
Abstract
Introduction:
Carbon dioxide (CO2) lasers deliver energy with minimal thermal spread to tissues during dissection. Excess thermal spread during dissection of the neurovascular bundle (NVB) can affect potency in men after robot-assisted radical prostatectomy (RARP). We report on a novel delivery mechanism for CO2 laser energy through a flexible fiber to enhance accuracy of NVB dissection during RARP.
Materials:
A feasibility study of the OmniGuide® BeamPath™ URO-LG CO2 laser fiber for NVB dissection was performed on 10 patients with primary Gleason 3 T1c prostate cancer during RARP. Bilateral lateral fascial antegrade nerve sparing was performed. We evaluated fiber performance, safety, and efficacy.
Results:
The fiber was inserted through the 12-mm assistant's port and easily manipulated by robotic instruments. Once pedicles were clipped and dissected, the laser fiber was effective in establishing planes of dissection between prostatic capsule and NVB. The endoscopically discernable thermal laser footprint was small, with minimal thermal spread during nerve sparing, meticulous dissection of NVB, and fascial layer identification. Although the laser did provide extremely accurate dissection, it was unable to serve as an adequate means of larger vessel coagulation.
Conclusions:
The flexible CO2 laser fiber was easily manipulated. Identification of fascial layers during nerve sparing was facilitated with the fiber. Long-term follow-up is necessary to determine efficacy of this technology versus conventional techniques on the NVB. Larger studies are currently in progress to determine if use of the flexible CO2 laser fiber results in improvements in functional outcomes with regard to return of sexual potency after RARP.
Introduction
Excess thermal spread during dissection of the neurovascular bundle (NVB) can affect potency in men after robot-assisted radical prostatectomy (RARP). 10
As such, we performed a pilot evaluation of a novel delivery mechanism of CO2 laser energy 11 through a flexible fiber to enhance accuracy of dissection of the NVB during RARP. The current study represents, to the authors' knowledge, the first series to evaluate the fiber in this setting.
Materials and Methods
Table 1 shows baseline demographic data. Mean patient age was 62.1 (54–71) years. Mean body mass index was 24.7 (range 21.5–29) kg/m2. Median preoperative PSA was 5.5 (range 1.56–18.0) ng/mL. All patients had either Gleason 6 (3 + 3) or Gleason 7 (3 + 4) T1c disease. Mean international prostate symptom score was 9.0 (range 1–18) and mean sexual health inventory for men was 20.4 (range 0–25).
BMI = body mass index; IPSS = international prostate symptom score; PSA = prostate-specific antigen; SHIM = Sexual Health Inventory for Men.
A feasibility study was conducted using the OmniGuide® BeamPath™ URO-LG CO2 flexible laser fiber (Omniguide, Inc.) to undertake NVB dissection on 10 patients undergoing RARP (Fig. 1).

The OmniGuide BeamPath URO-LG carbon dioxide laser fiber.
All 10 patients had undergone a 12-core prostate biopsy that had revealed a primary Gleason 3 (3 + 3 = 6 or 3 + 4 = 7) adenocarcinoma of the prostate and were clinical staged preoperatively as having T1c disease, with a negative preoperative metastatic survey.
Data on these 10 patients were also prospectively collected into a database after receiving approval from the institutional review board. This database includes information on patient age, race, height, weight, co-morbidity (classified using the Charlson Co-morbidity Index) clinical stage, cancer grade on diagnostic biopsies, preoperative prostate-specific antigen (PSA) levels, preoperative and postoperative urinary function (assessed using the validated international prostate symptom score questionnaire), preoperative and postoperative sexual health inventory for men scores, operative time, estimated blood loss, type of nerve sparing, surgical specimen pathology (tumor grade, stage, and surgical margin status), and follow-up PSA levels. The AJCC Cancer Staging Manual 5th edition was used for pathological tumor staging. 12 All patients underwent a detailed medical history. Body mass index was examined as a categorical variable using the National Institutes of Health definitions of obesity (>30 kg/m2).
