
Abstract
Background:
The incidence of urolithiasis is twofold to threefold higher in men than in women. Several animal studies have suggested an association between testosterone levels and the formation of kidney stones. Specifically, castration has been shown to decrease stone formation in rat models. The association between testosterone and stone formation in humans, however, has not been well investigated.
Patients and Methods:
Early morning total and free testosterone levels were recorded for 55 male patients. Participants completed a demographics questionnaire, and clinical records of enrolled subjects were reviewed. When available, stone composition was determined in the stone formers. Mann-Whitney tests and logistic regression models were used to examine the data.
Results:
Of the 55 patients, 25 had no history of urolithiasis and 30 had a history of urolithiasis. Although the differences between the two groups were not statistically significant, the stone formers compared with stone-free controls tended to be older (median age 48.4 vs 36.5 years, P = 0.072) and have higher serum levels of testosterone (median serum concentration 384 vs 346 ng/dL, P = 0.112). In the multivariate analyses, after adjusting for age and body mass index, the testosterone-related odds ratio was 1.004 with a corresponding P value 0.051.
Conclusions:
Male stone formers were found to have higher serum total testosterone levels compared with a similar cohort without stones. This result is consistent with several animal models that have demonstrated that testosterone is a risk factor for stone formation. Our findings warrant confirmation in a larger, prospective study. There are potential therapeutic implications if testosterone is found to be a risk factor in urolithogenesis.
Introduction
It is well established that urolithiasis occurs with greater frequency in males. The relative frequency has been noted to be three times that of women in multiple studies, and the rate of formation of idiopathic calcium stones has been reported to be four to five times higher in men than in women. 6 –10 This sexual disparity seems to be influenced by age. Interestingly, stone formation in the prepubescent population is similar between males and females. 11 The greatest difference in idiopathic calcium oxalate stone formation is seen in the third and fourth decade of life. 12 In the sixth decade of life, stone incidence, as well as testosterone levels, begin to decline in men. 13 –15 Each of these observations supports a role for sex hormones in lithogenesis. In addition, experimental studies in rats have demonstrated both that testosterone promotes stone formation and that estrogen inhibits stone formation, although the mechanisms remain unclear. 16,17
Our hypothesis is that higher serum testosterone levels are a risk factor for the development of urolithiasis. As such, we sought to prospectively test whether total and free serum testosterone levels were higher in male stone formers compared with a similar control cohort of nonstone-formers.
Patients and Methods
Enrollment of study subjects
Fifty-five men older than 18 years were enrolled in this study that was approved by the Emory University Institutional Review Board. All subjects were prospectively enrolled at the department of urology in the Emory Clinic from April 2006 to January 2010. Thirty of the subjects had a history of calcium-oxalate stones (stone formers) and 25 had no history of stones (controls). Patients were excluded from the study if they had primary hyperparathyroidism, chronic diarrheal syndromes, intestinal malabsorption, complete distal renal tubular acidosis, primary hyperoxaluria, recurrent or active urinary tract infection, history of kidney transplantation, ongoing 5-α reductase inhibitor therapy, liver disease, primary gout, any debilitating chronic illness, or a calculated creatinine clearance of ≤50 mL/minute.
Study protocol
One serum sample was drawn from each subject in the morning between 8AM and 11 AM. All patients underwent anthropometric measurements that allowed calculation of their body mass index (BMI). Patients were asked to self-identify their race/ethnicity and to complete a health questionnaire, which inquired about the family history of urolithiasis.
Assays
Blood samples were centrifuged immediately and stored at 2°C to 3°C until assayed. Serum total testosterone was analyzed by Quest laboratory (San Juan Capistrano, CA) by using turbulent flow liquid chromatography tandem mass spectrometry 18 and percent free was assessed by tracer equilibrium dialysis. 19 From these data, the free testosterone level was calculated.
