
Abstract
Background and Purpose:
According to the Randall plaque theory, urinary crystals may attach to focal interstitial deposits of calcium phosphate (CaP), localized in the tip of the renal papillae. The aim of this prospective study was to evaluate the feasibility and safety of papillary biopsy, performed during ureterorenoscopy (URS) or percutaneous nephrolithotomy (PCNL), to obtain, in vivo, appropriate samples to investigate interstitial CaP deposits that represent Randall's plaques precursors.
Patients and Methods:
Twenty-eight patients who were affected by recurrent renal stones, 13 males and 15 females, with a median age of 42.5 years (range 17–76 y), underwent rigid and/or flexible URS (8 paients) or PCNLs (20 patients). In all cases, endoscopic biopsies from renal papillae were performed. Papillary samples were obtained by means of 3F or 4F cup biopsy forceps if semirigid and flexible ureterorenoscopes were used. During percutaneous procedures, with rigid and flexible instruments, 5F or 10F cup forceps were used. The same pathologist analyzed all the histologic specimens.
Results:
All patients underwent successful biopsy procedures. The quality of the obtained tissue allowed for an accurate histochemical analysis in 27 of 28 (96.4%) biopsies. One biopsy was inadequate because of some important regressive phenomena. No specific complications had to be attributed to biopsy procedures.
Conclusions:
Percutaneous or transureteral biopsies of renal papillae resulted in being safe and appropriate procedures to obtain papillary samples to identify the presence of interstitial calcium deposits. In the light of the low number of inadequate biopsies, it can be concluded that no difference was found between the percutaneous and transureteral bioptic approach.
Introduction
In the last decade, the Randall plaque theory has been a matter of considerable interest, and several studies have investigated and discussed the possible pathogenetic role of those plaques and their involvement in idiopathic CaOx lithogenesis. 3 –11
Early studies focused their goals on creating the physiologic conditions for Randall plaques development using animals or cultured cell lines, 12 –18 even if their validity and applicability to the idiopathic CaOx lithogenesis in humans are doubtful. Unfortunately, there is no animal model that carries papillary calcifications similar to that of the Randall plaque. 19 Ideal studies should focus on crystal deposition in renal papillary tissue from well-characterized, living human stone formers, addressing the research on what structures and in response to what forces those crystals may be deposited.
According to these considerations, performing biopsies from human renal papillae, in vivo, seems mandatory if the purpose is to obtain adequate samples for histologic evaluations. In turn, that is necessary to investigate the pathophysiology of calcium nephrolithiasis. As a matter of fact, the recent breakthrough in renal stone research has been obtained by the Indianapolis group after they introduced the technique of papillary biopsy through percutaneous nephrolithotomy (PCNL) access to the renal pelvis as an investigative tool. 3,4,7 –9,20 According to Kuo and associates, 20 the technique was safe, and no significant hemorrhagic problem or renal dysfunction occurred.
Because of the increasing use of ureterorenoscopy (URS) to treat renal stones, in this study we evaluated the feasibility and safety of papillary biopsy performed during URS vs PCNL. We addressed in particular the appropriateness of tissue samples for research of interstitial CaP deposits, which, according to Evan and colleagues, 7 represent Randall plaques precursors.
Patients and Methods
Prospectively, 28 consecutive patients who were affected by renal stones were analyzed: 13 were males and 15 females. The median age was 42.5 years, with a range of 17 to 76 years. They underwent PCNL or URS with lithotripsy: Before ending the procedure, forceps biopsy of a renal papilla was performed.
The study protocol was approved by the Ethical Committee of the University Hospital of Verona. Each patient signed an informed consent regarding the endoscopic procedure and the adjunctive biopsy. Exclusion criteria from this study included patients who presented with stones that were associated with urinary infection that wasdetected by a preoperative urine culture because of the potential risk of increased morbidity. Patients with previous coagulation disorders were also excluded.
All subjects had radiopaque renal stones or had previously passed calcium stones. No patients had a history of intestinal bypass or resection, potentially responsible for an increased oxalate adsorption and consequently greater urinary excretion of oxalate. No patient had long immobilization periods, sarcoidosis, hypervitaminosis D, and milk-alkali syndrome, likewise responsible for increased urinary calcium excretion. On the other hand, two patients had primary hyperparathyroidism and one had distal tubular familial acidosis. Thus, 26 of 28 patients were primary calcium stone formers.
Because of stone burden and number, PCNL was performed in 20 (71.4%) patients and URS in the remaining 8 (28.6%) patients, applying our standard techniques. PCNLs were performed using 26F rigid and/or 15.5F flexible nephroscopes, and lithotripsy was obtained using ultrasonic, pneumaticm or holmium:yttrium-aluminum-garnet (Ho:YAG) laser devices, whereas 8F or 9.5F rigid and/or 7.5F flexible ureterorenoscopes and Ho:YAG laser were used to perform URS.
