
Abstract
Purpose:
To present our initial experience with the laparoendoscopic single-site surgery (LESS) approach to bladder diverticulectomy.
Patients and Methods:
Four patients underwent LESS bladder diverticulectomy for the management of diverticula that were associated with persistent symptoms. The median diameter of the diverticula was 8.5 cm (range 4–9 cm). Immediately before, a double-pigtail ureteral catheter was inserted in the ureter on the side of the diverticulum. An 18F urethral catheter was placed via guidewire, and its balloon was inflated into the diverticulum under fluoroscopic control. A TriPort inserted in the umbilicus and a combination of prebent and conventional laparoscopic instruments were used. The balloon inside the diverticulum was inflated and the diverticulum were incised. The diverticulum was dissected circumferentially and removed. Suturing of the bladder lesion followed. The specimen was extracted through the umbilical incision. Perioperative parameters were recorded. Postoperative follow-up included cystography, uroflowmetry, and ultrasonography measurement of postvoid residual urine.
Results:
Average patient age was 51 years (range 42–66 y) and the average body mass index was 26 kg/m2 (range 23.7–28.7 kg/m2). Average operative time was 130 minutes (range 101–154 min). Blood loss was minimal, with 150 mL the higher loss. Complications were not observed during the follow-up period. The catheter was removed on postoperative day (POD) 8 (n = 3) and on POD 9 (n = 1). Histologic examination did not reveal malignancy. Postoperative pain and analgesic medication requirement were minimal.
Conclusions:
LESS bladder diverticulectomy proved to be feasible with comparable postoperative outcome to that of the laparoscopic procedure. Further clinical evaluation is deemed necessary.
Introduction
Laparoendoscopic single-site surgery (LESS) is a new approach in the field of minimally invasive surgery and laparoscopy. The feasibility and safety of LESS has been validated in many urologic procedures, and the experience is constantly increasing. 7 –11 To our knowledge, LESS bladder diverticulectomy has not been reported. We present our initial experience with the LESS approach to bladder diverticulectomy.
Patients and Methods
Four patients were treated by LESS bladder diverticulectomy without the use of any additional trocars between January 2009 and August 2009. Two experienced laparoscopists performed the procedures. The procedure took place for the management of diverticula that were associated with persistent symptoms from voiding problems with residual urine >100 mL (one patient) and recurrent infections (three patients). The history of the patients included three cases of benign prostatic hyperplasia, while one patient had a long history of posterior urethral stricture/bladder neck stenosis due to pelvic injury. The diagnosis was set by ultrasonography followed by cystoscopy or cystography. The median diameter of the diverticula was 8.5 cm (range 4–9 cm).
All patients were candidates for open or laparoscopic diverticulectomy. The possibility to perform LESS diverticulectomy was proposed to them, and informed consent was obtained in all cases. Preoperative evaluation included fluoroscopically monitored voiding cystography and endoscopic examination. Immediately before the procedure, cystoscopy was performed to access the diverticulum. A double-pigtail ureteral catheter was inserted in the ureter on the side of the diverticulum. In one case, double-pigtail ureteral stents were inserted bilaterally because of a diverticulum located between the orifices. An 18F urethral catheter was placed via guidewire, and its balloon was inflated into the diverticulum under fluoroscopic control.
Patient demographics, operative time, blood loss, catheterization period, perioperative complications, and the pathology result were recorded. Postoperative pain and analgesic medication required were evaluated by questionnaire. The perceived pain was noted by the patient on an analog pain scale with values that ranged from 1 to 10. Score 1 represented minimal pain while and Score 10, the worst possible pain. Data regarding the evaluation of pain were obtained three times daily starting on the postoperative day (POD) 1 and continued for the next three days (until POD 3). Administration of analgesic medication was recorded for the first 2 postoperative days. Cystography was performed on POD 8 or POD 9. The bladder catheter was removed if there was no leakage. Patients were called for follow-up at 1, 3, and 6 months and were evaluated with uroflowmetry and ultrasonography measurement of postvoid residual (PVR) urine.
