
Abstract
Objective:
Short right renal vessels might complicate kidney transplantation, thus causing traction and difficulties during anastomosis. Single-center prospective comparison of right- and left-sided transperitoneal hand-assisted laparoscopic donor nephrectomy (HALDN) is presented.
Patients and Methods:
Eighty-two living kidney donors underwent HALDN between 2003 and 2008. Right-sided HALDN was performed in 46 living kidney donors. The operative technique of right-sided HALDN was modified to obtain the maximum length of right renal vessels. Outcome data in donors including quality of life as well as graft outcome in recipients were prospectively collected.
Results:
All procedures were laparoscopically completed with no conversion. Mean operative time was 127 minutes (vs. 138 minutes in left HALDN, p = 0.08). The mean warm ischemia time was 41 seconds (vs. 39 seconds in left HALDN, p = 0.23). There was no renal artery or vein thrombosis in any of the grafts. Mean blood loss was 81 mL (vs. 92 mL in left HALDN, p = 0.09). Hospital discharge was on an average of 3.6 days postoperative. Delayed graft function occurred in two recipients: one in the left group and the other in the right group. One-year graft survival rate was 95% in the left group versus 96.9% in the right group (p = 0.08). Further, no statistically significant difference in serum levels of creatinine was seen between the groups 1 year after the transplantation.
Conclusions:
Right HALDN is technically safe and feasible and results in convenient extension of right renal vessels to full length with no increased incidence of vascular thrombosis.
Introduction
The method of live kidney donation has experienced a further development along with the introduction of laparoscopic surgical techniques. The reason for this is the superior benefits of the minimally invasive nature of laparoscopic techniques. 2 Hand-assisted laparoscopic donor nephrectomy (HALDN) was introduced in 1998. 3 The use of hand-assisted approach permits the surgical team to use the necessary extraction incision to their advantage throughout the procedure. Potential advantages of HALDN include short operative time, a shorter learning curve related to the presence of robust tactile feedback, the ability to manually assist in dissection, prevention of torsion of the kidney after the lateral attachments have been dissected, and ease of obtaining hemostasis by manual compression of bleeding vessels. 4
However, as in open donor nephrectomy (ODN), the left kidney has remained the preferred organ for laparoscopic donor nephrectomy (LDN) due to the greater renal vessel lengths. 5 Most transplant surgeons are reluctant toward right-sided LDN fearing short vessels and renal vein thrombosis. On the other hand, some surgeons might prefer the right kidney, because it is easier to recover than the left kidney; and the risk of spleen laceration is decreased. 6 Anatomically, the right renal vein is considerably shorter than the left renal vein and the right renal artery lays partly retrocaval. Several techniques have been used to overcome the technical challenge associated with short right renal vein, such as renal vein extension using an autologous saphenous graft or polytetrafluoroethylene vascular prostheses. 7 Herein, we report our experience with right-sided HALDN with hand-assisted extension of renal vessels, which allowed the exposure of the right aortorenal junction and provided maximal length of the right renal vessels.
Patients and Methods
From December 2003 to December 2008, a total of 82 hand-assisted living donor nephrectomies have been performed at our institution. Of these, 46 living donors underwent right-sided HALDN. The institutional selection criteria for the right versus left kidney were to leave the largest and highest functioning organ with the donor and to provide the recipient surgeon with an organ with as few vessels as possible regardless of laterality. Pre-, intra-, and postoperative data were prospectively collected from all consecutive donors and recipients.
Preoperative management
Our preoperative donor work-up is standardized. Briefly, potential donors are thoroughly screened by medical history, physical examination, and an array of tests (hematology, coagulation, blood chemistry, and urine analysis), kidney and chest imaging, infectious disease including viral studies, immunologic studies to determine donor–recipient match, and electrocardiography (EKG). All donors were required to undergo an evaluation by a clinical psychologist.
