
Abstract
Purpose:
To assess the effect of surgeon experience and technical modifications on functional and oncologic outcomes after robot-assisted laparoscopic prostatectomy (RALP).
Patients and Methods:
Data were available for 1181 of 1420 consecutive patients undergoing RALP by a single surgeon (DBS). Three techniques were evaluated. The “initial” technique included incision of the lateral endopelvic fascia, suture ligation of the dorsal venous complex (DVC), and anterior tennis-racquet bladder neck reconstruction (n = 590 procedures). The “intermediate” technique included a modified “curtain” nerve-sparing technique and incision of the DVC without previous ligation (n = 170). The “current” technique uses a posterior tennis-racquet bladder neck reconstruction (n = 421). Outcomes included continence and potency recovery and the presence of pT2 surgical margins assessed in continuous fashion. Validated questionnaires were used to assess baseline and postoperative functional outcomes.
Results:
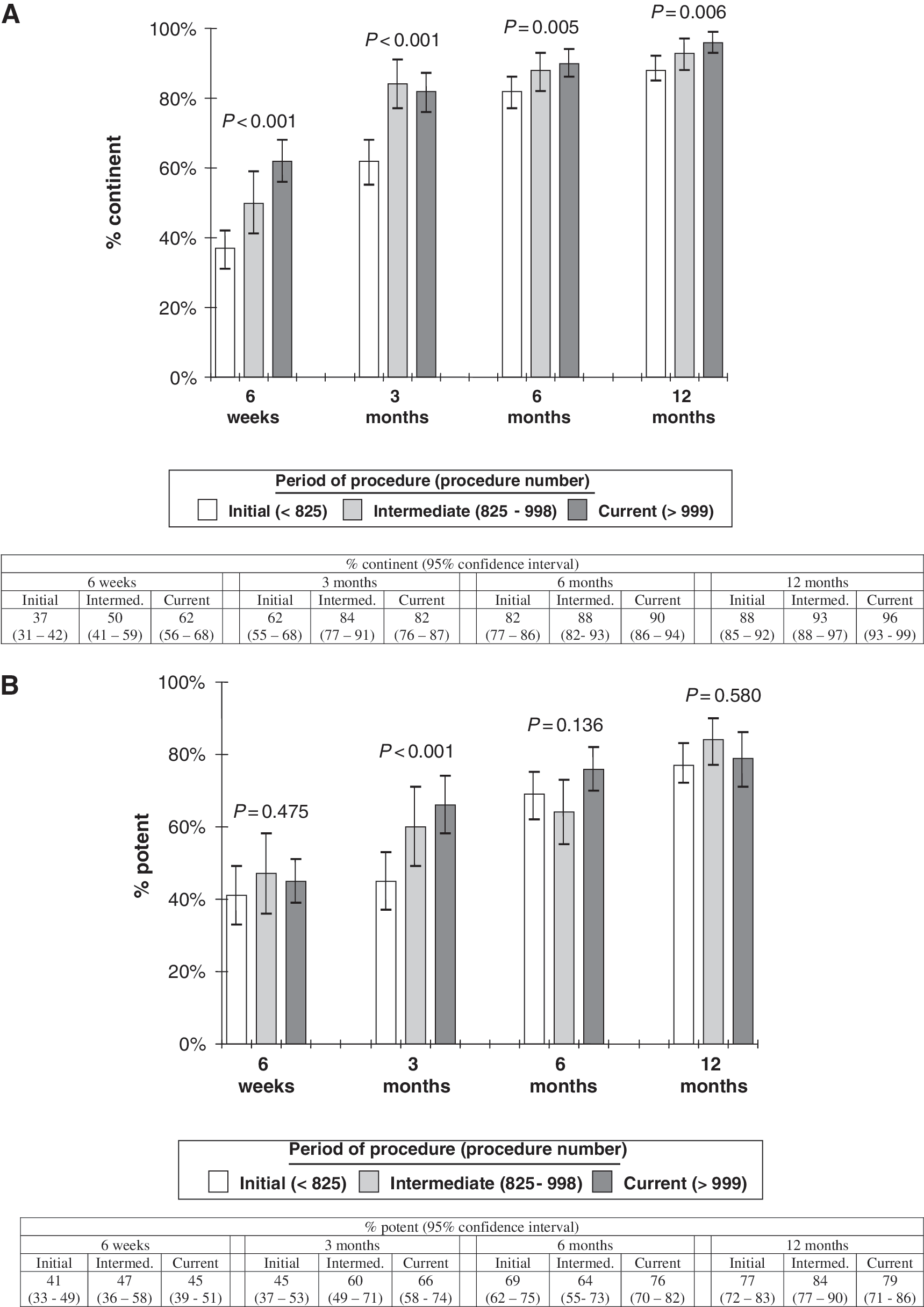
Continence rates improved between techniques at all evaluated time points, with 1-year continence rates of 88%, 93%, and 96% in the initial, intermediate, and current technique groups, respectively (Ptrend <0.001). One-year potency rates, however, remained similar among the groups, with rates of 77%, 84%, and 79%, respectively (P = 0.58). pT2 margin rates decreased continuously during the initial technique period, followed by a transient worsening of margin rates during the intermediate time period and a subsequent decrease during the period when the current technique was used.
Conclusions:
Increased experience with robot-assisted prostatectomy resulted in improvements in oncologic and functional outcomes. Modifications to robot-assisted prostatectomy techniques may aid in this improvement but are also associated with transient worsening of outcomes during the learning curve of the new technique.
Introduction
