
Abstract
Introduction:
Ten-year disease-specific survival for clinically localized prostate cancer after radiation is 93%, 88%, and 80% for low-, medium-, and high-risk groups, respectively. The objective of this study was to report long-term cancer survival outcomes for patients who had undergone prostate cryotherapy at our institution more than 10 years ago. To date, this is the longest reported follow-up after cryotherapy.
Materials and Methods:
A retrospective patient chart review, conducted of an Institutional Review Board (IRB)- approved cryotherapy database, identified 76 men who had undergone prostate cryotherapy before January 1999. Pre-, intra-, and posttreatment data were collected. Primary study endpoints were overall mortality and prostate-cancer-specific death. Secondary endpoints were disease recurrence and clinical progression.
Results:
Mean patient age was 69.2 (47.4–86.3) years; median preoperative prostate-specific antigen was 5.3 (0.2–208.0); mean Gleason score was 7. Forty of 76 (52.6%) were confirmed D'Amico high risk. Median follow-up was 10.1 (0.2–14.9) years; 25 patients underwent primary treatment; 51 postradiation. After 10 years of follow-up, 43 of 76 men (56.6%) were still alive; 33 men (43.4%) had died—10 (13.2%) from prostate cancer, 18 (22.4%) from noncancerous causes, and 5 (6.6%) unknown.
Conclusions:
The long-term results of prostate cryotherapy in our series indicate an 87% overall 10-year prostate-cancer-specific survival, despite early cryotherapy technology and the majority of patients being D'Amico high risk.
Introduction
Published long-term clinical outcome data of patients undergoing prostate cryoablation (especially for cases postradiation therapy that are not ideal cases for salvage prostatectomy) are very limited. Jones et al 4 recently published the largest series of 1198 patients undergoing primary whole-gland cryotherapy, all of whom were included in the industry-sponsored Cryo On-Line Data (COLD) registry. This showed good results from multiple centers, but the median follow-up period was only 2 years. 4 Pisters et al 5 also reported on 56 men with locally recurrent prostate cancer who had undergone salvage cryotherapy as part of a study comparing treatment outcomes against salvage radical prostatectomy. The median follow-up for these patients was only 5.5 years, with no significant difference in disease-specific survival.
The objective of this study was to determine the long-term cancer-specific and overall survival outcomes for patients who underwent total gland cryoablation of the prostate more than 10 years ago. The data on 76 men presented herein include patients treated before January 1999 and are more than any prior series at a single institution.
Materials and Methods
Patient data were prospectively collected into the Urologic Oncology prostate cryosurgery database after receiving approval from the institutional review board. This database includes information on patient age, race, presenting and preoperative prostate-specific antigen (PSA) levels, clinical stage, Gleason grade of cancer on diagnostic biopsies, primary or salvage treatment, follow-up PSA levels, and need for adjuvant hormones. The AJCC Cancer Staging Manual 5th edition was used for pathological tumor staging. 6 Patients were also stratified according to the 2001 D'Amico risk criteria for low-, medium-, and high-risk disease. 7
Eligible patients for our analysis included men who underwent either primary or salvage (after primary external beam radiotherapy or brachytherapy) prostate cryotherapy for the treatment of localized prostate cancer more than 10 years ago, between January 1994 and January 1999. Before treatment, all patients had a negative metastatic evaluation, including nodal imaging of the abdomen and pelvis, as well as a bone scan. Data on relevant pre-, intra-, and posttreatment information were retrospectively reviewed. For all procedures the whole gland was treated by a single surgeon (A.E.K.) using either the Endocare (Endocare, Inc., Austin, TX) or the Galil cryotherapy surgical system (Galil Medical, Inc., Arden Hills, MN) at Columbia University Medical Center New York, a tertiary care academic U.S. center.
Primary and secondary endpoints
The primary endpoints for analysis included overall mortality and prostate-cancer-specific death. Secondary endpoints were disease recurrence and clinical progression. Biochemical recurrence (BCR) was defined using the definition as formulated at the second Radiation Treatment Oncology Group (RTOG)–American Society for Therapeutic Radiology and Oncology (ASTRO) Consensus Conference in Phoenix 2005 for patients after external beam radiotherapy for prostate cancer: a PSA serum level rise by 2 ng/mL or more above the nadir PSA was considered biochemical failure after cryoablative therapy of the prostate. 8 Disease-free survival was calculated using Phoenix criteria (biochemical failure = nadir + 2 ng/mL) 8 and follow-up transrectal ultrasound (TRUS) biopsy results.