Technique of LESS diverticulectomy
The technique of transperitoneal laparoscopic diverticulectomy has been previously described in detail. 1,5 The LESS approach is similar in concept to the laparoscopic procedure. For the performance of LESS diverticulectomy in the current population, the following equipment and technique were used:
Instruments (Fig. 1)

Schematic of prebent instruments and multichannel single incision trocar.
TriPort (Olympus Medical, Germany); 5-mm high-definition laparoscopic camera with 30-degree lens (EndoEye, Olympus Medical, Germany); prebent forceps (with teeth for grasping and flat for suturing) and scissors (Olympus Medical, Germany); and straight needle holder, forceps, scissors, and bipolar forceps (a prebent bipolar forceps was not available).
Patient positioning and trocar placement
The patient was placed in the supine position. The Trendenburg position of 15 to 20 degrees and inclination toward the surgeon should also be established (Fig. 2). The placement of the trocar was performed in the umbilicus. The method for the insertion of a TriPort has been previously described in detail. 12 Pneumoperitoneum was established, and the procedure took place transperitoneally. The diverticulum was distended by saline infusion. Incision of the peritoneum covering the bladder followed (Fig. 3a). The identification of the diverticulum was relatively easy because of the balloon of the catheter (Fig. 3b). Palpation of the balloon was also possible for the detection of the diverticulum.

Intraoperative patient positioning.

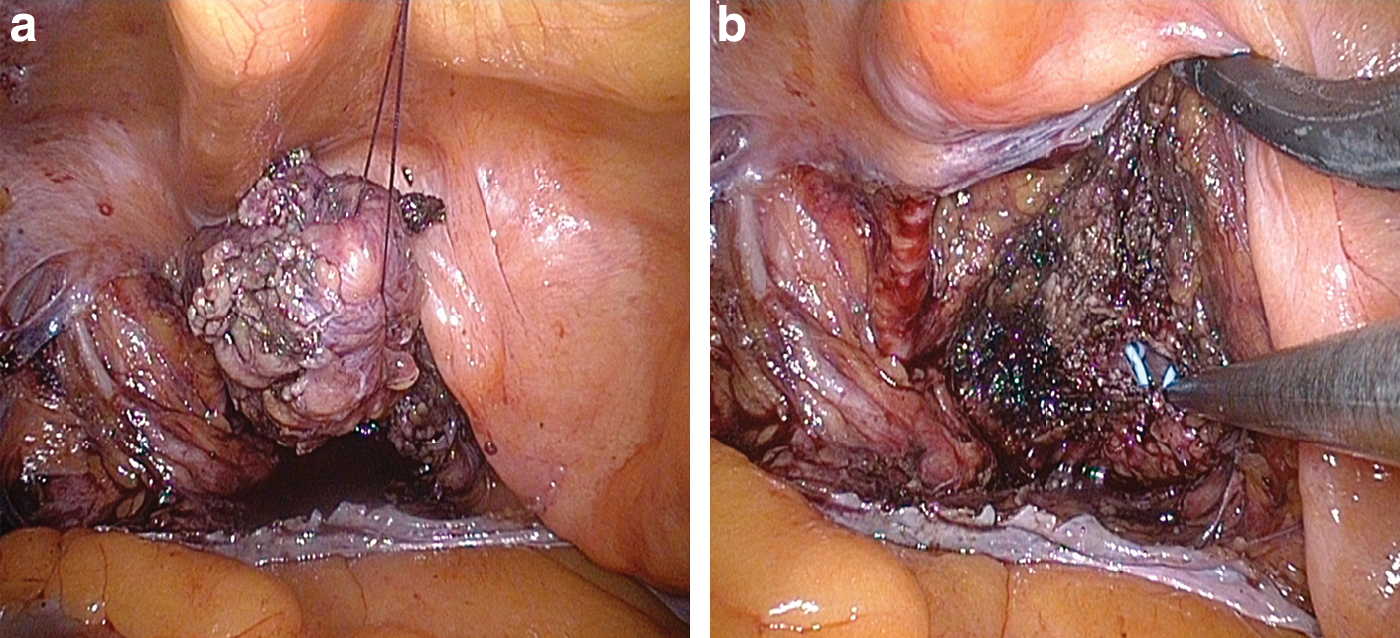
One prebent instrument was used for tissue retraction and exposure of the diverticulum. The dissection was performed by another instrument that was either prebent or straight (Fig. 4a). Incision of the diverticulum followed, and the balloon of the catheter was visible (Fig. 4b). The latter was deflated and removed to the bladder (Fig. 5a). The above maneuver facilitated the dissection of the diverticulum, because the latter could be visualized from outside and inside while the neck of the diverticulum was also identified.


