theory that axial methods acquire more diseased tissue and possibly result in a mild increase in disease grade.
We postulated that axial techniques allow the biopsy needle to traverse a greater proportion of the peripheral zone when compared with the sagittal technique and therefore detection rates are higher using axial techniques with greater needle obliquity, so sampling more of the laterally placed peripheral zone. We did not show, as had been hypothesized, that the axial-angulation technique was the most productive method, but, in fact, that the axial-rotation method, which exhibits a more anteriorly orientated trajectory, showed the greatest diagnostic yield and number of positive cores. Furthermore, yield in the left lobe, where the axial methods differed most in their trajectory, was greater using the rotation method. The reasons for this are not clear; it is conceivable that the axial-angulation method, despite obliquely traversing more of the peripheral zone, more commonly missed, or failed to optimally sample, the majority of the more posteriorly situated lesions.
This study is limited by its retrospective design. Furthermore, patients were not formally randomized, although patients were referred on a next appointment basis and the ratio of referrals from the two urology teams was approximately equal for each technique. No significant difference was seen between detection rates achieved by different operators. Each group showed approximately equal distributions of age and PSA level. The axial-rotation technique group demonstrated a smaller mean prostate volume relative to the other groups. This is a potential confounding factor, with PSA values being similar and the volume in this group lower, the number of patients with cancer may naturally have been greater, although this is difficult to prove. Furthermore, some authors advocate a greater number of cores for larger prostates 2 to ensure that if a tumor is present, it is sampled effectively. Varying core number, however, would itself have been a confounding factor.
We are not aware of any survey within the literature that has established which methods are most commonly used either by urologists or radiologists, and although there is general consensus regarding core number, we are not aware of consensus regarding specific biopsy technique in terms of image orientation. 8 Certainly, many new techniques using new technology 3 –5 have been advocated; however, we feel that this study begins to answer a simple but fundamental question using established technology that has the potential to alter the biopsy technique adopted by urologists and radiologists alike. To further investigate this hypothesis, we believe a large prospective, randomized trial is advocated.
Conclusion
We suggest that our study shows that axial techniques have the potential to increase carcinoma yield and Gleason score through a greater yield in positive core number and proportion of diseased tissue in the samples obtained.
Footnotes
Disclosure Statement
No competing financial interests exist.