
Abstract
Laparoscopic partial nephrectomy (LPN) is becoming the standard of care for incidentally diagnosed, small renal tumors. With its seven degrees of freedom and three-dimensional vision, the DaVinci robotic surgical system has been used to assist in LPNs. The main disadvantage of robot-assisted surgery, however, is the lack of tactile feedback. We present a case of renal artery injury during robot-assisted renal surgery. Robot-assisted partial nephrectomy (RPN) was planned for 47-year-old man with a 3.5-cm right renal mass. After standard bowel mobilization, renal hilar dissection was performed. In the attempt to complete the dissection posteriorly, however, there was sudden profuse bleeding. The intraperitoneal pressure immediately increased to 20 mm Hg, and an additional suction device was inserted through the 5-mm liver retractor port. On inspection, there was an injury at the takeoff of the posterior segmental artery. A decision was made to convert to robot-assisted laparoscopic radical nephrectomy. The main renal artery and renal vein were controlled with Hem-o-Lok clips. The estimated blood loss was 2,000 mL. Four units of packed red blood cells were transfused intraoperatively. The post-transfusion hemoglobin level was 12.6 g/dL. There were no other perioperative complications. The surgeon should keep in mind that the robotic arms are very powerful and can easily injure major vessels because of lack of tactile feedback. A competent and experienced tableside surgeon is very important in robot-assisted surgery because the unsterile console surgeon cannot immediately react to intraoperative complications.
Introduction
Recently, The da Vinci robotic surgical system (Intuitive Surgical, Sunnyvale, CA) has been used to perform partial nephrectomies with its benefit of reduced difficulty in intracorporeal suturing compared with standard laparoscopy. Purported advantages include three-dimensional stereoscopic optics, elimination of tremor, seven degrees of freedom of motion, and improved surgeon ergonomics. The robotic system, however, has a disadvantage of lack of tactile feedback, and it is difficult for the console surgeon to react directly to intraoperative complications that may necessitate conversion to open procedures. We present a case of renal artery injury during robot-assisted renal surgery.
