
Abstract
Background and Purpose:
A benefit of miniaturized percutaneous nephrolithotomy (MPCNL) compared with conventional percutaneous nephrolithotomy (PCNL) has not been demonstrated as yet. Thus, the aim of this study was to evaluate the outcome of conventional vs MPCNL and to determine if MPCNL offers an advantage for the patient.
Patients and Methods:
A prospective, nonrandomized series of 50 consecutive patients with solitary calculi (lower pole or the renal pelvis) were treated either by conventional PCNL (26F) or MPCNL (18F). Ultrasound or holmium laser were used for lithotripsy. Patients were treated tubeless after uncomplicated MPCNL, with thrombin-matrix tract closure and antegrade Double-J catheter placement. After PCNL, all patients received 22F nephrostomies. Demographic data, stone characteristics, perioperative course, and complication rates were assessed.
Results:
Patients characteristics were comparable in both groups, except for stone size, which was 18 ± 8 mm (MPCNL) and 23 ± 9 (PCNL; P = 0.042). Operative time was comparable in both groups (48 ± 17 vs 57 ± 22 min, not significant [NS]). After MPCNL, 96% were stone free at day 1 vs 92% after PCNL (NS). Significant complications did not occur in both groups. Minor complications were: Fever, 12% (MPCNL) vs 20% (PCNL; NS); bleeding, 4% vs 8%; perforations, 0% vs 4% (all NS). Overall outcome was not influenced by body mass index. Calcium oxalate stones were predominant with 75%. Patients after tubeless MPCNL had less pain (visual analogue score, 3 ± 3 vs 4 ± 3; P = 0.048.) and needed slightly less additional pain medication (25 ± 12 mg/d vs 37 ± 10 mg/d piritramid; NS). Hospital stay was significantly shorter after MPCNL (3.8 ± 28 vs 6.9 ± 3.5 d; P = 0.021.).
Conclusions:
Both techniques were safe and effective for the management of renal calculi. While stone-free rates were comparable in our series, MPCNL showed advantages in terms of shorter hospital stay and postoperative pain. The lower stone burden and the tubeless fashion of MPCNL, however, might have influenced these results.
Introduction
Percutaneous nephrolithotomy (PCNL) is recommended as standard therapy for kidney stones >20 mm, while shockwave lithotripsy (SWL) is recommended for smaller renal calculi. 4,5 The stone clearance of lower-pole calculi after SWL is limited, however, thus leading to an extended indication for PCNL even for stones between 10 and 15 mm in many centers. 6 This trend is further promoted by the introduction of mini-PCNL (MPCNL), which is postulated to be less invasive compared with standard PCNL because of the miniaturized instruments. The perioperative morbidity and hospital stay may be further reduced by omitting the placement of a postoperative nephrostomy (tubeless MPCNL). 7 Although being logical at first glance, however, no clear advantage of the miniaturized equipment has been demonstrated yet, and some authors deny a benefit of MPCNL procedures. 8
The aim of our study was to evaluate the perioperative course of standard and tubeless MPCNL to determine if the use of MPCNL offers a benefit for the patient concerning perioperative morbidity and hospital stay.
Patients and Methods
In this prospective, nonrandomized study, 50 consecutive patients with solitary renal calculi that were located in the lower pole or renal pelvis were treated either by conventional PCNL (25 patients, 26F outer sheath, Karl Storz Endoscopes, Tuttlingen, Germany) or MPCNL (25 patients, 18F outer sheath, Karl Storz Endoscopes). Ultrasound (Calcuson, Karl Storz Endoscopes) or holmium laser probes (Auriga XL, StarMedTech, Starnberg, Germany) were used for lithotripsy. Preoperative imaging was performed either by radiography of the kidneys, ureters, and bladder (KUB)/intravenous urography or CT. For planning of the procedure, ultrasonographic examination was performed on the day before surgery.
Percutaneous access was established by a urologic surgeon (TK) by combined ultrasonographic and fluoroscopic imaging with the patient in the prone position. Tract dilation was performed by Alken telescope bougies for PCNL and single-step metal dilators for MPCNL (all Karl Storz Endoscopes). The techniques have been described in detail. 6,9,10
Patients were treated in a tubeless fashion after uncomplicated, stone-free MPCNL, with thrombin-matrix tract closure (Floseal, Baxter, Unterschleißheim, Germany) and antegrade Double-J catheter placement as described previously. 7 After standard PCNL, all patients received 22F nephrostomies. If primary MPCNL did not render the patient stone free, a 16F nephrostomy tube was placed to maintain access for a second-look MPCNL.