After the removal of the stone(s), renal papillae were carefully inspected using both rigid and flexible endoscopes, to map their appearance and identify the presence of white areas, characterizing the endoscopic aspect of the Randall plaques. Papillary samples were obtained from the whitish areas (Fig. 1), when present, or from the papillary tip when the white areas were not evident. According to the type, 3F or 4F flexible or rigid ureteroscopes, and 5F or 10F, if flexible or rigid nephroscopes, cup biopsy forceps were used, respectively. One to 3 biopsies were obtained per papilla, one papilla per patient biopsied; this was similar for both ureteroscopic and percutaneous procedures. Multiple biopsies performed in a single patient were sent for histopathologic analysis as a single specimen.

Endoscopic image of Randall plaques in a primary calcium-oxalate stone former that was obtained during flexible ureterorenoscopy. Plaques are visualized as whitish irregular areas that are localized at the tip of the renal papilla.
In all the patients who underwent URS, the transureteral biopsies were obtained from the upper caliceal papillae. Biopsing the upper caliceal papillae was necessary in case of use of the semirigid ureteroscope and preferable when the flexible one was used, to avoid dangerous deflection of the tip of the instrument, when the 3F biopsy forceps was inserted. In the case of the percutaneous approach, biopsy samples were obtained from the upper caliceal papillae in seven cases, from the middle in six, and the lower in the remaining seven cases.
After the biopsy, all sites were examined to verify the absence of significant bleeding. Biopsy samples were immediately placed in 4% paraformaldehyde solution. The same pathologist analyzed all the histologic specimens. The von Kossa staining method was used to disclose calcium deposits.
Preoperative and postoperative hemoglobin (Hb) and hematocrit (Hct) values were obtained, as were serum creatinine values, preoperatively, postoperative, and at 3 months postoperatively; adverse events and hospitalization were analyzed to document the incidence of complications related to the adjunctive maneuver. Moreover, these data were compared to that registered in a concurrent control group of those who had undergone URS (76 patients) or PCNL (42 patients) and lithotripsy with no papillary biopsies in the same period.
Statistical analyses
Data are reported as medians with interquartile range, because of the skewed distribution of Hb, Hct, and serum creatinine values. Statistical analyses were performed by Mann-Whitney test to compare two independent samples and Wilcoxon test to compare two related values. The Friedman test (nonparametric repeated measure analysis of variance) was used to assess the overall differences in creatinine value distributions across all the periods considered. A P value ≤0.05 was considered significant. Statistical analyses were performed using SPSS software, release 12.0.
Results
The endoscopic biopsy protocol was successfully concluded in all patients included in the study. Spontaneous hemostasis in biopsy areas was rapid and complete: consequently, no patients needed further hemostatic interventions, such as cauterization, to control eventual bleeding from the biopsy sites (Fig. 2).

Every specimen achieved via the percutaneous approach and seven of eight bioptic samples obtained through URS were of sufficient quality and size to allow for the histochemical staining of the interstitial calcium deposits and accurate histopathologic analysis (Fig. 2). Histochemical aspects related to calcium microdeposits were found even in the remaining sample obtained, during semirigid URS, with the 4F cup biopsy forceps; however, this specimen was inadequate for a definitive analysis because of important buckling regressive phenomena (3.6% of cases).
All patients who had undergone URS had an uneventful hospital course, with a median hospitalization time of 2 days (range 1–3 d). In the PCNL group, two patients had a temperature of <38°C and one >38°C in the immediate postoperative period. Nevertheless, they rapidly recovered without any further problems. Moreover, no patients reported adverse sequellae, such as delayed bleeding or significant pain necessitating longer or rehospitalization. The median hospitalization time in this group of patients was 5 days (range 3–7 d).
Likewise, preliminary analysis of blood parameters showed the persistent normality of these variables after endoscopic surgery. No significant differences were registered between preoperative and postoperative serum creatinine levels in each group of patients across all periods considered (Table 1). Although the differences between preoperative and postoperative values of Hb and Hct just reached statistical significances (P < 0.001) in both procedures, they did not translate into significant clinical changes (Table 2). Indeed, no patients needed hemotransfusion in the postoperative period. In analyzing the control group of patients, no difference was registered between preoperative and postoperative serum creatinine levels, while the same statistical but not clinical significant differences regarding Hct and Hb were observed (Table 2). Furthermore, comparing the clinical findings in the study group to that registered in the control cases, no statistically significant differences were detected (Table 3). Therefore, Hct and Hb decreases were not attributable to the bioptic procedure.