The diverticulum was initially dissected ventrally, following circumferentially (Fig. 5b). The dissection of the posterior side of the diverticulum (especially the collum of the diverticulum) could be difficult. The dissection process was facilitated by fixing the diverticulum to the ventral abdominal wall (Fig. 6a). A long straight needle was passed from outside through the abdominal wall, stitched through the diverticulum and passed again through the abdominal wall. The suture was fixed on the outer side of the abdominal wall with the help of a clamp. When the diverticulum was completely dissected from the bladder wall (Fig. 6b), it was placed in an endoscopic retrieval bag. The ureteral stents are visible inside the bladder (Fig. 7b). The bag was closed and placed in the abdomen.
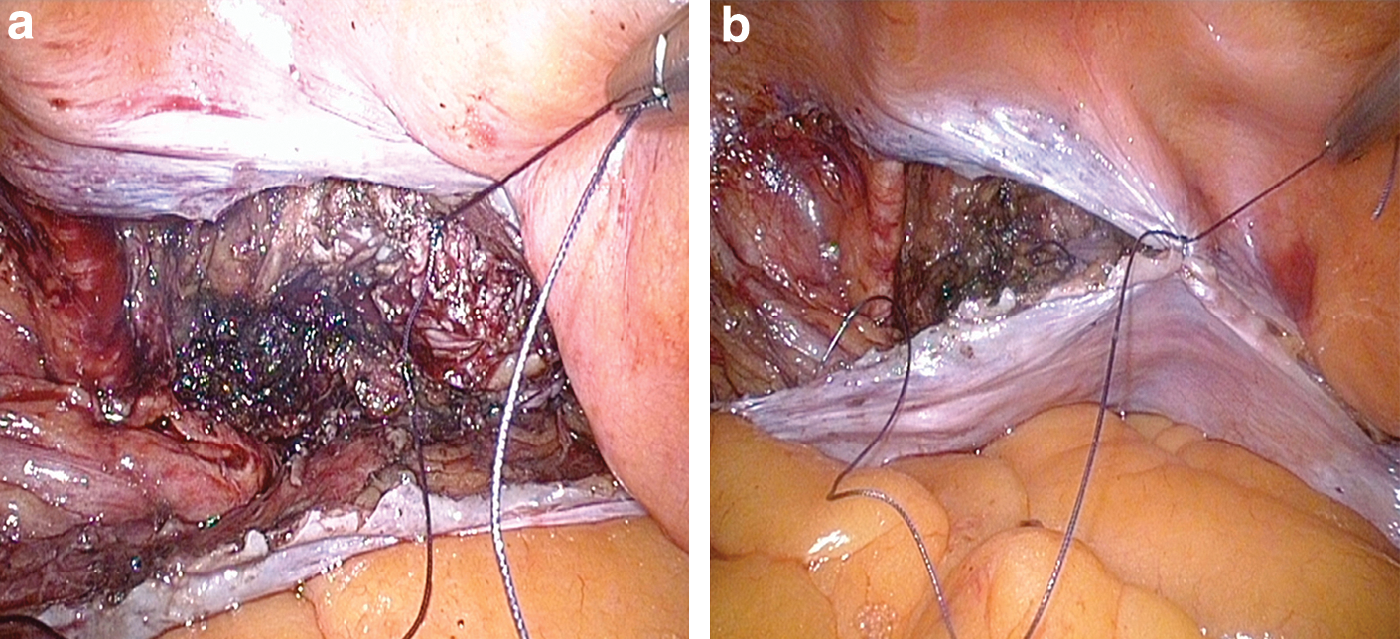
The bladder lesion was closed by interrupted sutures (2-0 Polysorb on a GU-46 needle or 2–0 Vicryl with UR-6 needle) (Figure 7a). Suturing of the bladder was performed with a straight needle holder and prebent forceps. Saline (200 mL) was infused in the bladder to identify any leakage. Any leakage could be managed by additional sutures. If the sutured bladder was watertight, the peritoneum was closed with running or interrupted sutures (Fig. 7b). A thin drain could be placed close to bladder wall into the extraperitoneal space according to the preference of the surgeon before the last suture was closed.
Finally, the endoscopic bag containing the diverticulum was grasped with straight forceps and retracted into the TriPort. The endoscopic bag and the TriPort were removed together. The umbilical incision was closed appropriately.
Results
The average patient age was 51 years (range 42–66 y) and the average body mass index was 26 kg/m2 (range 23.7–28.7 kg/m2). Operative time ranged between 101 minuntes and 154 minutes (median 130 min). Blood loss was minimal, with 150 mL to be the higher loss. Complications were not observed during the follow-up period. The catheter was removed on POD 8 in three patients and on POD 9 in one patient after the performance of cystography. Histologic examination did not reveal malignancy in the excised specimens. Postoperative pain evaluation results are presented in Table 1.
POD = postoperative day.
Discussion
Selection of the surgical approach for management of bladder diverticulum depends on several parameters, such as the size, number, location, and concomitant pathology associated with the diverticula. A small bladder diverticulum can be managed endoscopically by fulguration, 13,14 while a large diverticulum can be excised surgically either by the open or laparoscopic approach. The latter can be performed either an extraperitoneal or transperitoneal, extravesical, or intravesical technique. 1,2,5,15