Information was obtained regarding patient mortality by searching for death information using their social security number. For some patients, the next of kin or the family physician had already notified our institution that the patient had died. Patients lost to follow-up were contacted via telephone to confirm living status.
Procedure: cryoablation of the prostate
The procedure was performed using either second-generation (using both liquid nitrogen and argon gas) or third-generation (argon alone) technologies. The TRUS-guided percutaneous cryosurgery procedure has been previously described. 9 The prostate gland dimensions were analyzed via TRUS, as well as location of the urethra, peripheral zone, and the distance to the capsule, to determine the optimal geometry placement of either 17-gauge (1.47 mm) cryo-needles or 2.4-mm cryo-probes and thermocouples.
Under TRUS guidance, the needles/probes were placed through the skin of the perineum, approximately 10 mm apart, within 5 mm of the capsule. The sharp tip of each needle allows direct percutaneous insertion, with the patented needle technology producing precise and accurate ice balls.
As the gas was delivered through the specialized needles, the prostate tissue was rapidly cooled to the target temperature of (40°C. The ice ball was clearly visible on TRUS as it formed and was monitored continuously throughout the procedure. A double freeze–thaw cycle was performed under TRUS guidance according to standard protocols. 9 This has been shown to have significantly better outcomes of biochemical failure-free and local recurrence-free survival rates compared with one cycle. 10 Temperatures were monitored with thermal sensors to ensure complete ablation of targeted tissue. Patients were discharged on postoperative day zero with a temporary urethral catheter.
Statistical analyses
Data were summarized as the medians and ranges for continuous variables, and in frequency tables for categorical variables. Kaplan–Meier curves were constructed to determine overall and cancer-specific survival rates. The statistical software package SPSS 12.0 for Windows (SPSS, Inc., Chicago, IL) was used for all statistical analyses.
Results
Of the 76 men identified who underwent total gland prostate cryotherapy between January 1994 and January 1999, 25 had a primary treatment and 51 received salvage prostate cryosurgery (i.e., postradiation) when they were found to have recurrent disease on prostate biopsy.
The preoperative demographic and clinicopathological characteristics of the study population are presented in Table 1, illustrating differences in patient age, clinical stage, Gleason grade, and median presenting PSA between primary and salvage cases. Median overall patient age was 69.2 years (range 47.4–86.3) with median follow-up of 10.1 years (range 0.2–14.9). Clinical stage was only documented in 12 out of 76 men (T1 n = 2, T2 n = 2, T3 n = 8, T4 n = 1, unknown T stage n = 64). However, based on PSA data, Gleason score, and those with known clinical stage, 40 of 76 (52.6%) were confirmed to be D'Amico high risk. Median preoperative Gleason score was 7 (range 4–10); 8/25 (32%) and 22/51 (43%) were poor Gleason grade for the primary and salvage groups, respectively. Median preoperative serum PSA level was 31.78 ng/mL (range 3.3–2085) for primary cases and 6.43 ng/mL (range 0.2–50) for salvage cases. Table 2 details presenting PSA values for the group overall and those who died of prostate cancer versus other causes.
PSA = prostate-specific antigen.