Case Report
Patient
A 47-year-old man was referred for a right renal mass, which had been diagnosed incidentally at the health promotion center. He was classified as American Society of Anesthesiologists class I with well-controlled hypertension and had a remote surgical history of aherniated lumbar disc. Preoperative imaging studies revealed 3.5-cm, right enhanced mass at the posterior aspect of the lower pole, which was confined to the renal parenchyma. There was no thrombus of renal vein and lymphadenopathy (Fig. 1). The patient consented to robot-assisted partial nephrectomy (RPN) and possible complications. He underwent bowel preparation the day before surgery.
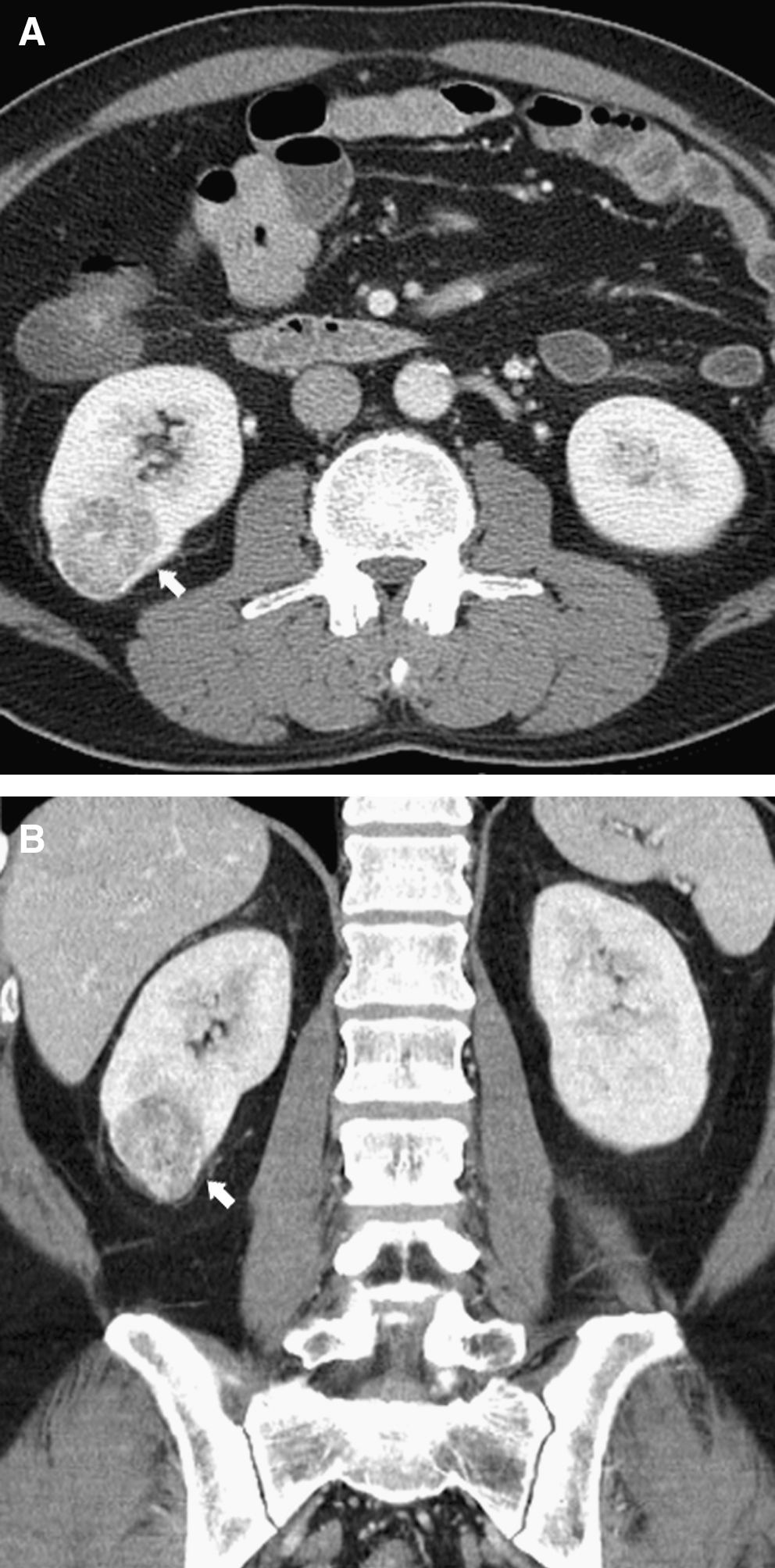
Preoperative enhanced computed tomography (CT) of the abdomen showing a 3.5 cm enhanced mass (white arrow): (
Operation and injury of renal artery
General endotracheal anesthesia was performed, and a Foley catheter was inserted before positioning. The patient was placed in the semilateral position. All dependent points were padded, and the patient was strapped to the operating table with cloth tape. Pneumoperitoneum was established by using a Veress needle just above the umbilicus up to a maximum pressure of 15 mmHg. A 12-mm port for the robotic camera was placed. Two 8-mm robotic instrument ports were placed under vision at an 8-cm distance on each side of the camera. These three ports were triangulated toward the renal hilum. A 12-mm assistant port was placed at 8 cm from the umbilicus toward the symphysis pubis. A 5-mm subxiphoid port was placed for liver traction (Fig. 2).
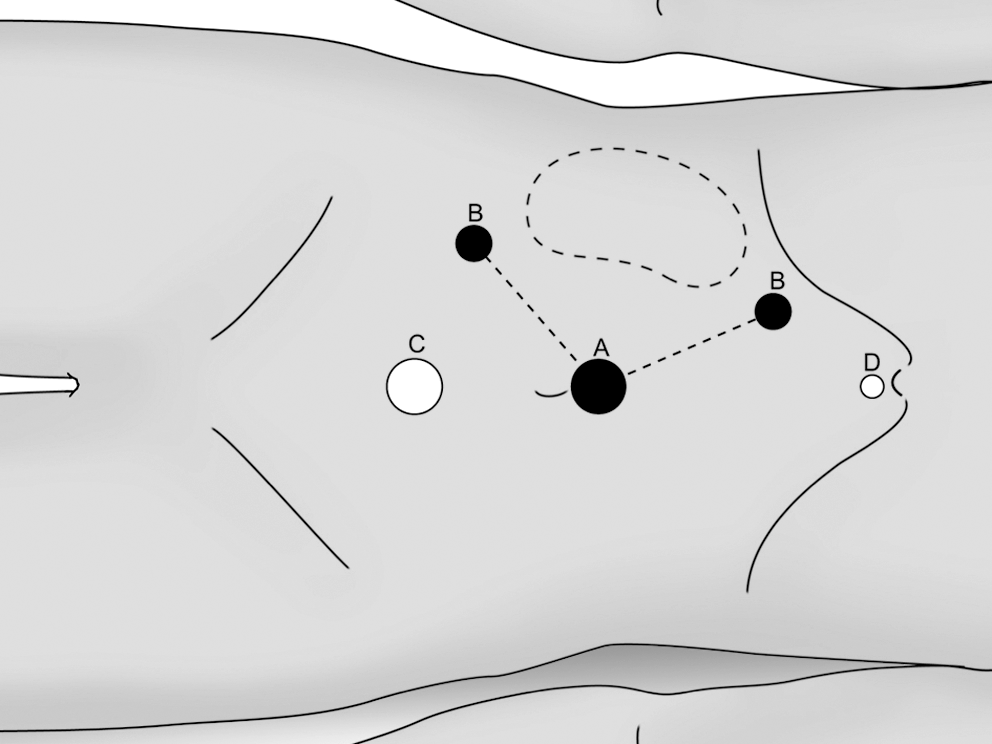
Illustration of port placement: (
The robot was docked posteriorly with a 20-degree oblique position toward the head of the patient. Using a 30-degree degree lens, the paracolic gutter was incised along the line of Toldt. The hot shears monopolar curved scissors on the right robotic arm and Maryland bipolar forceps on the left robotic arm were controlled by the console surgeon during dissection.