To assess whether changes in outcomes are a function of surgeon experience vs technique modifications, we evaluated the change in oncologic and functional outcomes after RALP in two ways: As a function of the number of procedures performed and as a function of “procedural eras.” A steady, continuous improvement in outcomes over the number of procedures performed would suggest that a prolonged learning curve of technical refinement occurs. In contrast, improvements in outcomes followed by a plateau after major procedural modifications would suggest that a change in technique is responsible for the improvements. A third alternative is that some technical modifications are associated with a new learning curve and that outcomes are transiently worse before improvements become apparent.
We evaluated this hypothesis in the setting of more than 1100 procedures conducted by a single, high-volume robotic surgeon. Using a single surgeon and a standardized technique minimizes the variability of surgeon-dependent variables. With previous training in both pure laparoscopic and open radical prostatectomy, this surgeon's robotic learning curve should not have been affected by a need to relearn the surgical anatomy from a laparoscopic perspective.
Patients and Methods
A prospective database approved by the Institutional Review Board that comprised all patients undergoing RALP by a single surgeon is maintained by the departmental research staff. Patients who underwent RALP between January 2003 and August 2009 formed the base population for the current analyses (n = 1420). Data for 239 patients, all of whom were in the “initial” technique group, were incomplete and were excluded from the analyses. After these exclusions, completed data were available for 1181 patients. Thus, the study was a retrospective analysis of a prospective database.
Functional outcomes and prostate-specific antigen (PSA) levels were collected at baseline, 6 weeks, and then every 3 months for the first year after surgery using International Prostate Symptom Scores (IPSS) and Sexual Health Inventory for Men (SHIM) scores. For the purpose of our analysis, we used the “social” continence definition—the use of either no pads or one security pad daily—which has been demonstrated to correlate well with urinary quality of life. 4 We also conducted a subanalysis of “strict” continence—the use of zero pads each day—at 12 month follow-up. Potency was defined as a SHIM score ≥16 in patients who were preoperatively potent (SHIM ≥16). A postoperative PSA level >0.2 ng/mL at least 6 weeks after surgery was considered a biochemical recurrence.