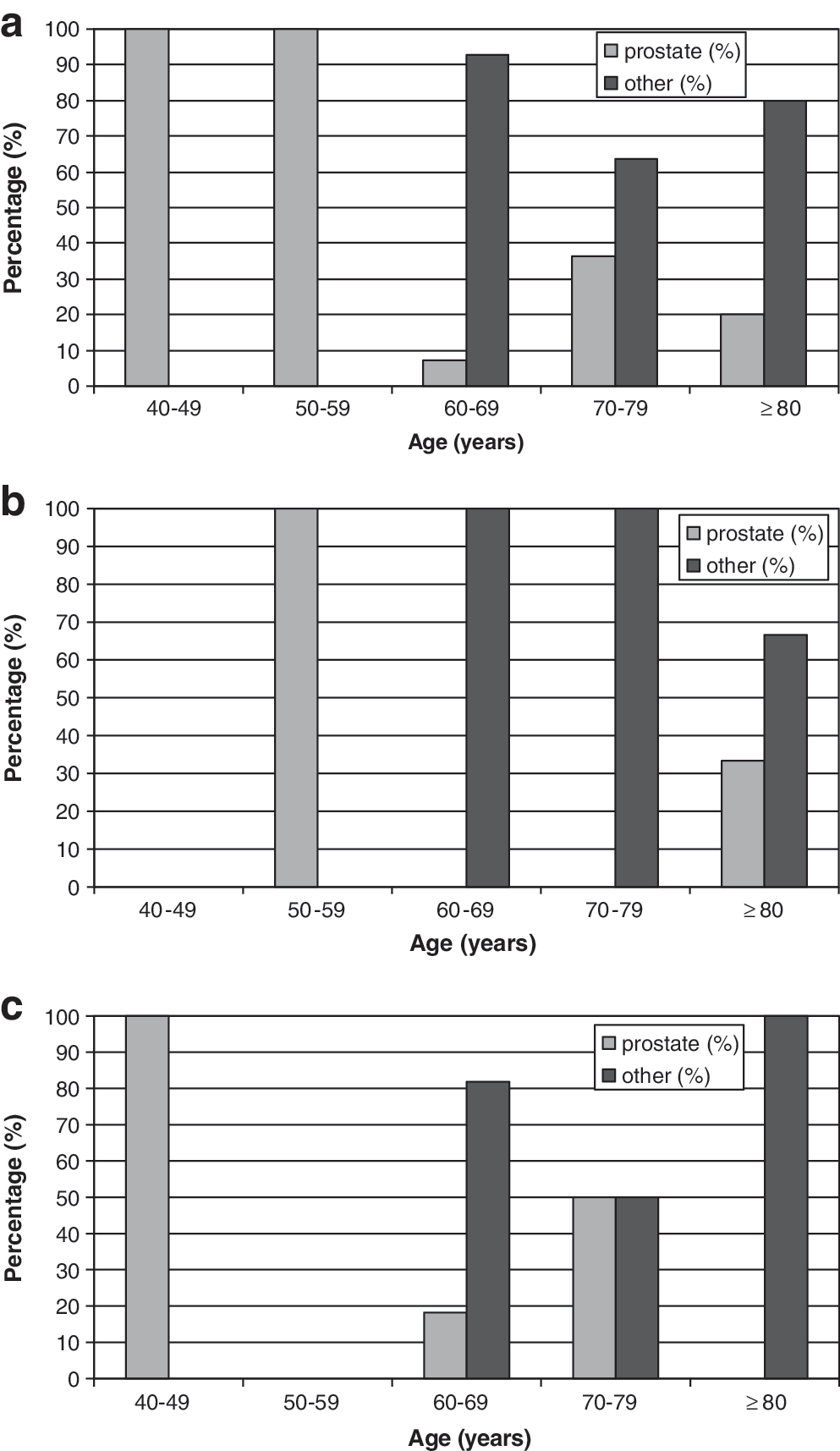
After 10 years of follow-up, 43 out of 76 men (56.6%) were confirmed alive; 29 (67.4%) and 21 (48.8%) men had follow-up beyond 5 and 10 years, respectively. For the 33 men (43.4%) who died, the cause of death (including cause of death by patient age at diagnosis of prostate cancer) for primary and salvage cases is illustrated in Figures 1 –3. The preoperative demographic characteristics for those who died of prostate cancer are presented in Table 3.
(

Cause of death in 10 patients who died after having undergone a primary cryoblation.