The following parameters were assessed prospectively: Age, sex, body mass index (BMI), stone size and location, operative time (excluding placement of an ureteral occlusion catheter), intraoperative and postoperative complications, stone analysis, stone-free rate (SFR) at day 1, postoperative pain (visual analogue scale [VAS], use of analgesics), and duration of hospital stay.
Urinary tract infection was excluded by dipstick analysis and urine microscopy before the procedure. All patients received antibiotics (ciprofloxacin or cotrimoxazole) for 5 days, starting on the day before surgery. For pain management, all patients received 2 × 75 mg Diclofenac or 3 × 500 mg metamizol orally. Further analgesics (7.5–15 mg intravenous Piritramid) were administered on demand.
Stone-free status was assessed endoscopically and by ultrasonography and KUB radiography at day 1 after tubeless MPCNL and nephrography in PCNL patients. Stone analysis was performed by infrared spectroscopy.
Statistical analysis was performed with SPSS Statistical Package for Social Sciences Version 14. The chi-square test was used for statistical testing. Regression analysis was performed for trend calculation. A statistical result was considered significant if P < 0.05, very significant if P < 0.01, and highly significant if P < 0.001. Power analysis was performed with Power on X (MMI Software, UK) for pain, pain medication, and complications (α-error 0.05, power 0.9).
Results
Patient characteristics were comparable in both groups, except for stone size, which was 18 ± 3.3 mm (MPCNL) and 22 ± 4.25 mm (PCNL; P = 0.042; Table 1). Operative time was comparable in both groups (49 ± 21.7 vs 59 ± 29.1 min, NS). After MPCNL, 96% (24/25) were stone free at day 1 compared with 92% (23/25) after conventional PCNL (NS). Patients with residual stones after the first procedure underwent a second PCNL to remove the remaining fragments within 5 days.
Not significant.
P = 0.042.
BMI = body mass index; PCNL = percutaneous nephrolithotomy; MPCNL = miniaturized percutaneous nephrolithotomy.
Significant complications did not occur in both groups (no blood transfusions or injury of other organs in both groups). Minor complications, including intraoperative or prolonged postoperative bleeding (4% vs 8%), fever (12% vs 20%, and perforations (0% vs 4%), were comparable in both groups; all NS; Tables 2 and 3).
Bleeding was considered as significant when leading to untimely termination of the procedure.
Not significant.
PCNL = percutaneous nephrolithotomy; MPCNL = miniaturized percutaneous nephrolithotomy.
All patients received orally 2 × 75 mg diclofenac or 3 × 500 mg metamizol. Further analgesics (7.5–30 mg piritramid intravenously) were administered on demand.
P = 0.048
Not significant.
VAS = visual analogue scale; PCNL = percutaneous nephrolithotomy; MPCNL = miniaturized percutaneous nephrolithotomy.
Overall outcome in terms of operative time, stone-free rate, and complications was not influenced by BMI. Postoperative pain, as measured on VAS on postoperative day 1, was lower after MPCNL (VAS: 3 ± 3 vs 4 ± 3; P = 0.048), and patients needed slightly less additional pain medication (25 ± 12 mg/d vs 37 ± 10 mg/d piritramid; NS; Table 3).
Stone analysis revealed 75% calcium oxalate stones (with 60% calcium oxalate monohydrate and 40% calcium oxalate dihydrate), 12% carbonapatite, 0.5% cystine, and 12% mixed calcium containing stones.
Hospital stay was significantly shorter after MPCNL (3.8 ± 2.1 vs 6.9 ± 2.9 d; P = 0.021, Figure 1).