Statistical analysis
The distributions of variables under study were compared in the two groups (urolithiasis patients and controls) using the Mann-Whitney rank sum test for continuous variables and the chi-square test for categorical variables. Logistic regression analyses were performed to examine the association between testosterone and kidney stones while controlling for possible confounding because of differences in age and BMI between the groups. The results of the logistic regression analyses were expressed as odds ratios (OR) accompanied by 95% confidence intervals (CI) and P values. All statistical analysis was performed using SPSS (version 17.0) software (SPSS, Inc, Chicago, IL).
Results
As shown in Table 1, stone-forming patients were not statistically different from the stone-free controls with respect to ethnicity (76.7 vs 76.0% of non-Hispanic whites, P = 0.954) and family history of kidney stones (53.3% vs 44.0%, P = 0.491). The median BMI was 26.8 kg/m2 among patients with a history of stones and 26.6 kg/m2 among controls (P = 0.389). Although none of the differences between the two groups were statistically significant, the stone-forming patients compared with stone-free controls were older (median age 48.4 vs 36.5 years, P = 0.072) and had higher serum levels of testosterone (median serum concentration 384 vs 346 ng/dL, P = 0.112). In contrast to the total testosterone results, there was no difference with respect to free serum testosterone (P = 0.919).
Based on Mann-Whitney test for continuous variables and chi-square test for dichotomous variables.
BMI = body mass index.
In the multivariate analyses, after adjusting for age and BMI, the testosterone-related OR was 1.004 (95% CI: 1.000–1.009) with a corresponding P value of 0.051 (Table 2). This reflects an increase in the likelihood of being a stone former for each increase of one unit of ng/dL of serum total testosterone. The OR shown for age and BMI are not statistically significant.
Logistic regression model includes all variables in the table.
odds ratio reflects increase in the likelihood of kidney stone per unit of each variable.
OR = odds ratio; CI = confidence interval; BMI = body mass index.
Discussion
Early investigations into the differences in stone formation between sexes noted that men had a higher rate of urinary excretion of oxalate, 2,20 an important promoter of lithogenesis, and women had a higher rate of urinary excretion of citrate, 21 –23 an important inhibitor of lithogenesis. Recent work has begun to elucidate possible mechanisms by which testosterone may affect these and other pathways leading to urolithogenesis.
Sex hormones are thought to alter oxalate metabolism, leading to increased lithogenesis in men (Fig. 1). Glycolic acid oxidase (GAO) is an oxalate-producing enzyme that is part of the pathway in converting ethylene glycol to oxalate. Richardson and associates 24 showed that testosterone increases the activity of GAO by an unclear mechanism. Conversely, estrodiol has been shown to decrease GAO activity. 25 Lee and colleagues 16,17 compared the rate of calcium oxalate stone formation of normal male rats, castrated male rates, normal female rats, and castrated female rats fed a lithogenic ethylene glycol diet. They found that uncastrated male rats excreted the highest levels of oxalate and the uncastrated female rats excreted the lowest levels. Not surprisingly, cases of urolithiasis occurred in the ethylene glycol fed intact male rats but not female rats. In addition, castration of male rats dramatically decreased the incidence of renal stones. Furthermore, subcutaneous implantation of exogenous testosterone restored calcium oxalate stone formation in postorchiectomy male rats and enhanced stone formation in intact female rats. The authors state that these findings support the hypothesis that testosterone plays a determinant role in the pathogenesis of calcium oxalate stone formation.