In 1992, Parra and associates 1 were the first to report laparoscopic transperitoneal bladder diverticulectomy, while Nadler and colleagues 2 introduced the extraperitoneal laparoscopic approach. In the following years, several investigators reported their experience with laparoscopic bladder diverticulectomy. 3 –6,16 Laparoscopic diverticulectomy is considered safe and is accompanied by a clinical outcome similar to that of the open surgical approach. 6
Currently, reported laparoscopic experience with bladder diverticulectomy includes two series of 10 and 13 patients by Iselin and coworkers 17 and Abdel-Hakin and colleagues, 18 respectively. Operative time has been reported to range between 80 and 230 minutes while hospital stay ranges between 2 and 6 days. Similar results have been reported recently with robot-assisted laparoscopic bladder diverticulectomy, which required an average operative time of 178 minutes (range 163–235 min, including the setup of the robotic system). The experience included only five patients. Hospitalization period ranged between 1 and 6 days (average 3 days). 19 Complications regardless of the approach are minimal, because the majority of the investigators did not encounter any complications. Two cases of extravasation at the site of the vesical suture line were reported and were managed by additional urethral catheterization. 17,19
Laparoscopic or robot-assisted diverticulectomies have been performed in one session immediately after photoselective vaporization of the prostate (PVP). 20,21 Some investigators favor the performance of transurethral resection of the prostate (TURP) just before diverticulectomy, while others perform TURP a few days after the diverticulectomy, because there is a risk to the bladder incision closure sutures due to the need for continuous irrigation postoperatively. Moreover, the need for continuous irrigation after TURP and during the diverticulectomy may represent a difficulty, because the bladder can be inflated and deflated intraoperatively to facilitate dissection. 6,17,18 The performance of PVP minimizes the need for irrigation intraoperatively (diverticulectomy) and postoperatively, rendering the sequential management of benign prostatic hyperplasia and bladder diverticulum feasible and safe. 20
LESS has been introduced as a further development of minimally invasive surgery and laparoscopy. 8,22 LESS aims to combine the outcome of laparoscopy with decreased access-related morbidity, postoperative pain, hospital stay, and improved cosmetic outcome. The LESS approach uses a specially designed multichannel access port to introduce the instruments and laparoscopic camera through one incision. This incision can be cosmetically concealed, when appropriate, within the umbilicus. The experience with LESS has significantly expanded in recent years. The two largest series of LESS experience are reported by Desai and associates 10 and White and coworkers, 11 including more than 200 LESS procedures in total. We have also reported the initial experience with LESS tumor nephrectomy. 12 Most of the urologic procedures have been performed by the LESS approach. Nevertheless, LESS bladder diverticulectomy has not been reported in the literature.