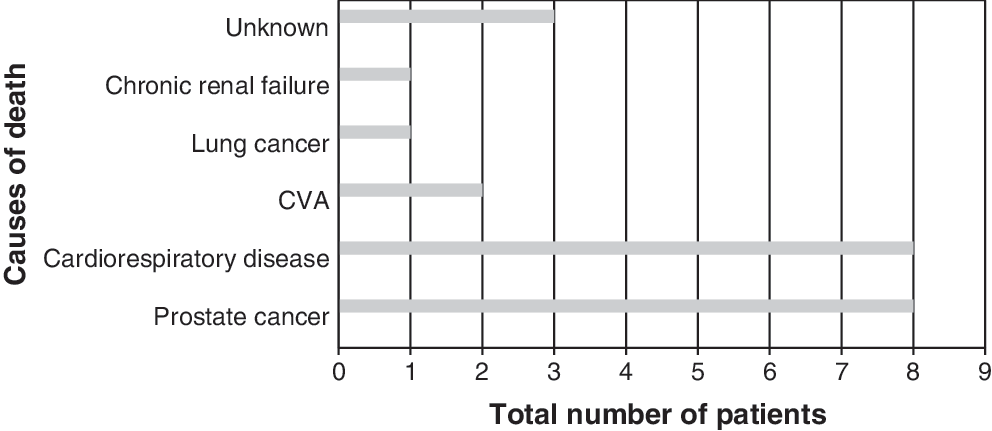
Cause of death in 23 patients who died after having undergone a salvage cryoblation. CVA = cardiovascular accident.
Overall, 10 patients (13.2%) had died of prostate cancer (2 primary cases, 8 salvage cases), and 18 (23.7%) had died of nonprostate cancer causes (13 from cardiac or respiratory disease, 2 from a cardiovascular accident, 1 from lung cancer, 1 liver failure, and 1 chronic renal failure). For five men (6.6%) the cause of death was unknown. The Kaplan–Meier curves for overall survival and prostate cancer disease-specific survival are shown in Figures 4 and 5, respectively. Median time to death for the different causes for primary and salvage cases is detailed in Table 4. One patient died 8 months after primary cryoablation for a Gleason 8, T3 cancer from cardiovascular disease, not prostate cancer. The patient with a presenting PSA of 208 ng/mL, negative metastatic survey, and a Gleason 9, T3 disease who underwent primary cryoablation died 103 months after treatment from alcoholic liver disease.

Kaplan–Meier curve showing overall survival.
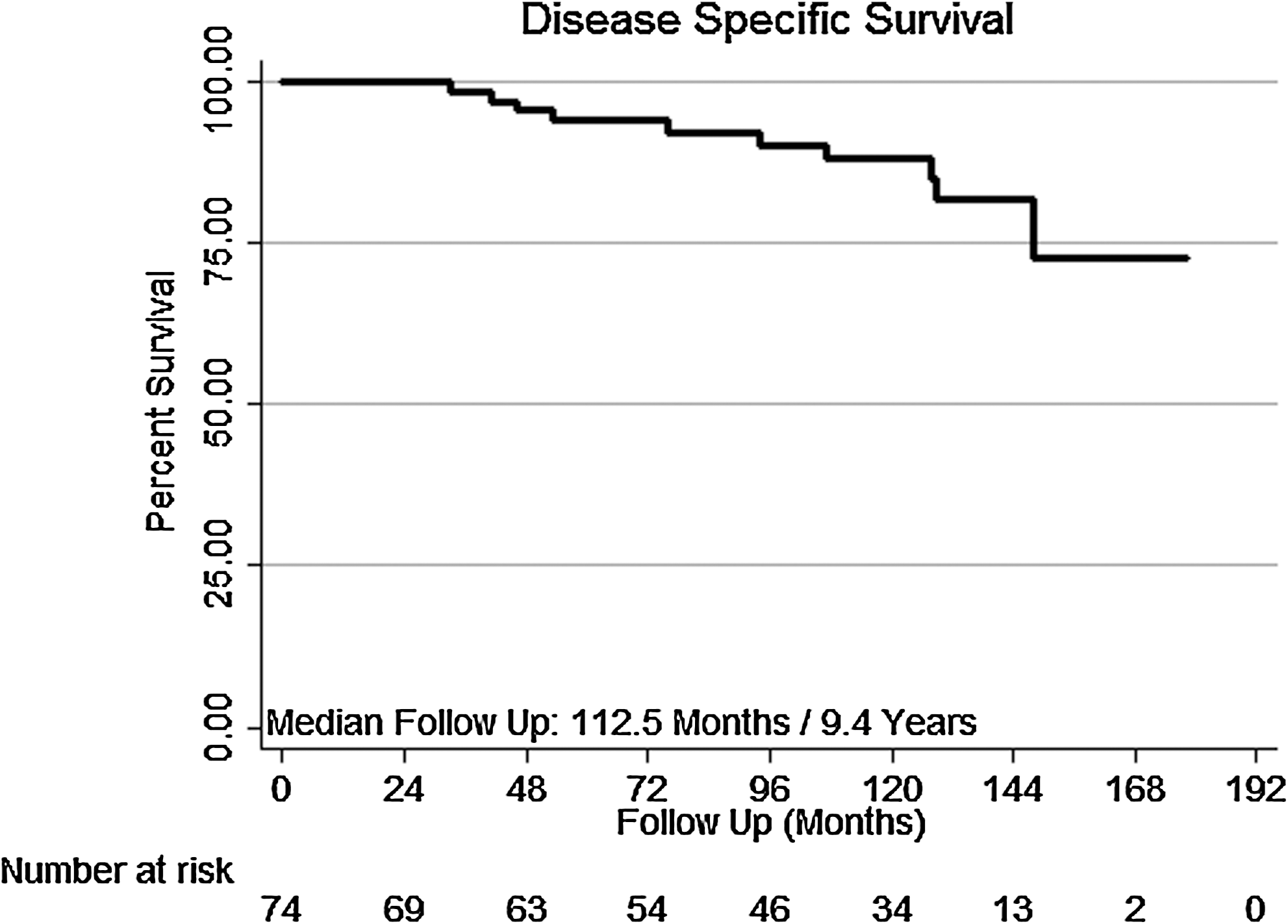
Kaplan–Meier curve showing prostate cancer disease-specific survival.
The number in brackets denotes the number of patients who died in each group.
According to the Phoenix definition, of the 43 men still alive, 21 (48.8%) patients met criteria for biochemical failure. For eight patients (18.6%) confirmed still alive, their biochemical status was unknown as a result of being lost to follow-up. Figures 6 and 7 delineate the time frame for those who had biochemical failure in the primary and salvage groups, respectively. Overall, 24% had biochemical failure within 1 year, 19% between 2 and 4 years, 19% between 5 and 7 years, 14% between 8 and 10 years, and 24% between 11 and 13 years.