The prostate specimen was sectioned in four quadrants and mounted in standard fashion. Volume of cancer was estimated based on the percentage of slides containing tumor (the positive-block ratio). 5 Tumor at the inked resection margin was considered a positive surgical margin (PSM). PSMs were dichotomized into “focal” or “extensive” if the length of the margin was less than or greater than 2 mm, respectively. The site of positive margins was also recorded and analyzed. Operative time was the length of time from skin incision to skin closure.
Surgical technique
The surgical technique evolved after two discrete modifications in the procedure. The patients were thus categorized into three groupings based on the procedure they received: Standard RALP with anterior tennis-racquet bladder neck reconstruction (initial technique), modified “curtain” nerve sparing and omission of dorsal venous complex (DVC) stitch (intermediate technique), and posterior bladder neck reconstruction (current technique). A graphic summary of the different techniques is provided in Table 1.
1. Initial technique: Standard RALP
This procedure was performed from the start of our robotic experience in January 2003 through December of 2007. A standard transperitoneal RALP was performed. 6,7 The endopelvic fascia was opened widely, lateral to the prostate. The DVC was ligated with an 0 prolene suture in a figure-of-eight fashion. No concerted effort was made to spare the bladder neck. Seminal vesicles were approached superiorly during posterior bladder neck dissection. Vascular pedicles were controlled with bipolar cautery alone. When indicated, nerve sparing was performed in an interfascial plane in antegrade fashion. Bladder neck reconstruction was performed on all patients via an anterior tennis-racquet repair to achieve a diameter of approximately 24F.
2. Intermediate technique: Modified curtain nerve sparing, omission of DVC stitch
We modified our technique in January 2008 to move the incision of the endopelvic fascia medially onto the anterior surface of the prostate. This is a procedure that has been described alternately as the “high anterior release.” 8 the “veil of Aphrodite,” 9,10 or the curtain technique. 11 In contrast to several of these techniques, our nerve sparing is performed in an interfascial plane, as opposed to an intrafascial one. The DVC is not ligated but rather cut with cold scissors just before removal of the specimen. It is subsequently suture ligated with 3-0 polyglactin suture in a running fashion. Nerve sparing is performed exclusively in an athermal manner with blunt dissection with rounded-tip scissors. The vascular pedicles were controlled by robotically applied Hem-o-lok® clips (Weck Closure Systems, Research Triangle Park, NC).
3. Current technique: Posterior bladder neck reconstruction
In June of 2008, we made the last modification: A transition from an anterior to a posterior tennis-racquet bladder neck reconstruction, with a narrower diameter of 18F. The remainder of the procedure remained as in the intermediate technique.
Statistical analysis
Data were analyzed with SAS version 9.2 (SAS Institute, Cary, NC) and R version 2.8 (R Foundation for Statistical Computing, Vienna, Austria). Patient characteristics were calculated as means and percentages for the overall population and by procedural era. The percent of patients with continence and potency recovery, separately, was calculated at 6 weeks and 3, 6, and 12 months after surgery for each era. These percentages were calculated including only those who were continent and potent before surgery. The statistical significance of trends in patient characteristics and outcomes across eras was assessed, modeling era as a three level ordinal variable, using analysis of variance.
To explore the effect of surgical experience on pT2 margins, we used restricted quadratic splines with knots at the 10th, 50th, and 90th percentiles of surgeries (ie, 95, 475, and 855 patients, respectively). We chose to analyze margins in a continuous fashion, restricted to patients with organ-confined (stage pT2) cancer (n = 952), because PSMs in these patients are more representative of surgical technique, as opposed to aggressive disease.
We chose to plot the x-axis based on the total number of procedures performed by the surgeon, because we believe his experience is a function of the total number of cases performed, not just procedures for pT2 tumors. Therefore, the x-axis extends to 1420 and not 952.
Results
The initial technique was performed on 590 patients, while 170 and 421 had the intermediate and current technique, respectively. Baseline demographic and pathologic results are listed in Table 2. Mean PSA level, nerve-sparing status, prostate weight, and Gleason score were similar for the three groups. The current group, however, had significantly more advanced disease than the earlier cohorts. The presence of extraprostatic extension and seminal vesicle invasion was more common in the recent groups. There was a statistically significant downward trend in extensive PSM from 8.5% to 4.3%, although this was countered by an increase in focal positive margins.