Surgical technique
For right HALDN, the donor is placed in the right flank position, supported by adequate padding. The abdominal cavity is explored using a five-port transperitoneal approach (an 11-mm umbilical port for the laparoscope, one 5-mm port for liver retraction, and two 5-mm and one 10-mm trocars as working ports). After creation of the pneumoperitoneum by insertion of a Veress needle through an incision above the umbilicus, a 10-mm trocar is placed for camera insertion. Thereafter, four additional working trocars were introduced. The insufflation pressure was maximally 12 mm Hg. After superior retraction of the liver, the peritoneum was laterocolically opened, and the colon was medially mobilized. This maneuver was followed by inspection and subsequent depiction of the psoas muscle and the ureter. Preparation followed along the ureter and the adnexal vessels to the renal hilum, where the vessels were identified. After complete exposure of the kidney and vessels with ligation of the side branches of the renal vein, the vena cava and the abdominal aorta were isolated. The kidney is dissected until it is only fixed by the hilar vessels. At this stage, a full mobilization of the right renal pedicle and inferior vena cava (IVC) was possible. The right renal vein was dissected down to its root from the IVC, and the renal artery was mobilized just to the lateral border of IVC, to obtain sufficient length for anastomosis. Thereafter, the left hand of the surgeon was intraabdominally placed via a right lower quadrant vertical incision (Fig. 1). For this purpose, a hand port (Omniport®; Advanced Surgical Concepts Ltd.) was used in the first 16 patients. In the remaining 66 patients, the surgeon's hand was directly placed through the incision