Each patient underwent RARP performed by a single surgeon (K.K.B.) using the four arm daVinci S (Intuitive Surgical) surgical system at Columbia Medical Center New York, a tertiary care academic center. For each patient bilateral lateral fascial nerve sparing was performed in an antegrade fashion, using anatomic foundations described by Walsh et al, 13 Menon et al, 14 and Ahlering. 15
Careful apical dissection was used to preserve the external sphincter mechanism and puboprostatic ligaments. During apical and seminal vesicle dissection, minimal electrocautery was applied. Upon identification of the NVB, the bedside assistant gently inserted the flexible laser fiber through the 12-mm right lateral assistant port and directed it toward the pelvis using laparoscopic graspers. The bedside assistant then presented the fiber in the jaws of the robotic needle driver, where the console surgeon was then able to manipulate the fiber into an optimal orientation in relation to the NVB. The console surgeon then activated the CO2 flexible laser fiber via a foot pedal control adjacent to the console to perform bilateral dissection of the NVB.
We evaluated the performance, safety, and efficacy of the OmniGuide BeamPath URO-LG fiber.
Results
The performance, safety, and efficacy of the OmniGuide BeamPath URO-LG fiber (Fig. 1) were evaluated. The mean total operative time was 3 hours.
Figure 2 shows the Omniguide CO2 laser machine, with the attached flexible fiber being inserted through the 12-mm assistant port. The size of the fiber allowed adequate space to be available for simultaneous insertion of standard 5-mm laparoscopic tools. The fiber was inserted through the port without resistance and directed into the pelvis by the bedside assistant using laparoscopic graspers in the assistant's left hand (illustrated in Figure 3).
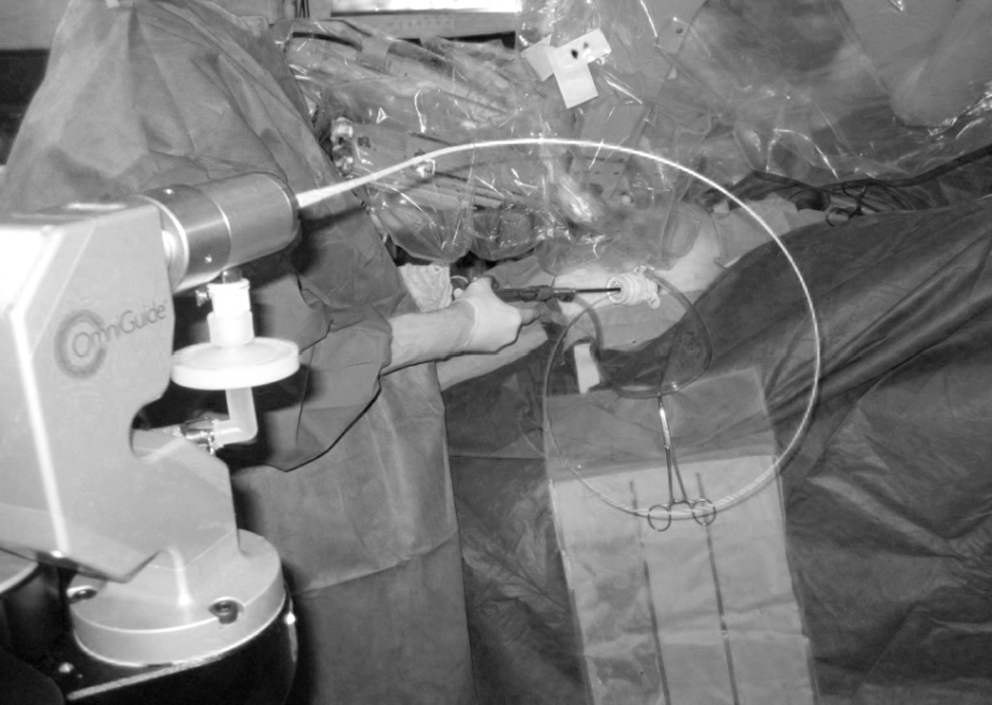
The OmniGuide laser machine is shown, with the attached flexible fiber being inserted through the right lateral 12-mm assistant port and then directed into the pelvis by the bedside assistant using laparoscopic graspers.

A close-up photograph showing the laser fiber in the assistant's right hand being inserted through the 12-mm assistant port, with the aid of the laparoscopic graspers in the assistant's left hand to direct the laser fiber toward the pelvis.
The bedside assistant then presented the fiber in the jaws of whichever robotic instrument (either the robotic needle driver or the PK® bipolar forceps [Gyrus ACMI]) was being used to grasp the fiber. The fiber was easily manipulated by both robotic instruments. For the first two cases, the fragile laser fiber was damaged when held directly in the toothed jaws of the robotic instruments. The fiber was thus modified for subsequent cases by the addition of an external transparent plastic sleeve (shown in Figs. 3 and 4) to allow easy nontraumatic grasping of the flexible fiber using the robotic graspers.
