
Abstract
Background and Purpose:
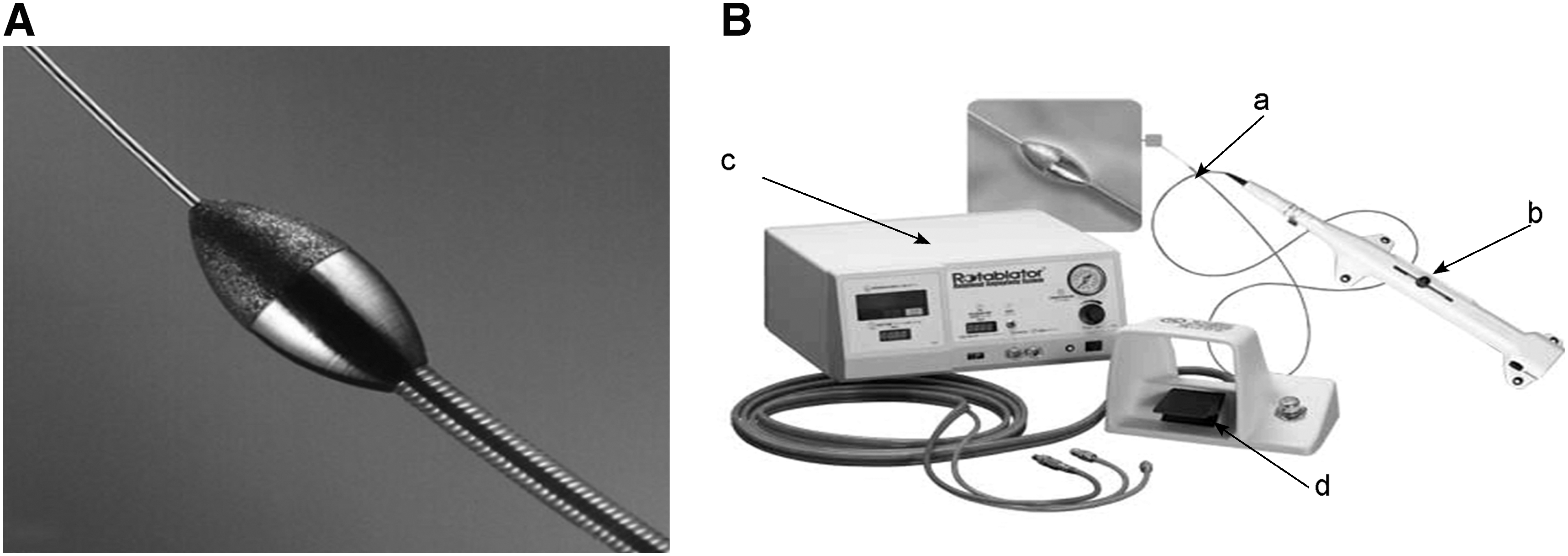
The Rotablator® is an angioplasty device that is passed over a wire. It uses a high-speed rotational “burr” (2 mm in diameter) that is coated with microscopic diamond particles and cooled by saline. It rotates at high speed (approximately 200,000 rpm) breaking up endovascular blockage into minute (smaller than red blood cells) fragments. We investigated, in vitro and ex vivo, the possible use of the Rotablator for urinary stone disease.
Materials and Methods:
Human stones of different sizes and composition were used for the experiment. Stone impaction in vitro was modeled by wedging the stones into the proximal part of a 16F silicone Foley catheter. Likewise, an ex-vivo study was performed on stones placed into a freshly harvested swine ureter using a nitinol basket. Data regarding the drill time, remaining stone size, and ureteral damage were collected.
Results:
Overall, 15 stones were treated (10 in vitro and 5 ex vivo). The device successfully drilled through all the stones, along the path of the guidewire, allowing complete passage of the burr. The pretreatment mean stone size for the silicone and ureteral testing was 65 mm3 and 34 mm3, respectively (both P < 0.01). The post-treatment size was 54 mm3 and 24 mm3, respectively. Average treatment time was 100 seconds. No visual macroscopic ureteral damage or perforation was observed.