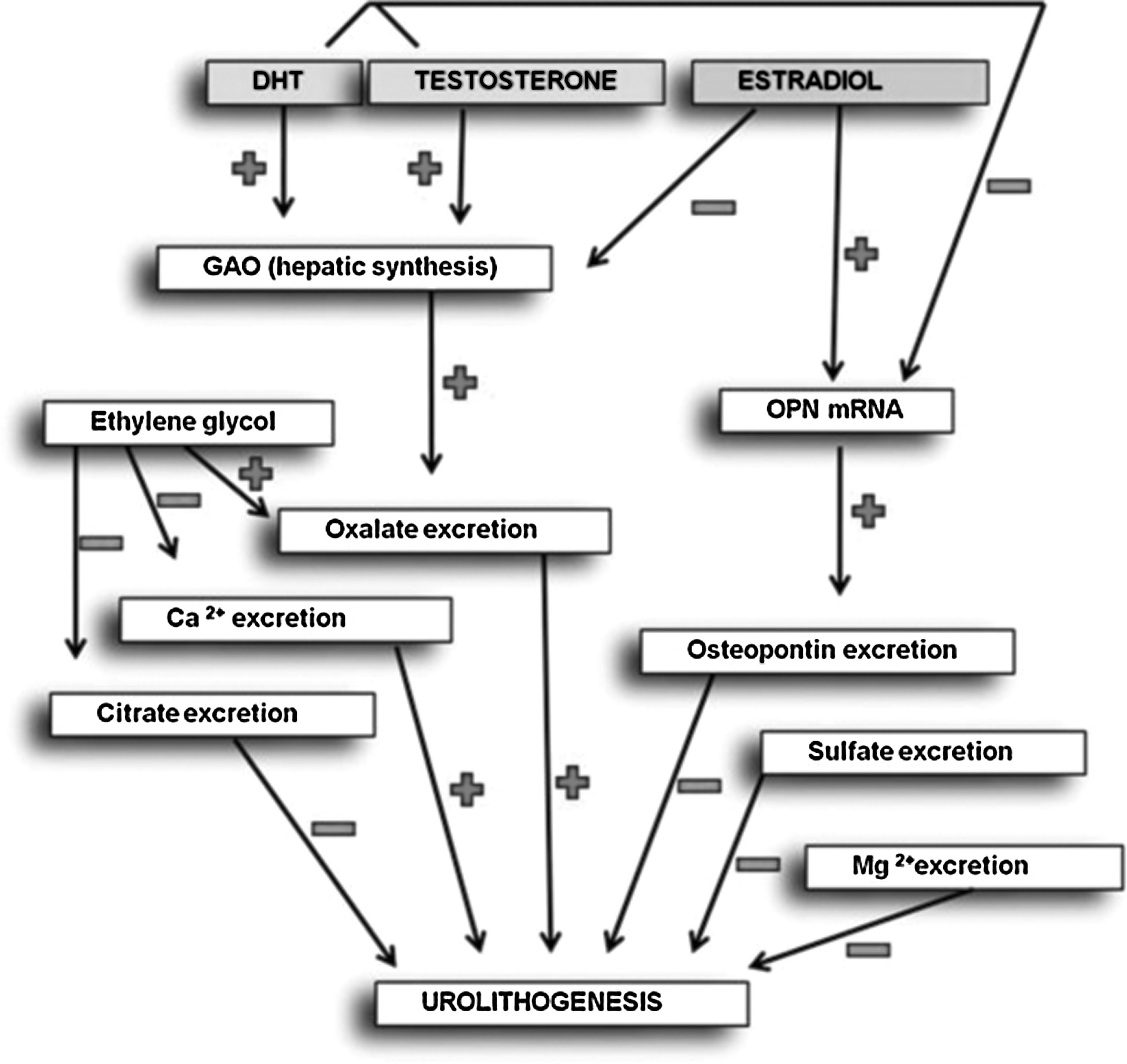
Proposed influence of sex hormones on urolithogenesis. DHT = dihydrotestosterone; GAO = glycolic acid oxidase; OPN = osteopontin.
Another mechanism by which sex hormones affect the rate of stone formation is via their effects on expression of osteopontin (OPN). OPN, a 44 kD renally secreted acidic phosphorylated glycoprotein, 26,27 has been shown to be a macromolecular in vivo inhibitor of calcium oxalate crystallization. 28 OPN synthesis has also been shown to be upregulated in experimental urolithiasis models induced by ethylene glycol supplemented diets in rats. 29 More evidence that OPN is involved in urolithogenesis is the link between an OPN genetic polymorphism and formation of urinary calcium stones reported by Gao and coworkers. 30 Importantly, Yagisawa and associates 31 used a rat model to demonstrate that OPN expression in the kidney is suppressed in the presence of testosterone and promoted by the presence of estrogen. This contributes further to the evidence that hormones are involved in urolithogenesis.