IQR = interquartile range; PCNL = percutaneous nephrolithotomy; NS = not significant; URS = ureterorenoscopy.
Although statistically significant (Wilcoxon test), changes were not clinically significant.
IQR = interquartile range; PCNL = percutaneous nephrolithotomy; URS = ureterorenoscopy.
Hct = hematocrit; IQR = interquartile range; Hb = hemoglobin; PCNL = percutaneous nephrolithotomy; NS = not significant; URS = ureterorenoscopy.
Finally, analyses of Δ Hct and Δ Hb showed significant differences between subjects who had undergone PCNLs or URSs and papillary biopsies, comparable to that achieved in the control group of patients. Therefore, these differences were exclusively from the different invasivity of the endourologic procedures (Fig. 3).
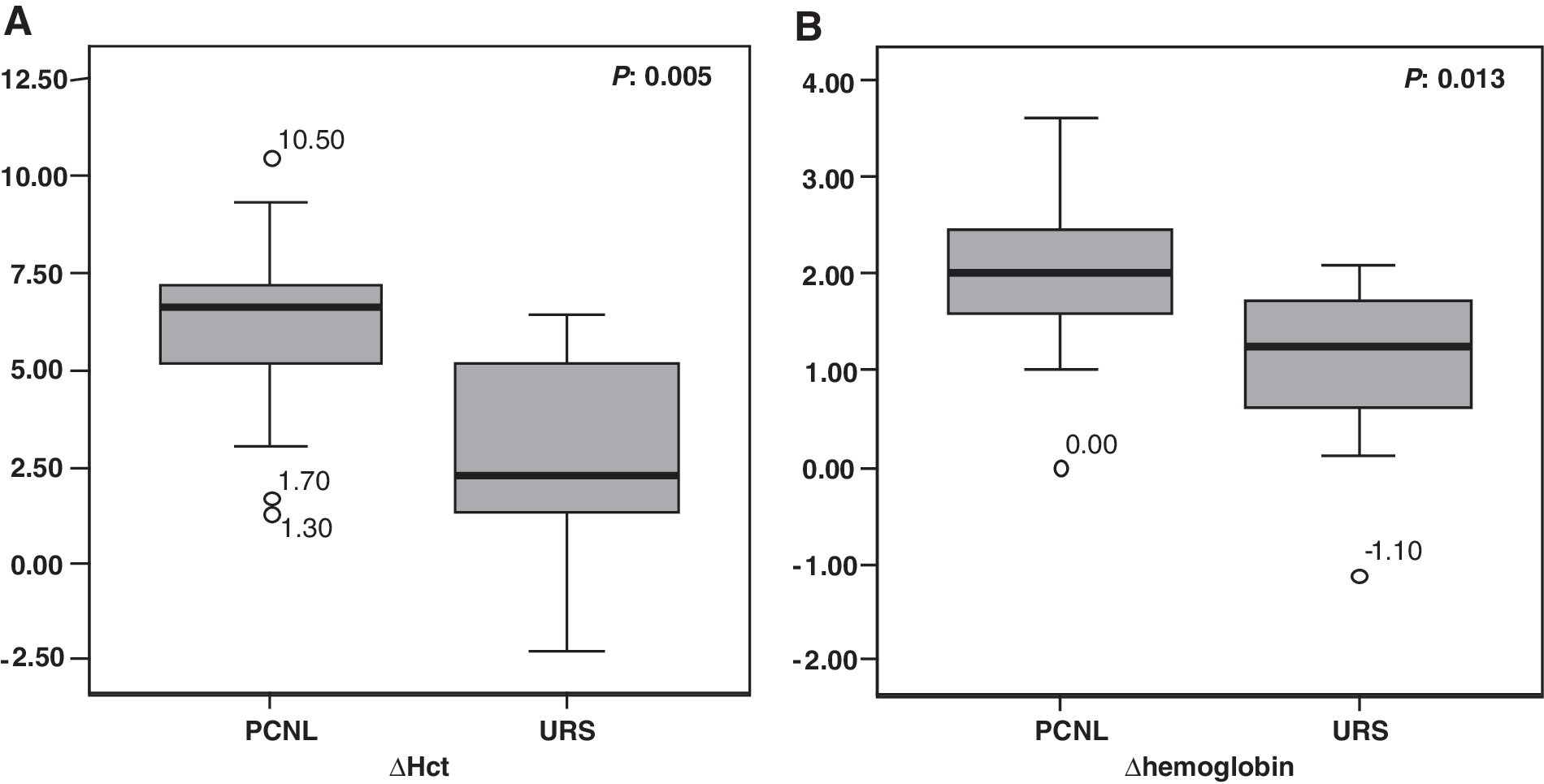
Boxplot for Δhematocrit
Discussion
Idiopathic CaOx stones represent the most frequent type of human urolithiasis. In 1937, Randall, approaching autoptic kidney studies, hypothesized that CaOx stones were formed from irregular and whitish areas, underlying urothelium and localized on the tip of renal papillae (the homonymous plaques), constituted by deposits of hydroxyapatite crystals located in the basement membranes of thin Henle loops. Recently, heterogeneous papillary pathologic findings have been described in different forms of calcium nephrolithiasis and a pathogenetic role of typical Randall plaques in idiopathic CaOx lithogenesis has been proposed. 3 –11
To investigate the relationship between the Randall plaque and its precursors with the different forms of calcium lithogenesis, we planned in an ongoing project (1) to collect the renal papillary tissue, with the aim of identifying the characteristic histologic lesions; (2) to investigate the papillary tissue by means of molecular biology techniques, and (3) to characterize patients with stones as in depth as possible with metabolic studies and crystallographic analysis of removed stones.