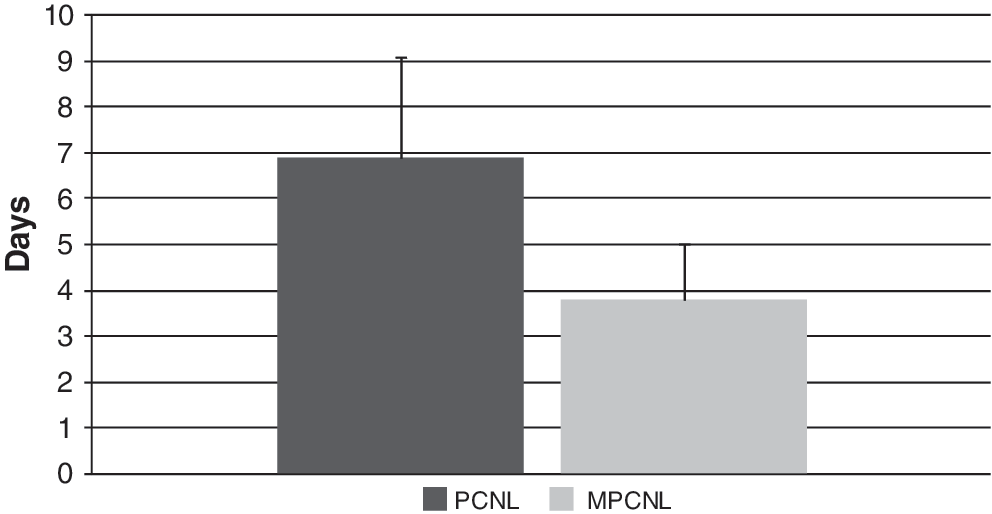
Length of hospital stay (days) after standard and tubeless miniaturized percutaneous nephrolithotomy (MPCNL). P = 0.021. PCNL = percutaneous nephrolithotomy.
Discussion
While PCNL is the treatment of choice for patients with renal calculi larger than 20 mm, 4 SWL is recommended for smaller renal calculi in most urolithiasis guidelines. 4,11 SWL, however, regularly necessitates repeated treatment sessions, and therefore time and patience are needed until complete stone clearance is achieved. In a substantial number of patients, residual fragments remain within the kidney. 12,13 Furthermore, SWL treatment of stones located in the lower pole often reaches unsatisfying SFRs. 14,15 On the other hand, several authors have demonstrated that PCNL achieves excellent SFR irrespective of stone burden and has reasonably low complication rates. 5,15,16 This has led to an expanded indication for PCNL, even for smaller calculi in many centers. 6
MPCNL was first described by Jackman and associates 17 for percutaneous nephrolithotomy in infants. The use in adults has been subsequently described by several groups. 6,10,18 Up to now, MPCNL has not been standardized, leading to the fact that sheath diameters below 20F are defined as miniaturized. In fact, Jackmanand colleagues 17 described a technique using an 11F access tract, while Nagele and coworkers 6,10 use 18F and Lahme and associates 18 use 15F.
The idea of using miniaturized instruments was based on the assumption of lower morbidity from reduced tract dilation and less renal trauma. Nevertheless, such an advantage of MPCNL has been described only in infants. 19 The reduced sheath diameter, however, causes major disadvantages because irrigation flow is limited and more extensive stone fragmentation is necessary, leading to prolonged operative times. 8 MPCNL has therefore, apart from some specialized centers, not become a standard procedure in adults.
Giusti and colleagues 8 performed a retrospective comparison of standard vs MPCNL. They demonstrated a lower SFR despite longer operative times in the MPCNL group. Nevertheless, the MPCNL patients had a lower hematocrit drop and, in contrast to the conventional PCNL group, did not need blood transfusions. Although it is surprising that a smaller shaft diameter leads to longer operative times and potentially lower SFR, the reduced hematocrit drop may support the improved minimally invasive nature of miniaturized instruments. Consequently, Li and coworkers 20 prospectively evaluated the systemic response to PCNL (30F) and MPCNL (14F–18F). 20 Based on experimental findings that acute phase reactions are proportional to surgery-induced tissue damage, they perioperatively measured acute phase markers such as tumor necrosis factor-α, interleukin-6/10, and C-reactive protein. The results, however, could not confirm their assumption and failed to demonstrate significant advantages in terms of a lower invasiveness. The benefit of MPCNL remains, therefore, undefined, which is why it is not explicitly mentioned by international guidelines.
The aim of this prospective “real life” series was to compare the perioperative and postoperative outcome of conventional vs tubeless MPCNL for renal calculi. In our series, both conventional PCNL and tubeless MPCNL were effective and safe procedures. While complications were comparably rare in both groups, MPCNL demonstrated efficacy equal to conventional PCNL. This is in contrast to the series of Giusti and associates 21 and may be attributed to the lower stone burden in our series. There was an expected tendency to longer operative times despite the smaller stone mass for MPCNL because of the necessity for more extensive stone fragmentation. The length of hospital stay was significantly shorter for the tubeless MPCNL procedure. Whether the shorter hospital stay was determined by the use of the miniaturized equipment or the omitted nephrostomy tube cannot be distinguished. Interestingly, Giusti and colleagues 8 reported a shorter hospital stay after MPCNL compared with conventional PCNL. 8 After tubeless conventional PCNL, however, hospital stay was shortest.