Conclusions:
In vitro, the Rotablator is capable of drilling through stones with minimal damage. Drilling, however, occurred alongside the stone in which the guidewire was located and, thus, stone fragmentation appears to be minimal. Further studies are necessary to investigate other burr configurations and the use of the Rotablator for the fluoroscopic-guided passage of ureteral impaction in difficult clinical settings.
Introduction
(
The basic physical principle behind this property is referred to as differential cutting. Differential cutting allows the advancing burr to selectively cut inelastic material, such as atherosclerotic, calcified, and fibrotic plaques, while elastic tissue deflects away from the burr. 9 As such, if one were to compress the burr head against the calcified shell of a hard-boiled egg with a finger, the eggshell would be specifically drilled away without damage to the inner egg or human skin.
The mechanism and its effectiveness, particularly the insignificant magnitude of vessel expansion have been evaluated by intravascular ultrasound studies. 10,11 The tip is also kept cool by saline irrigation, preventing thermal heat injury. Furthermore, at rotational speeds greater than 60,000 rpm, orthogonal displacement of friction occurs, which aids in the passage and retrieval of the device through tortuous vessels. 12 The generated microparticulate debris (95% less than 5 μm) does not significantly affect microcirculation and is eventually cleared by the reticuloendothelial system. 13
We sought to investigate the potential urologic role of the Rotablator in ureteral stone obstruction.
Materials and Methods
The Rotablator device consists of the Rotablator catheter with the oval-shaped burr on the distal tip of the drive shaft, the burr advancer, the control console monitoring as well as regulating the rotation speed, and the activator pedal (Fig. 1B). The drive shaft but not the burr is covered with a 4F Teflon sheath that is continuously lubricated by pressurized saline flush. A lubricant substance (RotaGlide,® Boston Scientific, Natick, MA) is added to the irrigation fluid (normal saline) to allow for almost friction-free rotation of the drive shaft within the sheath.
There are eight different burr sizes available for coronary rotational atherectomy. The smallest burr is 1.25 mm and the largest is 2.5 mm. The other sizes include 1.5 mm, 1.75 mm, 2.0 mm, 2.15 mm, 2.25 mm, and 2.38 mm. The selection of the burr size is based on the burr/artery diameter ratio, which should not exceed 0.70. For insertion of the Rotablator catheter, a guiding catheter with a size large enough (8–10F) to harbor the different burr diameters is usually used. The guiding catheter covering the Rotablator catheter (burr and drive shaft) is then brought to the site of lesion, and the Rotablator catheter is exposed short before the lesion. In this experiment, because of its in-vitro and ex-vivo design, no guiding catheter was used.
The stainless steel guidewire that runs within the drive shaft and exits central on the tip of the burr has a shaft diameter of 0.009 inches. The lumen tip is soft and can have varying degrees of stiffness in the four different available guidewires, allowing for an adjustable steerability in diverse settings. Each guidewire is equipped with a guidewire clip that serves as a torque device. After exposure of the burr out of the guiding catheter, the guidewire is advanced and crossed over the lesion. Thereafter, the burr is activated and moved toward the lesion in a smooth pecking motion until all the way through the obstruction. The rotational speed is regulated by the activator pedal up to the maximum speed preset on the console. To upsize the burr, the guidewire is left in place, the burr removed, and the larger Rotablator catheter inserted over the guidewire.