without using the hand port. The vessels were further prepared under digital control until the anterior surface of the IVC was exposed and the full length of the right renal vein was demonstrated. Thereafter, using the index und middle fingers, the IVC was mobilized and pushed aside (Fig. 2). This exposure allowed identification and dissection of the right renal artery down to the origin of the aorta. The residual nervous and connective tissue between the renal artery and the renal vein were then carefully dissected, allowing now a full exposure of the renal artery at the level of the aortorenal junction. After intravenous administration of heparin, the ureter was then cut between two clips at the transition to the pelvis minor. The renal vein was accordingly held between two fingers and closed by a triple-row Endo-TA stapler (Multifire Endo TA® 30; Covidien). Thereafter, the renal artery was closed and cut by a triple-row Endo-TA stapler (Fig. 3). This simple maneuver resulted in harvesting the entire right renal artery length in all cases, making a safe and simple anastomosis possible. We used this technique also for the left-sided HALDN. Immediately after extirpation of the kidney, perfusion with HTK (Custodiol®; Koehler) solution was carried out. The recipient was simultaneously prepared in the neighboring operating theatre. This resulted in a reduction of the cold ischemia time to <30 minutes.
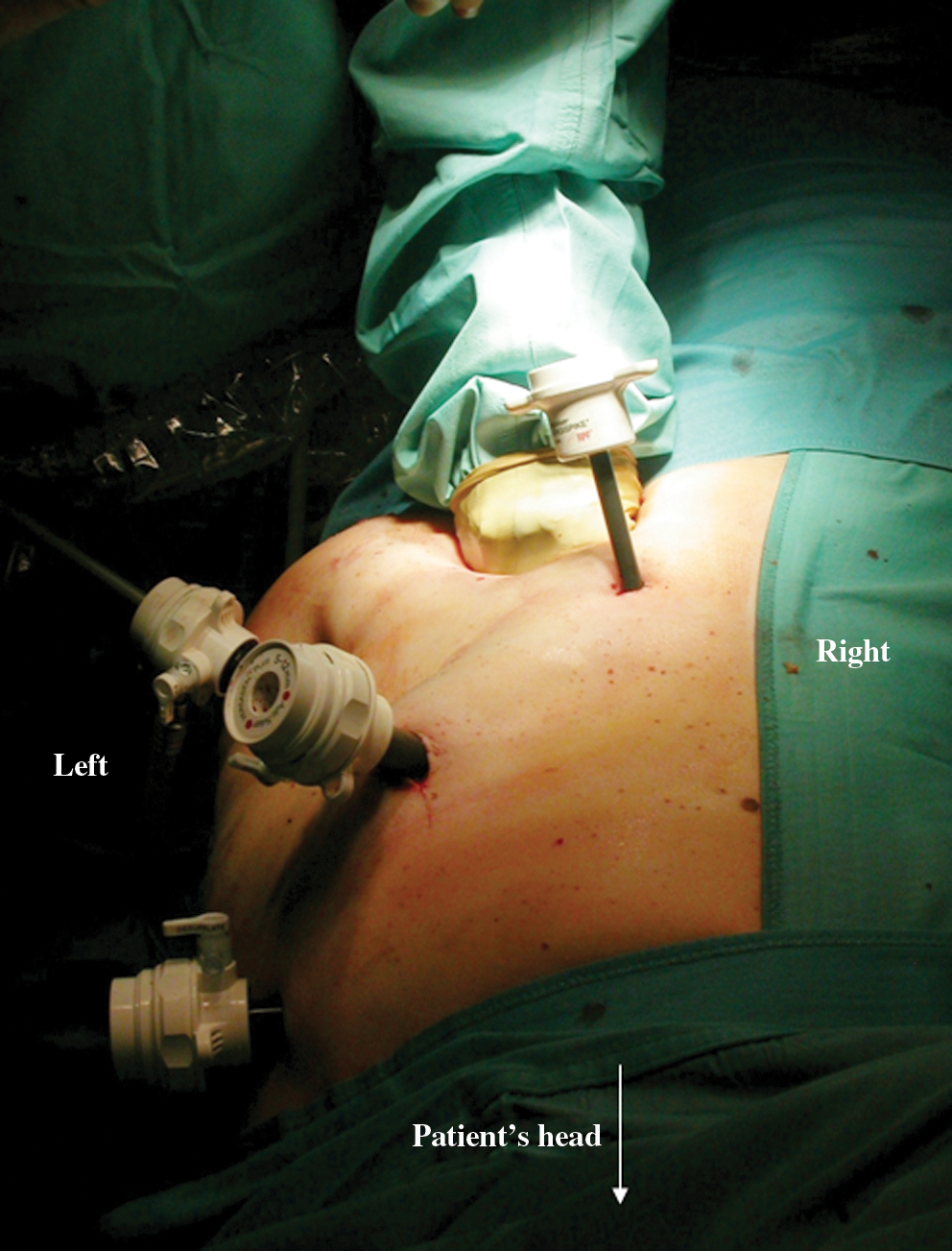
Introduction of surgeon's left hand into the abdominal cavity through a right lower quadrant vertical incision for hand assistance.

The vessels were prepared under digital control until the anterior surface of the inferior vena cava was exposed and the full length of the right renal vein was demonstrated.