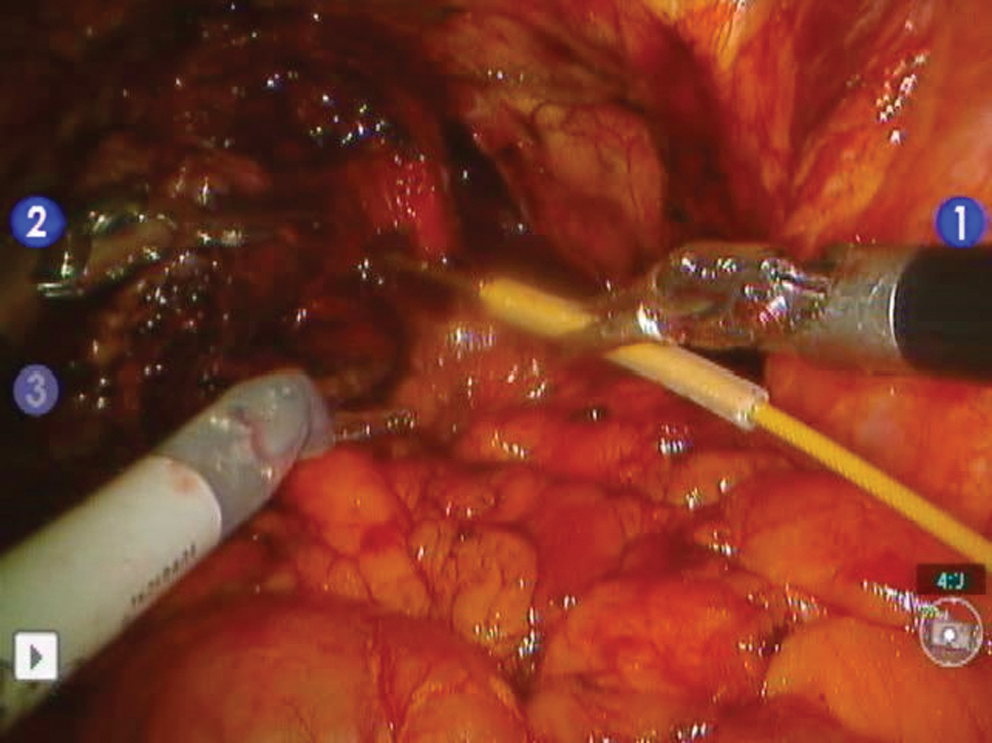
The robotic graspers (labeled instrument 1) are holding the flexible carbon dioxide laser fiber in the middle of the plastic modified sleeve, with the laser fiber tip positioned at the base of the right neurovascular bundle. Instruments 2 and 3 are the left arms of the robot.
Figure 4 shows the robotic graspers (labeled instrument 1) holding the flexible CO2 laser fiber in the middle of the plastic modified sleeve, with the laser fiber tip positioned at the base of the right NVB ready to perform the dissection.
Once the pedicles were clipped and dissected, the console surgeon was then able to orient the flexible laser fiber into an optimal position in relation to the NVB before laser dissection of the bundle. The CO2 flexible laser fiber was activated via a foot pedal control, which was positioned adjacent to the console. Bilateral laser dissection of the NVB was performed. Figure 5 is a close-up photograph showing dissection of the right NVB.

Close-up photograph showing dissection of the right neurovascular bundle.
The use of the laser fiber was safe with precise soft tissue cutting. It was also very effective in establishing the plane of dissection between the prostatic capsule and NVB. Visual examination indicated that the thermal footprint of the laser was small, with minimal visual thermal spread during the nerve sparing part of the procedure. This resulted in meticulous dissection of the NVB and identification of the appropriate fascial layers. There was minimal smoke produced, with no resultant effect on obscuring vision. Although the laser did provide extremely accurate dissection, it was unable to serve as an adequate means of coagulation in larger vessels.
The mean reported operating time was 165.9 minutes. The mean estimated blood loss was 124 mL. No patients were transfused either peri- or postoperatively. From a functional standpoint, 7 out of 10 patients (70%) had gained urinary continence (as defined by zero pad usage in 24 hours) at 6 weeks after surgery. Nine out of 10 patients (90%) had gained urinary continence (as defined by zero pad usage in 24 hours) at 3 months after surgery. It was unknown whether the 10th patient (who was not continent at 6 weeks) had regained urinary continence at 3 months, as he did not attend his 3-month follow-up appointment. It was too early to obtain any meaningful potency data or to determine the oncological safety of this nerve sparing approach.