Primary cryoablation treatment to biochemical failure time frame.

Salvage cryoablation treatment to biochemical failure time frame.
Of those 21 patients with known biochemical failure, 14 (66.7%) underwent TRUS prostate biopsy for clinical suspicion of recurrent disease. The number of cores taken for those undergoing a TRUS biopsy ranged between 8 and 12 cores. Those who had a TRUS biopsy after 2002 had 12 cores taken than those who had biopsies early on in the study period; 12 (57.1%) had no evidence of recurrent cancer histologically. The two (9.5%) patients with histological evidence of recurrent prostate cancer were salvage cryotherapy cases and are detailed below.
One patient had Gleason 9 (5 + 4) radiation recurrent cancer in the right lobe of the prostate before undergoing salvage cryotherapy in February 1996. His repeat prostate biopsy performed 22 months later for a rising PSA revealed Gleason 10 (5 + 5) disease in 2 out of 5 cores from the right lobe only. His metastatic survey was negative. His PSA was <1.0 ng/mL on hormone therapy in 2004 when he was lost to follow-up at our institution, but he remains alive.
The second patient had Gleason 8 (4 + 4) radiation recurrent cancer in the left lobe of the prostate before undergoing salvage cryotherapy in March 1998. His repeat prostate biopsy performed 33 months later for a rising PSA revealed Gleason 8 (4 + 4) disease in the left lobe only. He was scheduled for repeat cryoablation, but this was aborted because of inability to place a thermocouple in the external sphincter at the time of the procedure. He was thus treated with hormones and is still alive with a PSA <1.0 mg/mL and a negative metastatic survey.