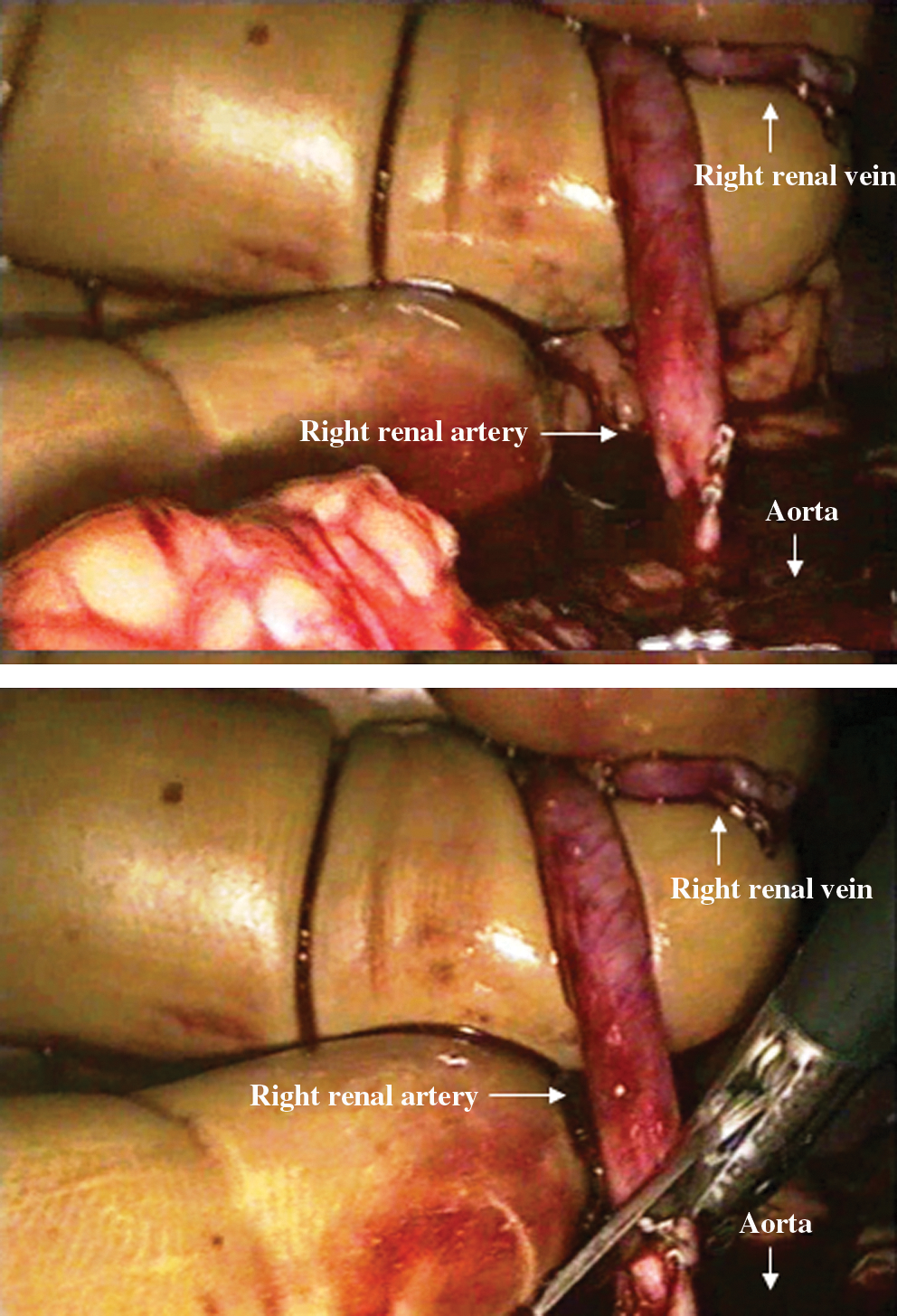
The exposure allowed identification and dissection of right renal artery down to the origin of the aorta.
Recipients
Renal transplantation was carried out using the standard technique of preperitoneal placement in the iliac fossa. The immunosuppression protocol was standardized in all recipients consisting of a triple combination (tacrolimus, methylprednisolone, and mycofenolate-mofetil). Patients with a particular immunological risk received an additional therapy with anti-thymocyte globulin or IL-2R inhibitor basiliximab as induction therapy. During the first year postoperatively, we recorded survival rates of recipients and grafts, acute rejection rates, venous thrombosis, and ureteral complications as defined as the need for a percutaneous nephrostomy, ureter reconstructions, and renal function. First episodes of acute rejection were treated with pulse doses of methyl-prednisolone; and second episodes were treated with thymoglobulin. Delayed graft function was defined as the need for dialysis within the first postoperative week.
Statistical analysis
Statistical analyses were performed with SPSS 12.0 (SPSS, Inc.). Student's t-test and chi-square test were used for statistical comparisons. The rate of 1-year graft survival was calculated by Kaplan–Meier analysis. The level of significance was set at p < 0.05.