The LESS approach has been associated with the aforementioned advantages, which remain questionable because the currently available data in the literature do not document any advantage of LESS over conventional laparoscopy other than the more desirable cosmetic outcome. 9,23 Nevertheless, Canes and associates 24 are investigators who observed faster convalescence in the patients who underwent left donor nephrectomy by LESS in comparison with the conventional laparoscopic approach.
In addition, needlescopic surgery represents another alternative approach of laparoscopic surgery. The needlescopic approach has been associated with lower morbidity in comparison with standard laparoscopy. Nevertheless, LESS is considered to possess an advantage in terms of cosmesis, which has not been documented yet. 25 To our knowledge, reports on needlescopic diverticulectomy are not available in literature.
The current study investigates the feasibility of LESS diverticulectomy, describes the technique, and reports the preliminary outcome of the procedure. The technique of the procedure is similar to that of transperitoneal laparoscopic bladder diverticulectomy. The access (trocar placement) is the only step of the procedure that is different. The inflation of a urethral catheter balloon in the diverticulum and occlusion of the neck of the diverticulum as well as its selective filling and emptying facilitated the identification of the diverticulum during the dissection of the peritoneum and the performance of the initial incision on the diverticulum. The insertion of the balloon catheter for the identification of the diverticulum has been previously proposed by other investigators and was proven to be helpful in the current series. 17,19 –21 Insertion of the double-pigtail ureteral stent in the ipsilateral to the diverticulum ureter provided visualization of the ureteral orifice. Thus, injuries of the ureteral orifice and ureter could be prevented. 17,19 –21
Operative time was similar to that of reported robot-assisted and laparoscopic series. The latter observation probably was influenced by the use of prebent instruments. Intraoperative ergonomic issues, such as instrument clashing and crossing, are significantly minimized by the use of prebent instruments. In fact, the design of prebent instruments provides more space outside the body of the patient for instrument movement, while the need to cross the instruments as they enter the port is an uncommon maneuver for these instruments in comparison with the flexible ones. In addition, the above instrumentation has rigid bent shafts that facilitate tissue retraction during dissection.
Nevertheless, these procedures were performed by two very experienced surgeons counting many hundreds of laparoscopic procedures. Thus, operative time was also influenced by the rapid adaptation of the surgeon to the LESS setting. Complications were not observed while blood loss was similar to that of the laparoscopic literature. 1 –6,17,18,20,21
Conclusion
LESS bladder diverticulectomy proved to be feasible with comparable postoperative outcome to that of the laparoscopic procedure. The use of prebent instruments improved intraoperative ergonomics. Further clinical evaluation and comparison with the laparoscopic bladder diverticulectomy would elucidate the advantages of the approach over laparoscopy.
Footnotes
Disclosure Statement
No competing financial interests exist.