
Abstract
Introduction:
Management of ureteroenteric strictures presents a significant challenge because of its intraabdominal location and morbidity associated with open surgical management. The peripheral cutting balloon microsurgical dilatation device (PCBD), approved by The United States Food and Drug Administration (USFDA) for use in coronary angioplasty, features a 2-cm noncompliant balloon with four microsurgical blades mounted longitudinally on its outer surface. We evaluated the feasibility and outcome of this cutting balloon dilator in the treatment of ureteroenteric anastomotic strictures.
Materials and Methods:
Three patients with a 1-cm or less ureteroenteric stricture underwent a transluminal incision under fluoroscopic guidance. Percutaneous access was obtained and a guidewire was introduced into the renal pelvis and ureter in antegrade fashion and passed through the stricture. The exact length of the strictured segment was measured. The PCBD was deployed over the guidewire and the balloon was inflated at the stricture site. The maximum diameter of the inflated balloon was 8 mm. Approximately 30 seconds later, the balloon was deflated and the enlarged passage from the ureter to the ileal loop was verified under fluoroscopy. A ureteral stent was placed and removed at 6 weeks after the procedure.
Results:
Postoperative computed tomography scans at 12 months revealed improved hydronephrosis. All patients were asymptomatic postoperatively. One patient had a solitary kidney and creatinine level decreased significantly following the procedure.
Conclusion:
Dilatation and incision with PCBD is a novel approach for the treatment of the short ureteroenteric anastomotic strictures. Long-term data need to be obtained to establish the efficacy of this technique.
Introduction
Recently, a new system for balloon angioplasty was introduced. The peripheral cutting balloon microsurgical dilatation device (PCBD) combines the features of conventional balloon angioplasty with advanced microsurgical capabilities (Boston Scientific, Natick, MA). This device was originally designed for treating in-stent coronary artery stenosis and has been expanded to additionally treat fibrotic vascular stenosis including vein bypasses and dialysis–fistulae–stenosis with potential to better dilate ischemic and fibrotic lesions resistant to conventional percutaneous transluminal angioplasty. 12,13 In this study, we describe a novel technique of treating ureteroenteric strictures with the PCBD and our results with 1-year follow-up.