In our opinion, it has to be mentioned that tubeless PCNL does not mean fully tubeless in most series. In contrast, most surgeons do place Double-J catheters instead of percutaneous tubes, with only few reports on true tubeless procedures. 22 –25 Many reports demonstrated the safety of tubeless PCNL after uncomplicated procedures in stone-free patients. 26 –31 While many authors aimed to launch tubeless PCNL as the new standard, the disadvantages have to be considered: The access is lost to remove residual calculi, and bleeding or fever may cause significant problems with the need for further adjunctive procedures. Furthermore, the removal of the Double-J catheter necessitates an, at least for males, uncomfortable cystoscopy. This is the reason the value of tubeless PCNL has been questioned recently. Mishra and coworkers 32 demonstrated in a randomized study that early removal of the nephrostomy results in an equivalent analgesic requirement and decrease in hemoglobin and hospital stay as tubeless PCNL and a lower incidence of hematuria.
Tubeless procedures might have a substantial impact on postoperative pain. Desai and associates 33 demonstrated a negative correlation of nephrostomy size and postoperative demand for analgesics. Lowest pain scores were achieved when placement of a nephrostomy tube was omitted. These findings were confirmed by others, including this series. 34 Pain and consecutively necessary pain medication were lower in the tubeless MPCNL group. The morbidity of Double-J catheters, however, can be significant. Shah and coworkers 34 reported stent-related discomfort in 39% of patients. This is in accordance with other studies. 35 –37 In our opinion, true tubeless PCNL should be performed to achieve best results in terms of pain. The price of losing renal access and having the risk of urine outflow obstruction has to be paid, however.
Although MPCNL showed advantages in terms of VAS, further studies have to evaluate whether this observation was because of the replacement of the nephrostomy by a Double-J catheter or by the reduced shaft diameter of the miniaturized equipment.
We used the same technique for tubeless MPCNL as described by Nagele and associates, 7,38 including sealing of the tract by gelatin-thrombin matrix. 7,38 In our experience, closure of the tract prevents bleeding and urine extravasation. The group at the University of California, Irvine, confirmed effective hemostasis and watertight tract closure. 39 Uribe and associates 40 demonstrated in an in-vitro setting that gelatin-thrombin matrix remains a fine particulate suspension in normal and sanguine urine while other sealants form stable solid clots that may obstruct the collecting system. The necessity for hemostatic tract closure, however, is still a controversy that has not been demonstrated in a comparative study.
A PubMed review by Michel and coworkers 41 reported a regular occurrence of major complications, such as transfusions (11.2%–17.5%), septicemia (0.3%–4.7%), and colonic (0.2%–0.8%) or pleural injuries (0.0%–3.1%). In this series, major complications were not seen, confirming earlier reports of our group. 5 While we believe that the combination of experience, puncture by the urologist, and combined ultrasonographic-fluoroscopic guidance for puncture account for these excellent safety results, the use of miniaturized instruments seems to have a minor impact.
A major drawback of our comparative study is the different stone size in the PCNL and MPCNL groups. Smaller solitary renal calculi were managed by MPCNL while larger renal calculi were managed by conventional PCNL. Despite the smaller stone mass, however, MPCNL produced longer operative times than conventional PCNL. Furthermore, the impact of the tubeless fashion of MPCNL has to be evaluated in future studies. Another possible conclusion that should be investigated is the combination of larger shaft diameters with tract sealing, possibly leading to shorter operative times, less pain, and shorter hospital stay.
It is important to advise investigators of upcoming randomized studies to choose well-calculated sample sizes. If focusing mainly on complications rather than stone removal, little differences in postoperative pain, pain medication, and overall complications were observed in our series. Assuming that a difference of 10% is of clinical significance, a group size of about 100 patients is necessary to avoid underpowered results. Because such case series for PCNL are hard to collect in single centers, this may support the formation of multicenter groups.
Conclusion
We could demonstrate that conventional and MPCNL are both safe and effective procedures for the treatment of renal calculi. The shorter hospital stay and less postoperative pain may support the use of MPCNL for smaller and intermediate sized stones. The lower stone burden and the tubeless fashion of MPCNL, however, might have influenced these results.
Footnotes
Disclosure Statement
No competing financial interests exist.