None of the patients with biochemical failure had evidence of clinical progression of disease. On imaging performed for a metastatic survey, only one patient had a suspicious bone scan result. This patient had undergone radiotherapy after an aborted radical prostatectomy because of tumor extension in 1992. He then had a salvage cryoablation for Gleason 7 (3 + 4) radiation recurrent prostate cancer in the left lobe in 1998. Repeat prostate biopsies performed for a rising PSA in 2002 and 2003 were entirely negative. A bone scan in October 2007 was suspicious for metastatic disease, but subsequent plain films of the ribs and thoracic spine did not confirm metastatic disease. He remains alive with a current PSA of 12.8 ng/mL.
It was not possible to confirm how many men truly had preoperative or postoperative hormonal ablation because of inadequate and inconsistent medical record documentation. It was thus not possible to tease this information out of the BCR rate.
Discussion
Prostate cryosurgery is a thermal therapy that extracts heat from the targeted tissue, resulting in a series of destructive effects. 11 Prostate cryoablation first took place in 1964. 12 Early studies, performed using probes cooled by liquid nitrogen in a closed system, limited the ability to control the growth of the ice ball. 13 Follow-up reports demonstrated a curative potential equivalent to radiation and surgery. 14 However, inability to control the ice ball, coupled with improper cryoprobe replacement, led to unacceptably high complications 10,15 ; as a result, prostate cryosurgery fell into disuse.
In the mid-1990s, the development of argon-based cryotherapy systems using ultrathin 17-gauge needles with echogenic tips, has since allowed highly controlled and accurate delivery of the treatment. Thermocouples introduced through the perineal skin into different zones of the prostate, as well as the area of the urethral sphincter, monitor temperature changes. 16 The development and implementation of transrectal (TRUS) ultrasound guidance, advancing imaging techniques, and urethral warming devices (to reduce the incidence of urethral sloughing) has led to improved results using newer multiprobe devices. 17,18
The application of prostate cryotherapy, for both primary and recurrent localized prostate cancer is now supported by the American Urological Association, 19 The European Association of Urology, 20 and the U.K. National Institute of Clinical Excellence. 21,22 However, despite technical advances and recent published studies approving prostate cryoablation, the legacy of publications from the 1990s 10,16 (reporting significant complications) means that it remains a controversial treatment option.
One of the larger primary series of patients to date, with the longest follow-up, included 590 subjects followed for a mean of 5.4 years. 23 Relatively few late failures occurred beyond 24 to 36 months. 23 Jones et al 4 recently published the largest series of patients undergoing cryotherapy as primary treatment, all of whom were included in the industry-sponsored COLD registry: 1198 men managed by 27 physicians with a mean follow-up period of 24.4 ± 25.9 months. Five-year actuarial BCR-free survival rates were reported to be 72.9% using the Phoenix definitions. 24 However, this definition (intended to predict outcomes only at a point 2 years short of median follow-up) was misused; thus, outcomes may be expected to worsen somewhat with further follow-up.
Patients who experience disease progression after radiation therapy have few options for potentially curative therapy. Cryotherapy is an option for patients who have pathological evidence of locally recurrent disease without clinical or radiological evidence of metastatic disease. Longer-term salvage data are now becoming available. Bahn et al 25 reported 7-year salvage biochemical failure-free rates of 59% to 69%. Pisters et al 26 recently reported outcomes for salvage cryotherapy among 279 men from the COLD registry, the largest salvage series to date. Good biochemical and local control rates were reported, supporting the use of this treatment for localized recurrence after failed radiation therapy. However, preprocedure PSA levels of more than 10 ng/mL, biopsy Gleason scores > 8, and clinical stage T3–T4 disease predicted biochemical failure. 26
The current study is the first to report on survival beyond 10 years of prostate cryotherapy for localized prostate cancer (over 50% of whom were D'Amico high-risk salvage cases), a valuable addition to the cryotherapy literature despite small numbers. It was encouraging that 15/25 (60%) and 28/51 (55%) in the primary and salvage groups were alive at 10 years. Our study was not primarily intended to determine the differences between primary and salvage groups. Obviously, the men who underwent salvage ablation have a history of prostate cancer that is much longer than the primary group and it is not surprising that 8 out of 23 deaths in the salvage group were prostate cancer deaths (35%) compared with 2 out of 10 (20%) in the primary group. Median time to death for those who died of prostate cancer was longer in the primary arm (100.5 months) than the salvage arm (81.75 months) although numbers were small and this was not statistically significant. Median time to death for those who died of nonprostate cancer causes was shorter in the primary (49.7 months) than in the salvage arm (108.4 months, p-value = 0.001). This is somewhat surprising, but may be explained by the fact that patients undergoing primary cryoablation may already have more comorbidity (excluding them from other treatments like surgery or radiation) and thus are more likely to die from nonprostate cancer causes. Those undergoing salvage cryoablation also had a much lower presenting PSA (6.43 ng/mL) than the primary group (31.78 ng/mL), which may reflect less aggressive disease as well as the confounding effect of any hormonal treatment in the salvage group.