Discussion
The OmniGuide BeamPathURO-LG CO2 laser fiber (Omniguide, Inc.) is a novel flexible fiber that transmits CO2 laser energy with minimal absorptive loss. Previous histological studies conducted on various animal models have demonstrated minimal thermal spread during dissection, confirming the inherent precision of CO2 laser energy when applied to soft tissue. In a recent porcine study the CO2 laser produced consistent incisions with narrow, well-defined areas of surrounding desiccation and edema. 4,5 These findings are consistent with earlier assessments of the CO2 laser, including a porcine study demonstrating a maximal increase in tissue temperature of only 4°C within 0.5 mm of the site of use of the CO2 laser. 6
The CO2 laser is widely used in head and neck oncological surgery, 2 treatment of benign airway disease, and stapes surgery. 3 It has also been reintroduced in neurosurgical oncology, 4 resulting in predictable penetration depth and minimal collateral damage. 5,6 However, until recently, use of CO2 lasers as surgical tools has been limited by the necessity for their delivery through a rigid, rather than an efficient, fiber-based flexible delivery system. 7 –9
Not only does development of the flexible fiber lend itself to use in open surgical procedures, but also its flexible nature is probably more advantageous in endoscopic minimally invasive procedures in conjunction with both rigid and flexible endoscopes, that is, laryngoscopy, 16 gastroscopy, 17,18 colonoscopy, laparoscopy, 19 thoracoscopy, hysteroscopy, and bronchoscopy. 20 Otolaryngology was the first specialty to adopt the flexible OmniGuide CO2 laser technology, in a commercial format, since early 2007. The body of evidence available since the late 1960s commenting on the efficacy of CO2 lasers for precision microsurgery in otolaryngology was deemed sufficient to warrant routine use of this laser. 16 Further, use of the laser in neurosurgical oncology (cranial and spinal tumors) since late 2008 means that outcome data are evolving in this field too. Prior evaluations in gastroenterology have also been positive, for both lesion dissection and vaporization. More recently, gynecology surgeons, who already use the CO2 laser (rigid, line-of-sight) in trans-vaginal and laparoscopic applications, have shown interest in the flexible fiber technology.
We have adopted the technology of the OmniGuide BeamPathURO-LG CO2 laser fiber and integrated it into one of the surgical steps of RARP. The basic chassis of the BeamPath laser remained the same. However, two major modifications were made to adapt the fibers to the laparoscopic environment. First, the protective jacket was changed to add higher density of stainless steel. This increases the robustness of the fibers, to minimize accidental damage that may occur because of use in a robotic environment that does not have haptic feedback. Second, the tip of the fiber was modified to add a grasping surface so that the fiber could be articulated with laparoscopic and robotic instruments. Further, changes are currently underway to optimize this technology for use as a prostatectomy tool. The tip configuration is being changed to make grasping easier. To facilitate blunt dissection, an additional metal cannula is being added to the fiber that allows easier hand-over-hand sweeping.
Each NVB lies adjacent to the prostate. The type of nerve sparing performed (where nerve sparing units are considered individually) on each side during RARP is usually in one of three planes, determined by grade and extent of disease. The levels of nerve sparing are categorized as lateral prostatic fascia nerve sparing, traditional or wide.
The technique of lateral prostatic fascia nerve sparing has shown an improvement in recovery of sexual function after RARP 21 and thus can be performed in men with good preoperative sexual function if the following inclusion criteria are met: PSA < 10, primary Gleason score of 3, no ipsilateral nodule, and <50% of any core positive for cancer. If this is not the case, a less extensive traditional postero-lateral nerve sparing is usually performed, and where disease is reported as high grade and/or extensive volume, a wider resection is typically performed.
In any one of these planes, excess thermal spread during dissection of the NVB can affect potency in men after RARP. 10. The flexible fiber was used in this study with the aim of enhancing accuracy of dissection of the NVB using novel delivery of this CO2 laser energy. The current study represents, to the authors' knowledge, the first series to evaluate the feasibility of this.
The benefits of using the flexible CO2 laser fiber are as follows: it was safe to use and easily manipulated between bedside and console surgeon. Soft tissue cutting was precise, stemming from its ready absorption in water. 22 –24 The fiber was very effective in establishing the plane of dissection between the prostatic capsule and NVB, with subsequent meticulous dissection of the NVB and clear identification of appropriate fascial layers as the plane was developed in an antegrade fashion.