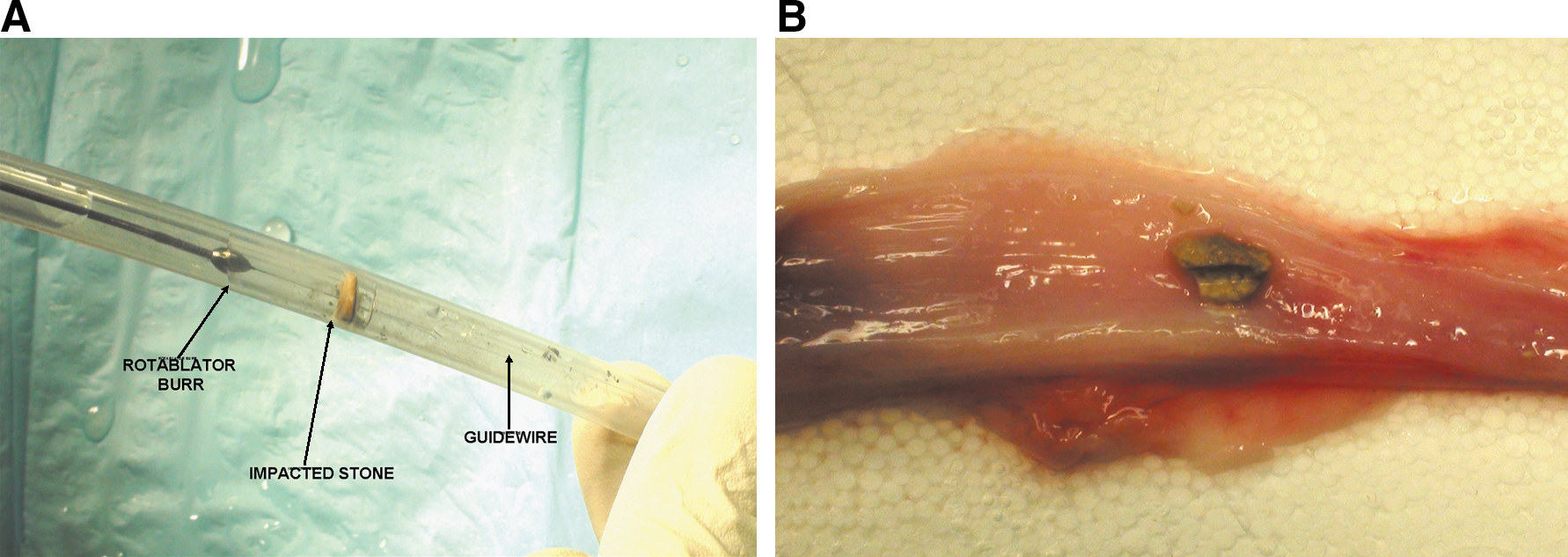
To assess the effectiveness of this device in dealing with often very resistant stones formed in the urinary tract, previously retrieved human concernments of different composition and size were selected. Overall, 15 stones (5 calcium oxalate monohydrate, 5 calcium oxalate dihydrate, 3 uric acid, and 2 cysteine stones) were investigated. After careful, three-dimensional stone sizing, in the first part of the experiment, stone impaction in vitro was created by wedging a stone fragment into the proximal part of a 16F silicone Foley catheter (Fig. 2A). Data regarding the drill time, remaining stone size, and location of the created drill channel were collected.
(
In the second aspect of the experiment, an ex-vivo study was performed on two freshly harvested swine ureters to assess any collateral damage of the Rotablator device to the biologic tissue. Stone impaction was created by placing calcium oxalate monohydrate and dehydrate stones by a nitinol basket first in the midureter and subsequently at the ureteropelvic junction (two stones in each ureter, four stones overall). After treatment, the ureters were incised longitudinally and any tissue damage assessed. Again, drill time, remaining stone size, and location of drill channel were registered (Fig. 2B).
Statistical analysis
Treatment time and stone size both pretreatment and post-treament were collected and analyzed. The Student t test and Fisher exact test were performed to compare the stone sizes of the in-vitro and ex-vivo groups with P < 0.05 considered statistically significant.