Results
Characteristics, surgical outcomes, and postoperative outcomes of donors and recipients are shown in Tables 1 and 2.
HALDN = hand-assisted laparoscopic donor nephrectomy; NS = not significant; SD = standard deviation; NA = not available.
POD = postoperative day; GFR = glomerular filtration rate.
Clinical results—donors
The procedures were all carried out as planned without conversion to ODN. In all cases, the vascular anastomoses were easily performed, and no vascular thrombosis occurred. The clinical results of 46 donors from right-sided HALDN using the modified technique were compared with results of 36 donors with left-sided HALDN. Mean operative time was 127 minutes (range, 98–184 minutes) in right HALDN group and 138 minutes (range, 109–191 minutes) in left HALDN group (p = 0.08). The warm ischemia time was not significantly different between the right HALDN (41 seconds; range, 25–110 seconds) and for procurement of the left kidney (39 seconds; range, 21–103 seconds; p = 0.32). Also, the average estimated blood loss for the right HALDN (81 mL; range, 42–280 mL) was not significantly different from that for the left HALDN (92 mL; range, 48–420 mL; p = 0.09). Blood transfusion was not required for any patient who donated a right kidney. One patient required transfusion 2 days after donating the left kidney. The mean time to discharge from hospital was equal for the patients in both groups (right HALDN; 3.6 days vs. 3.7 days; p = 0.52). Intraoperative complications occurred in two patients during left-sided laparoscopic hand-assisted nephrectomy, which were bleeding in one case (total blood loss 420 mL) and a small capsular tear of the spleen. The lesions were immediately recognized and treated without conversion. Re-interventions were not indicated. No major postoperative complications occurred in either group. No kidney graft was lost for technical reasons.
Quality of life was measured in all donors using the SF-36 questionnaire. Overall, our donors reported a better quality of life than the general German population in all domains (Fig. 4).
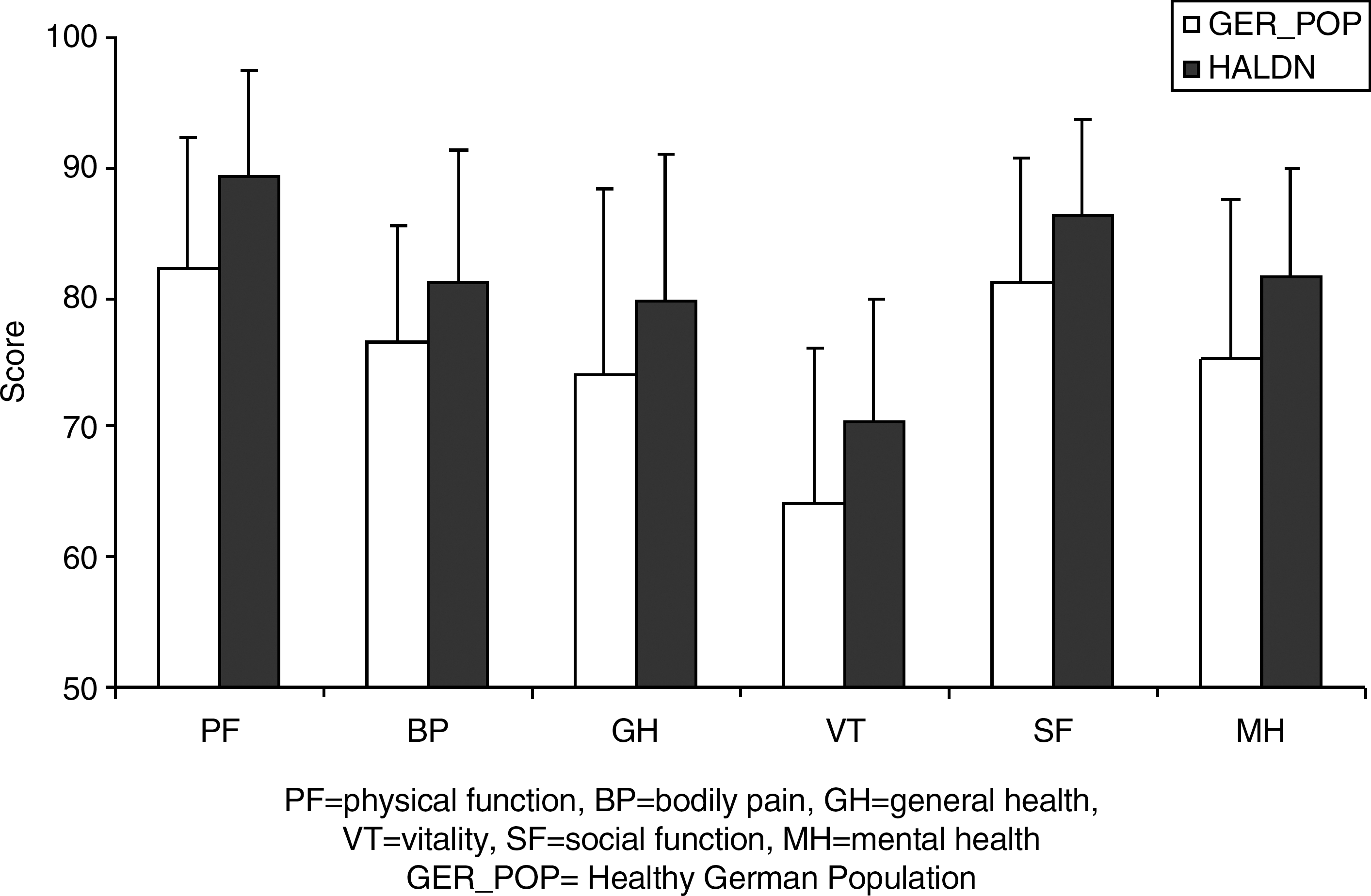
Mean quality of life scores (SF-36 questionnaire) for all donors after hand-assisted laparoscopic donor nephrectomy (HALDN) procedure (right and left, n = 82) and for the German population.
Clinical results—recipients