Materials and Methods
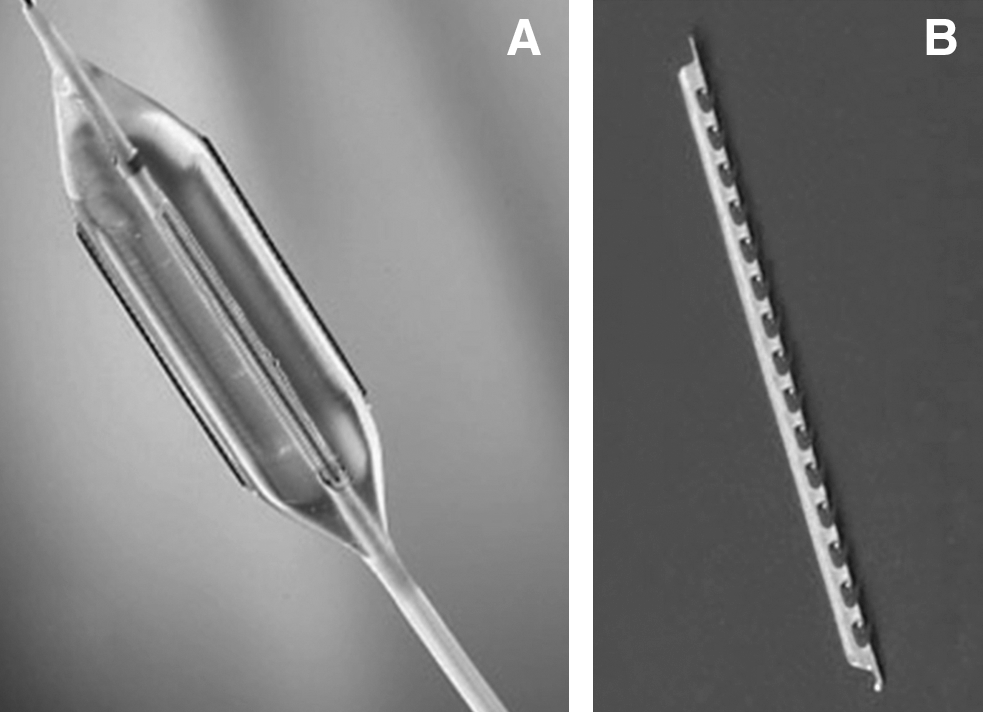
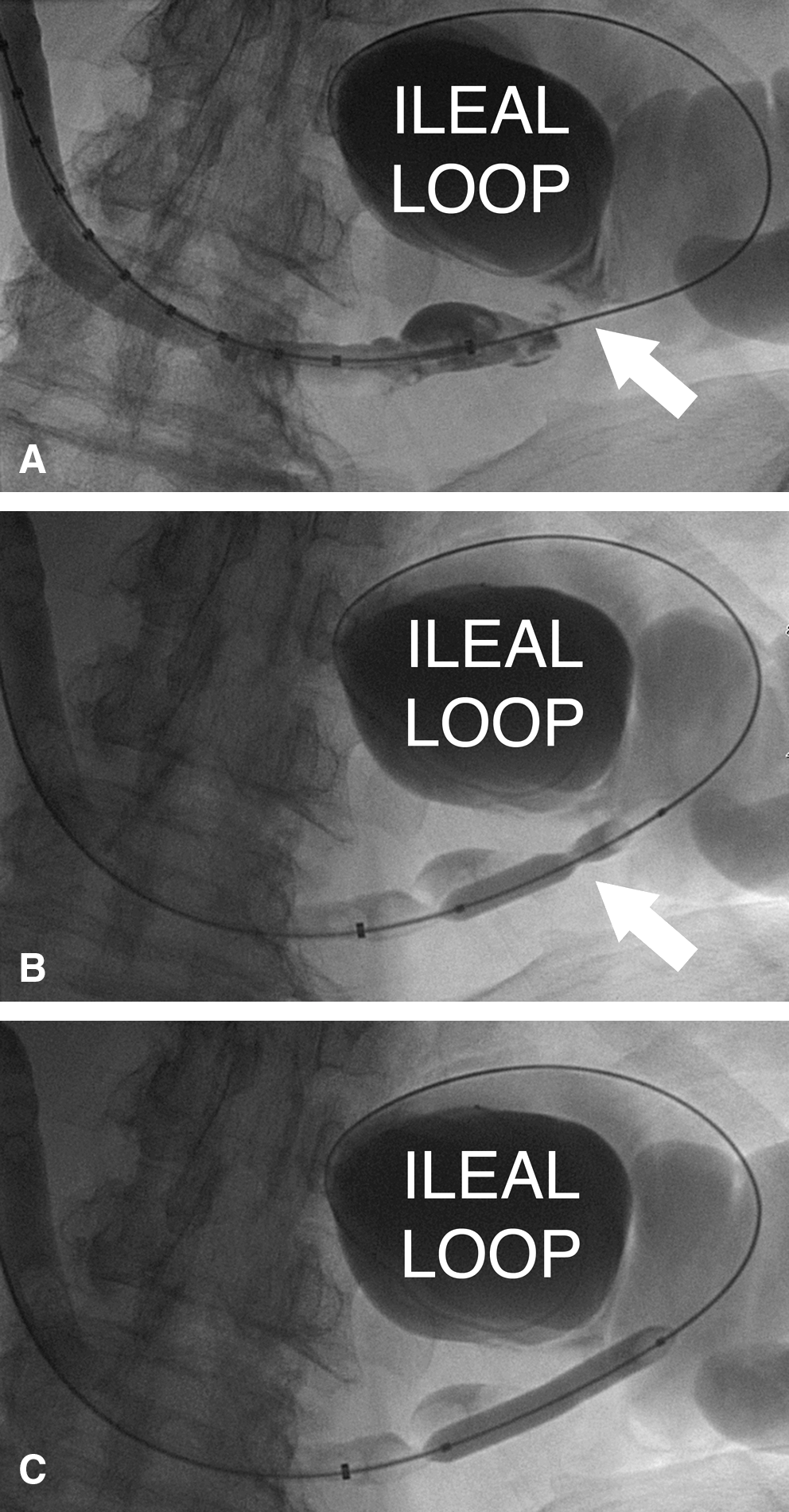
Three male patients (45, 72, and 77 years old) were referred to our institution with a diagnosis of ∼1-cm ureteroenteric stricture after radical cystectomy and ileal conduit. Imaging studies revealed moderate hydronephrosis on the affected side. One patient (45 years old) had a solitary kidney and therefore elevated serum creatinine level. After institutional review board approval and specific informed consent, all patients underwent a transluminal dilatation and incision with PCBD under local anesthesia and fluoroscopic guidance. A guidewire was introduced into the renal pelvis and ureter in antegrade fashion, through a percutaneous nephrostomy puncture, and then passed through the strictured segment. The stricture site was observed under fluoroscopy and the exact length of the stricture was measured using fluoroscopy and radio-opaque measuring stents. The PCBD was subsequently deployed over the 0.018-inch guidewire and the balloon was inflated to pressures up to 6 atm at the stricture site. The maximum diameter of the inflated balloon was 8 mm. Four externally mounted microsurgical blades (atherotomes) incised the stricture (cold cutting) and relieved the obstruction. The length and the height of each atherotome were 2 cm and 0.127 mm, respectively (Fig. 1). There were radio-opaque markers placed on the guidewire tubing at the ends of the atherotomes to provide visual reference points for balloon positioning within the ureter. Approximately 30 seconds later, the balloon was deflated and the enlarged passage from the ureter to the ileal loop was verified under fluoroscopy (Fig. 2). A pigtail stent and a nephrostomy tube were placed. The nephrostomy tube was removed the day following the procedure and the pigtail stent was removed at 6 weeks after the procedure.