Results
Overall, 15 stones were treated (10 in vitro and 5 ex vivo). The two uric acid stones were very brittle and were pulverized by the Rotablator. One stone was displaced by the device in the ex-vivo experiments before completion of the ablation. All three mentioned stones were excluded from the analysis. All remaining 12 (8 in vitro and 4 ex vivo) stones were treated successfully. The device drilled through all the stones, allowing complete passage of the burr beyond the site of obstruction.
The pretreatment mean stone size for the silicone and ureteral testing was 65 mm3 and 34 mm3, respectively. The post-treatment size was 54 mm3 and 24 mm3, respectively (both P < 0.01). Mean treatment time (defined as time to drill through impaction) was 100 seconds (range 40–210 seconds). No visual macroscopic ureteral damage could be observed. There were no perforations.
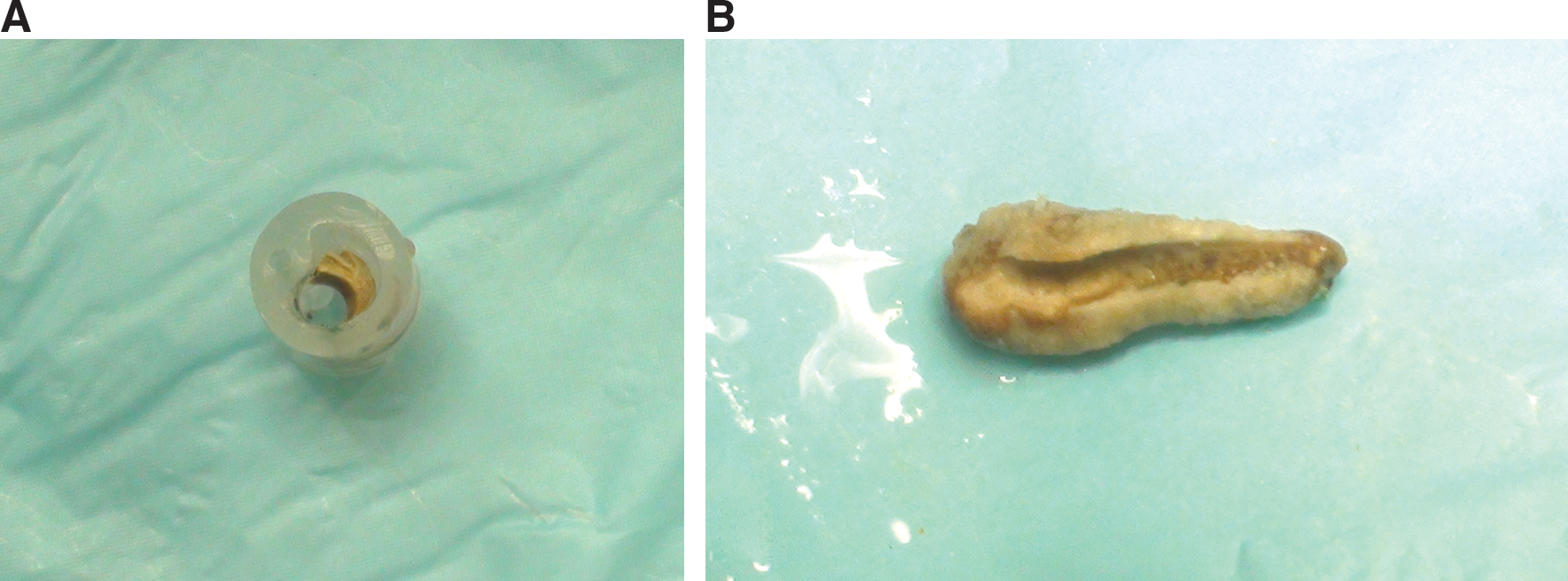
Although the stones were not completely fragmented, a smooth, columnar defect was created in all stones. The site of the drilled channel was, without exception, located at the perimeter of the impacted stone (Fig. 3). Direct observation of the drilling process of the device in the in-vitro setting through the transparent silicone catheter afforded following the passage of the guidewire and the burr. In cases in which the guidewire could pass over the stone, drilling started quickly. In instances where the passage of the guidewire was not possible, the burr drifted after initial pecking at stone to the periphery, following the path of least resistance and lodged at one site. The drilling process started in these instances slowly and less effectively. Once a small opening appeared and the guidewire could be passed through, the Rotablator proceeded more efficiently.