We prospectively collected the data of recipients of 46 right-sided hand-assisted laparoscopic harvested kidneys and compared these with data of recipients of 36 left-sided procured kidneys (Table 2). A total of 58 kidneys were transplanted to the right iliac fossa and twenty-four into the left fossa. When comparing the rate of early function, no significant difference was observed between the recipients of both groups (Table 2). Delayed graft function occurred in two patients: one in the left group and the other in the right group. One-year graft survival rate was 95% in the left group versus 96.9% in the right group (p = 0.08). Further, both parameters of the glomerular filtration rate for the characterization of renal function, creatinine, and cystatin C showed no statistically significant difference between the groups 1 year after transplantation (Table 2).
Discussion
Despite initial concerns about the safety of laparoscopic living donor nephrectomy, this technique has proved to be safe and reproducible in many studies. 8 Recently, there has been increasing interest in LDN for harvesting kidneys for donation, especially in high-volume renal transplant centers. This has been due to the advantages reported for LDN, with an equivalent graft outcome to ODN. 9 We have previously reported our earlier results comparing outcomes and complications in open and HALDN, where safety, graft function, and complications were similar in the two groups. 10 However, recovery and the return to normal activity were more rapid for donors who underwent laparoscopic hand-assisted surgery. One of the disadvantages considered for LDN versus ODN is the limited use of the right kidney, even where harvesting the right kidney would be preferable. Thus, when reviewing the cumulative experience of LDN, it is clear that the left kidney is preferred due to the longer renal vein. 5 However, drawbacks of the left-sided HALDN are higher chance of lacerating the spleen during laparoscopic mobilization of the splenic flexure of the colon and handling of the lumbar and supra-adrenal side branches of the left renal vein. 11 In the meantime, some data on the advantages of right-sided LDN have become available. For instance, Dols et al 12 demonstrated that right-sided LDN is associated with a significantly shorter operating time of a median of 30 minutes compared with left-sided LDN. Same kind of data were reported by Lind et al, 6 whereas Husted et al 13 revealed no difference in operating time between both groups.