(
(
Results
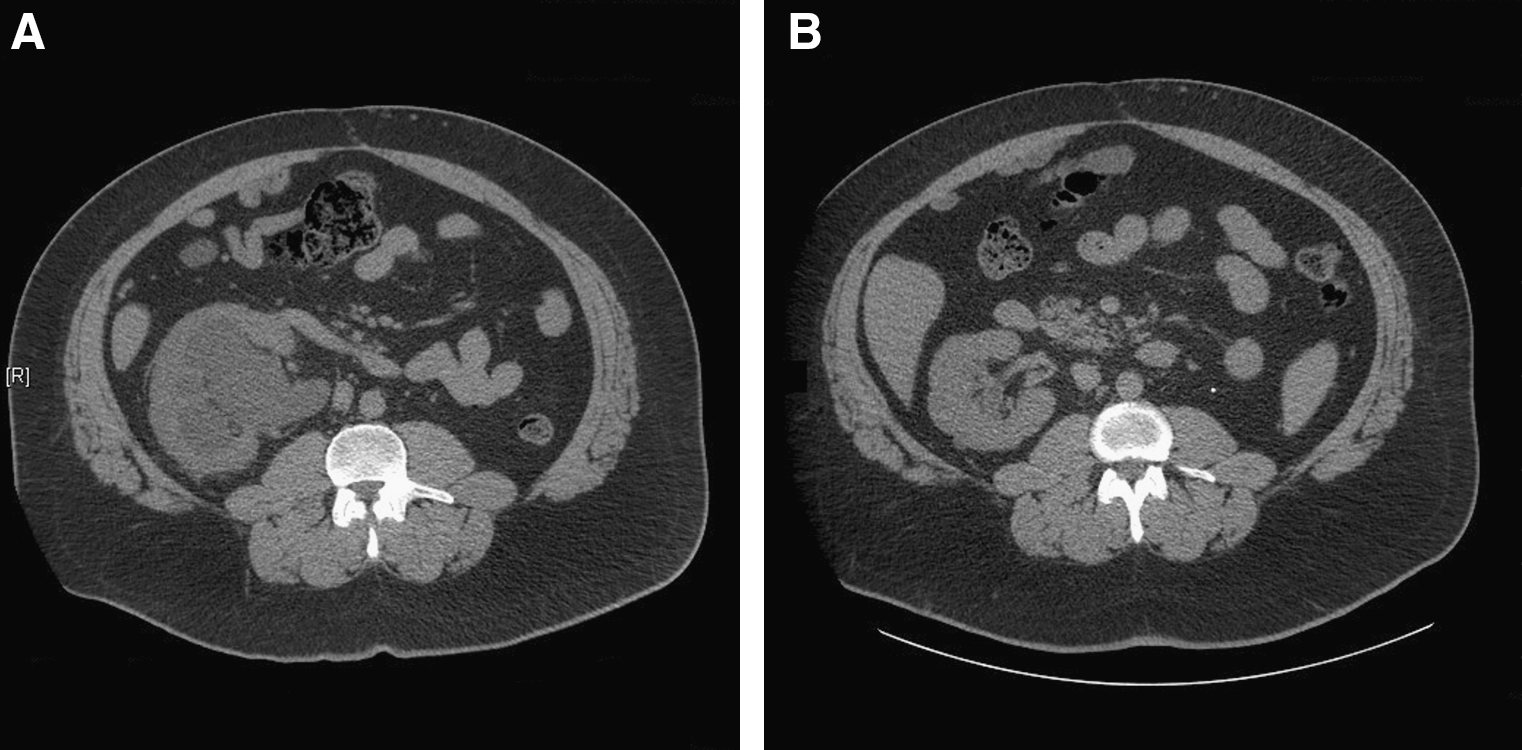
All three procedures were successful in relieving the obstruction. There was no extravasation of the contrast or any other procedural complications. All patients were asymptomatic postoperatively and discharged the day following the procedure. Postoperative computed tomography scans at 3 and 12 months revealed no discernable hydronephrosis in two patients and improvement in the third patient (Fig. 3). The creatinine level in the patient with a solitary kidney decreased significantly following the procedure (Table 1). Postoperative mercaptoacetyltriglycine (MAG-3) renal scans showed improved drainage.