After standard medial mobilization of the ascending colon, the ureter and gonadal vein were identified. The ureter was retracted superiorly to expose the underlying psoas muscle. Dissection was directed toward the renal hilum. The renal artery and vein were visualized. While attempting to complete the dissection posteriorly, however, there was sudden profuse bleeding. The intraperitoneal pressure was immediately increased to 20 mm Hg, and an additional suction device was inserted through the 5-mm liver retractor port.
On inspection, an injury was noted at the takeoff of the posterior segmental artery (Fig. 3). A decision was made to convert to robot-assisted laparoscopic radical nephrectomy. The main renal artery was controlled with Hem-o-Lok clips. The renal vein was controlled in the same manner. The rest of the kidney was mobilized by sharp and blunt dissection of perirenal soft tissue and division of the ureter. The fully freed specimen was placed in an extraction bag that had been inserted through the 12-mm assistant port. A closed drain was placed through a port site. The robot was then undocked from the patient. The camera port site incision was extended, and the specimen was delivered. Standard port site closure was performed.
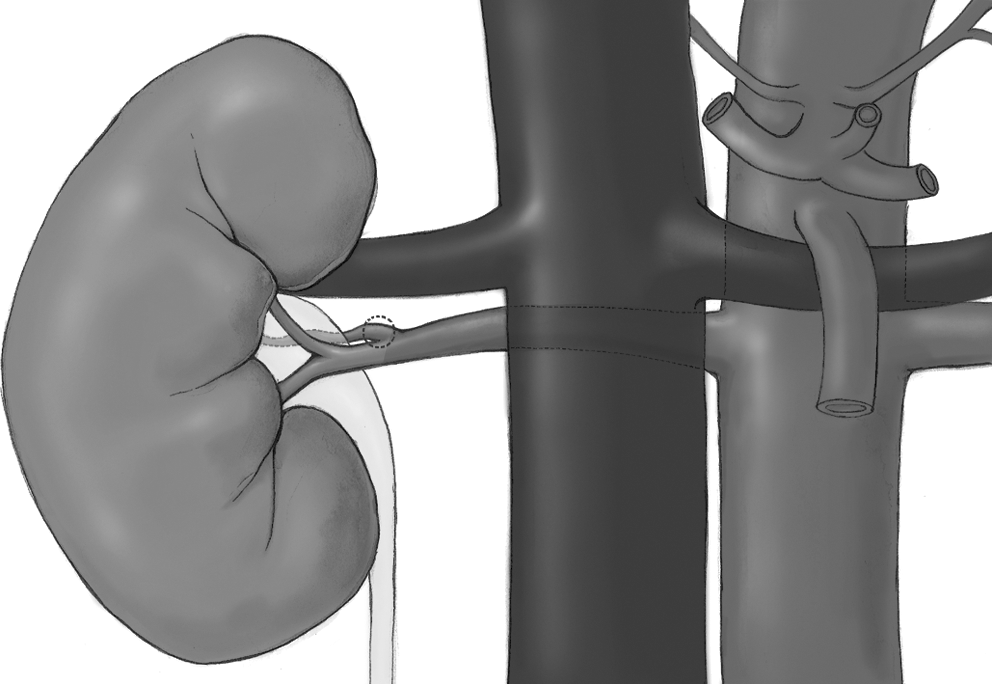
Illustration of renal pedicle; circle in dashed line indicates the injured site of posterior segmental branch of the right renal artery.