Use of this CO2 laser may better facilitate nerve preservation than the standard noncautery technique. We hypothesize that use of cold tools may cause some mechanical trauma, and bleeding could lead to challenges in observing the plane of dissection. In addition, blunt dissection to find prostatic fascial planes can be traumatic to nerve tissue. Using the CO2 laser offers potential benefits on these aspects, with its no-touch nature and limited hemostatic capabilities.
Visual examination indicated that the thermal footprint of the laser was small, with minimal visual thermal spread during the nerve sparing part of the procedure. Histological studies previously demonstrating minimal thermal spread in various animal models would suggest that this visual observation was accurate.
Use of protective eyewear is recommended while using any laser. However, certain conditions of a standard laparoscopic procedure, as well as inherent properties of the CO2 laser, when combined with a fiber-based delivery system, provide a wide margin of safety in such use. Therefore, in an abdominal laparoscopy setting it is not necessary, and we do not wear protective eyewear. However, this remains a hospital policy issue and at the institution's discretion.
There were a number of limitations in its use. Initially, the fragile fiber was damaged by robotic graspers and thus required modification with the addition of the protective sleeved fiber. Second, because the fiber is not yet integrated into the robotic instrument, it requires feeding through one of the laparoscopic ports by the bedside assistant. Further, the flexible fiber is not yet jointed at its tip. These two factors mean that, in its current form, optimum angulation of the fiber with respect to the NVB can be difficult for the console surgeon who is required to stabilize the fiber using both robotic arms. The console surgeon cannot easily manipulate the fiber independently, requiring the assistance of the bedside surgeon to control how far the fiber is projected into the pelvic cavity. Although the laser did provide extremely accurate dissection, it was unable to serve as an adequate means of coagulation in larger vessels.
Mean reported operating time was 165.9 minutes, which is not significantly different from our usual time of 161.4 minutes. Mean estimated blood loss of 124 mL was also not significantly different compared with blood loss when only conventional techniques (hemoclips and standard monopolar or bipolar diathermy) were used.
From a functional standpoint, the early urinary continence results were highly encouraging, with zero pad usage in 7 out of 10 patients (70%) by 6 weeks after surgery, and 9 out of 10 patients (90%) at 3 months. We have previously reported our continence rates to be 50%, 80%, and 92% at 6 weeks, 3 months, and 8 months, respectively. Although this is a small case series with numerous confounding factors, it is extremely encouraging that we found our early continence rates to be higher than normal when using the laser.
Owing to the recent experience with the OmniGuide CO2 laser system, meaningful potency results (assumed to be a minimum of 6 months) have yet to be established. However, we felt it appropriate that a feasibility study be performed early so that preliminary results could be shared with the wider urological community. We felt that the early continence results were promising, though certainly recognize that further data are required to comment on efficacy and clinical value. With our on-going data collection, we hope to report potency results after appropriate follow-up time has lapsed.
It is also too early to determine the oncological safety of this nerve sparing approach. However, no patients were upstaged to T3 disease. All patients had negative surgical margins on final inked pathological specimens. We followed anatomical principles of nerve sparing, and therefore do not believe that we increased the risk of margins status.
The CO2 laser generator (capital equipment) is significantly less expensive than other operating room lasers, and currently retails at $72,000 versus $120,000/$150,000 for line-of-sight and visible light lasers. This is because the CO2 laser uses a cheap, abundant gain medium (CO2 gas), which is also easier to maintain than solid-state lasers. The technological platform used to manufacture BeamPath photonic bandgap fibers (single-use) is an inherently scalable one—it uses a combination of optical processing principles with semiconductor level tolerances. This technology is currently priced at a premium to traditional solid-state optical fibers, but not a level that would preclude its use for high-value applications.
Conclusions
This feasibility study confirms safe and easy use of the flexible CO2 laser fiber to facilitate identification of fascial layers and enhanced accuracy of dissection of the NVB during nerve sparing RARP. Although the initial results are promising, further technical modifications are required to optimize the use of the fiber in this setting.
Long-term follow-up is necessary to determine the efficacy of this technology versus conventional techniques on the NVB. Larger studies are currently in progress to determine if use of the flexible CO2 laser fiber results in improvements in functional outcomes with regard to return of sexual potency after RARP. However, only a randomized trial can control for the many known and unknown confounding factors that can affect long-term oncological and functional outcomes.
Footnotes
Disclosure Statement
No competing financial interests exist.