(
Discussion
The current study demonstrates feasibility of the Rotablator Rotational Atherectomy device to mechanically drill through solid and resistant stone material encountered in the urinary tract. It further shows that the principle of differential cutting is also operational in the cavity of the urinary tract and not only in the vasculature system. To the best of our knowledge, this is the first study to evaluate such a device specifically for urologic stone disease.
In clinically difficult endourologic cases with impacted ureteral stones in which guidewire placement is unsuccessful, the Rotablator could potentially create a working channel and provide a guidewire passage for the placement of a ureteral stent or definitive treatment. Other situations, such as stent encrustation, may also benefit from the Rotablator.
Based on the conception of the Rotablator as a drilling device to tackle circumferential atherosclerotic vessel lesions, the main shortcoming of this tool in urolithiasis becomes obvious. The Rotablator works more like a sander, creating a polished columnar defect and with minimal collateral material fragmentation. With regard to urolithiasis treatment, stone fragmentation into smaller pieces is desirable. For this device to meet urologic expectations as an intracorporeal lithotripter used under imaging guidance, changes to the burr dimension but also possible modification of the burr's configuration would be necessary. For example, the requirement to have microparticle debris that does not inflict damage on blood circulation is not relevant in the urinary tract. The question arises whether a coarser burr coating along with a larger burr size than that used in the current experiment would allow for adequate stone fragmentation. Similarly, the concept of having the entire burr coated with diamond particles may allow for retrograde stone treatment while retracting the device over the guidewire to reduce frustrating stone migration.
Before urologic application of the Rotablator for endourologic stone management, the issue of stone extraction would need to be addressed. More traditional hydraulic and ultrasonic methods of stone fragmentation carry the potential risk of mechanical damage to the tissue with possible development of strictures. Holmium laser technology, although very effective in stone fragmentation, also has the potential risk of significant heat injury with similar sequelae. Bleeding and perforation are also other associated risks. Furthermore, stone migration during treatment has always remained a frustrating challenge during ureteroscopy. A new approach would be to consider the idea of “sanding” the stone in small particles in an atraumatic manner either under direct vision or fluoroscopy in an antegrade fashion (treating the stone with the back end of the Rotablator while retracting the burr head toward the camera).
The unique feature of this device is its atraumatic nature to the normal tissue as well as its ability to pass through tortuous, small arterial vessels. This opens new fields of application in the arena of stone treatment, such as transplant kidney stone management or continent diversion urolithiasis, where standard ureteroscopy and equipment are limited. In these difficult circumstances, the Rotablator device would render safe passage over impacted stones and guidewire placement under fluoroscopic guidance.
Further studies, however, would be necessary to assess the compatibility of this device with existing endourologic equipment for management of urolithiasis. Such animal model studies would help pave the way for the collaboration with the industry to adapt this device and technology to urologic needs.
This preliminary study did not aim to illustrate the material and procedural costs that the application of this device would entail. It goes without saying that for this device to become widely accepted, it must withstand the tests of cost-effectiveness.
Conclusion
The Rotablator® Rotational System is capable of safely drilling over a guidewire through urinary stones with no apparent damage to the ureteral mucosa. Stone fragmentation, however, is minimal, especially beyond the radius of the burr. Further animal studies are necessary to investigate the use of the Rotablator for the fluoroscopy-guided passage of ureteral impaction in difficult clinical settings.
Footnotes
Acknowledgment
Boston Scientific provided the Rotablator.®
Disclosure Statement
No competing financial interests exist.