Results
The operative time, including robot setup (15 minutes), was 260 minutes. The console time was 195 minutes. It took 7.5 minutes from the onset of injury to the control of the renal artery. The estimated blood loss was 2,000 mL. Four units of packed red blood cells were transfused intraoperatively. Preoperative and posttransfusion hemoglobin (hematocrit) level was 14.5 g/dL (44.2 %) and 12.6 g/dL (38.0 %). Regular diet and ambulation were resumed by postoperative day 1, and the patient was discharged home on postoperative day 4. There were no other perioperative complications.
The final pathology report revealed a clear-cell, renal-cell carcinoma (Fuhrman nuclear grade 2, T1aN0Mx by American Joint Committee on Cancer). The follow-up period was 9 months. There were no remarkable findings in chest radiography and abdominal CT scans taken during the follow-up period.
Discussion
Partial nephrectomy has become an acceptable therapeutic approach in patients with small renal-cell carcinoma, especially a T1a stage tumor. LPN has resulted in the benefit of improved postoperative convalescence while following the principles of open oncologic surgery. Ultrasonographic guidance allows accurate localization and subsequent marking of the tumor. The tumor is then removed under direct vision with intraoperative assessment of the tumor bed. Difficulty in intracorporeal suturing and concerns regarding warm renal ischemia, however, have limited its widespread application.
Recently, robot-assisted surgery has become a promising new technique in fields of urologic surgery, especially in patients with prostate cancer. In parallel with the superior data from robot-assisted radical prostatectomy, several studies have compared RPN with LPN and demonstrated that outcomes with RPN are comparable with those with LPN, with several variables improved over LPN. 3 –6 A multi-institutional analysis of more than 100 patients, showed the benefits of RPN over LPN. Comparison of perioperative outcomes revealed shorter operative time (140 vs 156 minutes), shorter warm ischemic time (19 vs 25 minutes), and shorter duration of hospital stay (2.5 vs 2.9 days). 7
Complications, including intraoperative hemorrhage during RPN, however, can occur in LPN. During LPN, the rate of intraoperative hemorrhage has been reported to be 2% to 3.5%. 2,8 There have been few reports regarding serious intraoperative bleeding during robot-assisted partial nephrectomy. Bleeding during RPN can have a number of causes. Bleeding can occur during dissection of the hilum or ureteral/gonadal vessels or during tumor resection even with a clamped renal pedicle. Most serious bleeding among these can occur from injury to major vessels, especially the renal artery.
Complete and thorough dissection of the renal hilum is very important before attempting vascular control. While attempting to complete the dissection posteriorly in our patient, we encountered profuse bleeding. This highlights the value of gentle handling of the tissues. The lack of tactile feedback in the robotic system might have contributed to this complication.
After the injury, we considered conversion to open surgery. Scrubbing time for the console surgeon, however, had to be considered also. Instead of conversion, we continued our robot-assisted operation for bleeding control. Intraperitoneal pressure was increased to 20 mm Hg immediately. Insertion of an additional suction provided us with a better operative field and helped us tremendously in locating the site of injury. It took 7.5 minutes from the onset of injury to the control of the bleeding vessel, and these 7.5 minutes would not have been much different from time needed for the arrival of the console surgeon after scrubbing for conversion to open procedure. We have to admit, however, that continuation of the robot-assisted operation might have been reckless, considering the blood loss of 2,000 mL in less than 8 minutes.
Performing a vascular operation with a bulldog clamp applied to the main renal artery and completing nephron-sparing surgery could have been one solution to this event. We chose conversion to robot-assisted radical nephrectomy, however, because of concerns regarding prolonging the warm ischemia time and the technical difficulty in repairing the renal artery injury.
During open or LPN, the surgeon is able to react directly to unexpected complications. During RPN, however, it is technically difficult for the unsterile console surgeon to immediately address intraoperative complications at the operating table. If heavy bleeding occurs during LPN, immediate conversion to an open procedure can be achieved. Unlike LPN, the procedure cannot be converted to an open procedure immediately during RPN, because the robotic system has to be undocked first. This delay can lead to a life-threatening situation. A competent and experienced tableside surgeon is very important. He or she has to have a solid knowledge of the anatomy, be familiar with the steps of the operative procedure, and must know how to troubleshoot the robotic system when problems arise. He must also be prepared to perform open surgery if conversion is warranted, because the console surgeon will need some time to scrub before proceeding in the operation.
Conclusions
RPN can facilitate the technical challenges of LPN because of purported advantages. Complications during RPN, however, can occur as well. The surgeon should keep in mind that the robotic arms are very powerful and can injure major vessels easily because of lack of tactile feedback. The importance of good surgical technique cannot be overemphasized. A competent and experienced tableside surgeon is likewise essential in RPN.
Footnotes
Disclosure Statement
No competing financial interests exist.