Some limitations of this study should be noted. It should be recognized that this is a single-institution study and the results may not generalize to other centers. Cryo-ablation remains operator dependent, and complication rates, as well as biochemical and clinical outcomes, have varied according to site, technique, and indications. Treatment is becoming more standardized and data from the COLD Registry support that whole-gland cryoablation practiced in a spectrum of academic and community centers, and maintain efficacy and morbidity similar to that of single-center reports. 4
Defining BCR after localized prostate cancer treatment is controversial. This variation in definition creates great difficulty in comparing outcomes across treatment modalities and is no less of a problem in the case of cryotherapy. A unique specific definition for PSA recurrence after prostate cryoablation currently does not exist. PSA thresholds of 0.4, 0.5, and 1 ng/mL have all been used to define failure after cryotherapy, as have both the original ASTRO definition of three consecutive rises after nadir and the updated Phoenix definition of nadir plus 2 ng/mL. 8 In addition, a positive biopsy is usually required, regardless of which definition is used.
In our study we used the Phoenix criteria for definition of BCR after cryosurgery. Although 21 of 43 (48.8%) men alive met the criteria for biochemical failure, only 14 of these patients underwent a posttreatment biopsy.
Numerous disease- and treatment-related factors have also been shown to predict rates of local control. In one series, for example, the likelihood of positive biopsy findings was 9% in subjects with clinical stage T1 or T2 disease, compared with 21% in those with T3 disease.
Prepelica et al 27 reported a series of 65 men with high-risk prostate cancer, defined as a PSA level of ≥10 ng/mL and/or a Gleason score of ≥8. They found an 83.3% biochemical disease-free survival rate based on the ASTRO definition at a median 35-month follow-up. The median follow-up in this study was clearly shorter than that in our series. Further, the variations in definitions of biochemical failure may account for differences in comparing outcomes with other studies where different definitions of biochemical failure are used. This emphasizes the need for a definition of PSA recurrence after cryosurgery.
Of note, it is also unknown how many patients in our cohort had received neoadjuvant or adjuvant hormonal therapy, which also makes direct comparison of the two groups difficult to assess. This may explain the difference in presenting PSA values for the two groups shown in Table 1, where patients with locally recurrent prostate cancer may well have been put on hormones for a rising PSA before undergoing a salvage cryoablation. Further, neoadjuvant hormone therapy is sometimes prescribed for shrinking larger prostates before treatment to facilitate whole-gland ablation. However, there is no documented evidence of survival benefit from hormone therapy before salvage cryosurgery. 27
Conclusions
Despite the limitations discussed, the current study is the first to report on long-term survival beyond 10 years of prostate cryotherapy for localized prostate cancer. This is despite early cryotherapy technology and over 50% of our patients being D'Amico high-risk salvage cases.
In conclusion, the long-term results of prostate cryotherapy in our series reveal an 87% overall 10-year prostate-cancer-specific survival and encouraging biochemical and local control rates.
Our findings suggest that prostate cryoablation can result in long-term progression-free survival in a subset of carefully selected, high-risk men who have been adequately staged to confirm localized disease. Further, patients undergoing prostate cryotherapy may have a cancer-specific survival advantage compared with those electing for radiation or hormones alone. However, only a randomized trial can control for the many known and unknown confounding factors that can affect long-term outcomes.
Footnotes
Disclosure Statement
No competing financial interests exist.