There is a paucity of research into the relationship between sex hormones and urolithogenesis in humans, with only two publications noted on review of the literature. In the first study, Van Aswegen and colleagues 32 examined human testosterone levels and their relationship to stone formation by investigating total urinary testosterone and renal calculi in 16 healthy participants. The authors demonstrated that urinary testosterone levels were lower in patients who had a history of kidney stones. Because of the proposed endocrine (eg, via GAO) mechanism of sex hormone influence on lithogenesis, however, examination of urine testosterone levels is less than ideal to investigate the role that serum testosterone levels play in the physiology of stone formation.
In the second of these studies, Tiselius and colleagues 33 demonstrated, in a series of castrated men with prostate cancer, that there was no significant change in urinary oxalate excretion despite a decrease in plasma testosterone. However, the mean age was 71 years, thus introducing grounds for questioning the magnitude of the effect, given our lack of knowledge of the in vivo enzyme kinetics of GAO. There was also little attention paid to standardizing or quantifying oxalate intake. Our study seeks to answer the question of whether stone-forming men have higher testosterone levels than nonstone-forming controls.
Currently, interventions for stone prevention consist primarily of increased water intake, diet alterations, urine alkalinizing agents, thiazides, and allopurinol. 34,35 If testosterone contributes to stone formation, however, perhaps testosterone may also be targeted to enhance stone prevention. In particular, 5-α reductase inhibitors may provide a way to effectively target dihydrotestosterone (DHT) levels to provide stone prophylaxis. In fact, the use of finasteride to decrease urinary oxalate excretion has already been described in male rats. 36 This implies that DHT and testosterone may both play a role in the pathway of stone formation.
Our analyses showed that after controlling for age and BMI, total serum testosterone levels were higher in the group with a history of urolithiasis. This is consistent with our hypothesis that testosterone may play a pivotal role in urolithogenesis in men. Free testosterone levels, however, did not statistically differ between the two groups. The free testosterone level was directly measured, but there is debate over the most reliable method of assay. Furthermore, there is no experimental evidence to suggest that free testosterone concentration is specifically relevant to urolithogenesis. Therefore, it is difficult to draw conclusions regarding the lack of difference in free testosterone concentrations between our patient populations.
Several limitations of this study should be noted. The small sample size and lack of age-matched populations of cases and controls has not prevented us from drawing statistically valid conclusions but may limit the ability to detect other differences, such as differences in free testosterone or impact of family history of urolithiasis. Also, the use of single sample-based serum assays prevented us from taking into consideration diurnal as well as day-to-day variation in testosterone levels. In addition, there is a lack of consensus on what magnitude of difference in testosterone levels is sufficient to imply clinical significance.
Previous animal research has reported a direct correlation between serum testosterone concentrations and urinary oxalate excretion. 32,36 Therefore, another limitation of this study is the absence of 24-hour urine studies. Finally, our participants were predominantly non-Hispanic Caucasian (42/55, 76.4%), and thus our results cannot be extrapolated to other ethnic groups. This is important because of known ethnic variation in the rate of stone formation, such as described lower rates of stone formation in the African American population. 37
We believe that our findings indicate a need for further study, possibly prospectively following a large cohort of patients on whom testosterone levels are recorded and reporting the incidence of stone formation.
Conclusions
In this small pilot study, a higher total serum testosterone level was found in stone-forming men than in nonstone-forming controls. This finding is consistent with several animal models that have demonstrated that testosterone is a risk factor for stone formation. This should be studied in a prospective fashion on a larger scale to further elucidate the association between serum testosterone levels and urolithiasis in humans. A significant association may have relevant therapeutic implications.
Footnotes
Acknowledgment
The work on this publication was supported in part by the funds from the Atlanta Clinical & Translational Science Institute.
Disclosure Statement
No competing financial interests exist.