Today, renal papillae are reached easily using an endoscopic approach. Continuous improvements in the field of rigid and flexible endourologic instruments and ancillary devices has allowed us to access and visualize all renal collecting system, minimizing the potential morbidity of the procedures and extending the endourologic applications. 21 Moreover, the working channel of these instruments accommodates, at least, 3F caliber biopsy forceps, which are able to remove a sufficient amount of papillary tissue. Therefore, percutaneous as well as transureteral approaches seem to satisfy the need of safely and efficiently obtain tissue samples from selected renal papillae.
To our knowledge, Kuo and coworkers 20 were the only ones who had previously analyzed the feasibility and safety of renal papilla biopsies. They limited their evaluation, however, only to the bioptic procedures during PCNL. They focused their attention on the absence of significant bleeding and on the need of hemotransfusions as well as on the absence of significant clinical changes in mean renal function between preoperative and postoperative periods.
In the framework of the above ongoing research project, with the aim of expanding the possibility to obtain valuable papillary biopsies, we have investigated their collection during ureteroscopy. No studies regarding feasibility and safety of the URS papillary biopsy that aim to identify Randall plaques are available so far in literature.
As a result of our evaluation, both endoscopic percutaneous and transureteral biopsies have been shown to be minimally invasive, safe, and able to obtain samples of sufficient quality and size to allow for an accurate histopathologic analysis. Such a relatively safe procedure seems to reflect and confirm that renal papillae have limited blood flow; as a consequence, bleeding after biopsy appears to be quite modest. Although the biopsy forceps used during URS are thinner than those used during PCNL, leading to smaller biopsies (approximately 1 mm in maximum diameter), the tissue was sufficient in quantity and of good quality for pathologic examination. As a matter of fact, only one specimen obtained via URS was not appropriate for histologic examination.
In our study, von Kossa staining was used to reveal crystalline deposit sites that were localized in basement membranes of the thin loops of Henle (Fig. 2), because it was the calcium staining method usually applied by our pathologist. Although the Yasue method could be a better method to find plaque, von Kossa staining remains one of the most valid and widely used methods to identify in sections the calcium anions, such as in calcium phosphate 22 that represent the interstitial Randall plaque precursors.
It was not the aim of this study to describe the relationship of Randall plaque and its interstitial precursors with renal stones; to address this issue, we need to expand and investigate our case population as outlined above in the ongoing research project. It is interesting to observe, however, that crystalline calcium deposits that were localized in basement membranes of the thin Henle loops similar to those described by Evan and associates 7 have been observed in paients with primary CaOx recurrent stones (Fig. 2D).
Investigations on the pathology of the papilla, together with the assessment of the extension of the Randall plaques, the metabolic evaluation, and the analysis of the crystal nature of stones will hopefully lead to pinpointing a correct understanding of the stone disease heterogeneity. This should potentially guide the approach to patients with stones in a more rational way: Perhaps identifying those who are at high risk of recurrence, or to develop renal failure; perhaps identifying new pathogenetic treatments. We believe that in the framework of a comprehensive research project, it is ethically acceptable to perform renal papillary biopsies, a very safe procedure, in patients who need stone removal.
Conclusions
Our study confirms that both percutaneous or transureteral biopsy of renal papillae represents a safe and appropriate procedure to obtain papillary samples to evaluate interstitial calcium deposits. Indeed, patients had no complications attributable to bioptic procedures. In our hands, the endoscopic biopsy protocol provided tissue of excellent quality for our scientific purposes. Furthermore, according to the low number of inadequate histologic specimens, no difference was found between the percutaneous and transureteral approach.
Footnotes
Disclosure Statement
No competing financial interests exist.