(
Discussion
Ureteroenteric anastomotic strictures are one of the most common complications of urinary diversions. These ureteroenteric strictures are considered as ischemic lesions secondary to periureteral microvascular injury during manipulation and construction of the urinary diversion. Length and side of the stricture, time from initial diversion, previous radiotherapy, and initial renal functions may have an effect on response to treatment. 14 Traditionally, open surgical repair is considered the standard treatment for ureteroenteric anastomotic strictures after radical cystectomy and urinary diversions. 10,14 However, the difficulty of open surgical repair and the associated morbidity for poor surgical candidates have led surgeons to consider and develop minimally invasive alternatives with lower cost, decreased hospital stay, and fewer complications. Despite the lower success rates compared with open surgical repair, several endoscopic treatment options exist for the management of ureteroenteric anastomotic strictures. Short-term success rates of up to 60% have been reported with endoscopic balloon dilatation. 10,15 –17 Unfortunately, long-term patency rates decrease to as low as 5% by 3 years. 10 DiMarco et al 10 reported higher failure rates for strictures longer than 1 cm, occurring within 6 months of ureteroenteric diversion.
Another endoscopic option is endoureterotomy with cold knife, electrocautery, or laser. Poulakis et al 18 reported the results of 40 patients with 43 ureterointestinal anastomotic strictures treated with cold-knife incision. The authors pulled a wire-mounted cold-knife through the strictured area in retrograde fashion under fluoroscopic control and the stenosis was incised circularly three to six times. Successful treatment was defined as radiographic and scintigraphic resolution of obstruction and symptomatic relief. The success rate at 1, 2, and 3 years was reported as 86%, 67.8%, and 60.5%, respectively. Although these results appear promising, no further studies were reported regarding the use of cold-knife for ureterointestinal anastomotic strictures. Nevertheless, studies with Acucise™ and holmium laser have reported varying successful patency rates in long-term follow-up. 9,19,20 Lin et al 20 reported the results of Acucise endoureterotomy in 12 ureteroenteric strictures. The patency rate was 30% in a mean follow-up time of 24 months. Extreme caution should be exercised while incising such strictures without direct vision because trauma to adjacent organs, such as the bowel and blood vessels, is of concern. The herein described PCBD device has four microsurgical blades that do not present the possible hazards of trauma to adjacent organs. Recently, holmium laser incision of ureteroenteric strictures under direct vision has emerged as an option. Varying success rates of 32% to 85% have been reported with laser endoureterotomy. 9,11,19,21 Laven et al 11 performed holmium laser endoureterotomy in 16 renal units with a flexible ureteroscope under direct vision. The authors reported a patency rate of 50% with a median of 3-year follow-up. In a study by Watterson et al 22 that involved 23 ureteroenteric strictures treated with holmium laser endoureterotomy, the success rate at 3 years was 56%.
A review of published literature reveals limited data regarding the use of peripheral cutting balloon devices in ureteral and ureteroenteric anastomotic strictures. 23 –25 In a study published by Iezzi et al, 24 two patients underwent PCBD—one with pelvic tumor externally compressing the distal ureter and one with an endoluminal ureteral tumor—after conventional balloon dilatators failed. The authors were able to incise and dilate the ureters with PCBD in both patients and place the ureteral stents. However, both patients had extrinsic or intrinsic tumors, which is not representative of the patients in our series. Atar et al 25 presented initial results of the PCBD in three ureteric strictures after renal transplantation. The authors reported their success rate as 66% with a mean follow-up of 8 months. Steiner et al 23 performed dilatation and incision with PCBD in two cases with ureteroenteric strictures. The success rate was 100% at a mean follow-up of 9 months. In the present study, we have no failure with PCBD in three patients with a 1-year follow-up (range, 9–17 months). No procedural complications, such as bleeding due to major vascular injury, has been reported with the use of PCBD in the treatment of ureteric and ureteroenteric anastomotic strictures. This novel technique of dilatation and incision of ureteroenteric anastomotic strictures with PCBD seems promising considering that most failures occur within 12 months of initial intervention. With diligent follow-up via imaging and functional studies, PCBD can be considered as an alternative treatment to open repair for poor surgical candidates. Further studies should be conducted with larger series and longer follow-up to define the clinical significance and long-term success rates.
Conclusion
Dilatation and incision with PCBD is a novel approach for the treatment of short ureteroenteric anastomotic strictures of 1 cm or less and is recommended as an initial approach for managing this complex group of patients. Long-term data need to be obtained to establish the efficacy of this technique.
Footnotes
Disclosure Statement
No competing financial interests exist.