However, major drawbacks for using the right kidney are the shorter length of the renal vein and the retrocaval position of the renal artery. In addition, transection of the renal vessels with laparoscopic vascular staplers might lead to additional loss of available length necessary for implantation. Short vessels can consume more time and extend the length of the warm ischemia during renal vessel anastomoses. In the last few years, several techniques have been reported for right-sided LDN to overcome the problem of short renal vessels. 14 Mandal et al 15 reported three venous thromboses in eight right renal allografts harvested by right-sided LDN. Since they found these results unacceptable, they used several modifications both for right donor nephrectomy and in recipients. After these changes in technique, they reported no vascular complication in their next nine recipients. Buell et al 16 reported a large series of right-sided LDN, with 4% renal vein thrombosis (3 of 85) in the pure laparoscopic group but no vascular complications in a hand-assisted group (40 patients). They found that hand-assisted devices can provide better exposure and result in faster surgery, with an acceptable outcome when compared with the pure laparoscopic approach. Further, Lind et al 6 reported their experience of pure right-sided LDN in 73 patients, with recipient iliac vein mobilization to overcome the difficulty in anastomosing the right renal vein. Bollens et al 17 described a new technique to maximize the length of right renal vein using a modified Endo-GIA stapler. Kay et al 18 reported 66 left and 18 right donor nephrectomies that were performed by laparoscopic techniques. In right donors, the IVC was controlled through an open incision to introduce a Satinsky clamp in six patients. In the last 12 patients, Kay et al used a stapler to divide the renal vein. Several techniques have been described to elongate the right renal vein by forming a collar or using patient veins or an artificial material. 18 Turk et al 19 reported laparoscopic right donor nephrectomy using a laparoscopic Satinsky clamp that was inserted through a separate incision in the abdominal wall and applied to the IVC, and the renal vein with a cuff of IVC was excised.
However, in view of difficulties associated with the right renal vein, less attention has been given to the shortened length of the right renal artery obtained during right LDN. 20,21 The aim of this work was to describe a novel and simple maneuver during right-sided HALDN as a feasible and safe technique to gain the maximum available length of the right renal artery. The basic idea behind this technique is that during HALDN, the digital palpation offers a valuable tool giving the surgeon a tactile sensation to manually trace the vascular structures, especially the aorta and the renal artery. The technique described in this study provides exposure of the right aortorenal junction during HALDN using the index und middle fingers to mobilize the IVC and push it aside. This exposure allows identification and dissection of right renal artery down to the origin of the aorta, thereby providing maximal length of the right renal artery. In addition, this approach also enables the surgeon to have safe control of the IVC during excision of the right renal vein. This technique had proved to be safe and reproducible. We did not detect any significant differences in donor hospital stay, donor intra- and postoperative complication rate, or renal graft survival between left- or right-sided hand-assisted donor nephrectomy. No grafts were lost due to technical reasons. There were no conversions and no major complications in our study. However, regardless of the difficulty due to a short right renal vein and the difficulty in performing the graft implantation, the evaluation process for the kidney extraction must follow the principle where the best kidney should always remain with the donor.
In conclusion, the modified technique presented in this article is a feasible way to overcome technical problems associated with short right renal vessels in right-sided HALDN that may jeopardize the results of living renal transplantation. This simple modification provides an additional option for laparoscopic right donor nephrectomy and might motivate more laparoscopic surgeons to perform right HALDN. However, our study is limited to the experience of a single surgeon; thus, more studies are needed to confirm the safety and reproducibility of this technique. This technique should, therefore, be performed by experienced laparoscopic surgeons.
Footnotes
Disclosure Statement
No competing financial interests exist.