Numbers in table are mean (standard deviation) or percentage.
PSA = prostate-specific antigen.
Significant improvements in continence were seen at all time points when analyzed by procedural era, with 12-month social continence rates of 89%, 93%, and 96% in patients undergoing the initial, intermediate, and current techniques, respectively (Fig. 1A, P = 0.006). Strict (pad-free) continence at 12 months also showed a similar trend, occurring in 76%, 80%, and 83% of the three groups, respectively, although this did not achieve statistical significance (P = 0.23). Technical changes had less of an effect on potency; significant improvements with the more recent techniques were present only at 3 months. Progressive improvements in potency rates, however, were seen at each successive time point in all procedural eras (Fig. 1B).
(
The odds ratio for having PSM in patients with pT2 disease by procedural number is depicted in Figure 2. The overall curve is sinusoidal in shape. During the initial technique period, the odds ratio for PSM decreases continuously with surgeon experience. After the first procedural modification, the odds ratio for having PSM increased for the next 200 patients. This period of increasing rates of PSM includes both surgical technique changes. The odds for PSM decreased continuously with surgeon experience after the adoption of the current technique. A detailed analysis of pT2 surgical margins by location and extent is presented in Table 3. No significant differences were noted in the locations of the margins between technique groups.

Restricted quadratic spline showing the odds ratio for having positive surgical margins by procedure number performed. Analysis is limited to patients with pT2 stage. Solid line represents odds ratio, shaded area represents the 95% confidence interval. Dashed lines represent the timing for the two discrete technique changes as described in the Methods section.
Discussion
Since its initial description in 2001, numerous modifications have been reported to RALP. Included among these are a new form of nerve sparing, 10 a urethral suspension stitch, 12 posterior (and to a lesser extent, anterior) fascial reconstruction, 13 the sparing of the lateral prostatic fascia, 9 abandonment of the DVC stitch, 14 and the avoidance of any thermal energy during nerve sparing. 15 Each of these maneuvers has a theoretical basis for improving postoperative outcomes, and each has been reported to have a positive effect on outcomes via lower margin rates, better functional outcomes, or a faster return to continence and potency.
Improvements in outcomes after technique changes, however, have been evaluated in consecutive cohort studies, where improvements in outcomes may have been because of continued surgeon improvement over time, not the procedural change itself. The only technique change that was evaluated in a prospective, randomized study—the posterior fascial plate reconstruction—was not found to provide a significant benefit. 16
In the current study, we report the results from a large cohort study of consecutive patients undergoing RALP. A clear improvement in outcomes was present with increasing surgeon experience. This may partly be because of continuous improvement and small modifications made after the frequent assessment of our technique through review of videotaped procedures. It is more likely, however, that the improvement is related to the major technical modifications as described above. Although a learning curve was present after the adoption of new techniques, eventually these techniques appeared to result in better outcomes.
As in previous studies, 1 we chose to use surgical margin status as a continuous metric to assess our learning curve. It is the only surgeon-dependent variable that impacts prostate cancer-free survival, the most critical outcome of radical prostatectomy. We chose to use margin status in pT2 patients to help restrict our analysis to PSMs related to surgical technique, not tumor biology (as in pT3 tumors). We also used a validated questionnaire to objectively measure potency (we only used subjective measures for measuring continence because the IPSS does not have an explicit continence component).
As expected, outcomes improved as surgeon experience increased. Rates of PSM decreased; continence and potency were regained more rapidly and in higher percentages of patients. More interesting was the change in the proportion of patients with PSM associated with surgical case number. Initially, a steady continuous decrease was found in the odds for PSM until the first technique change. At that time, there was a marked upward inflection, as the PSM rates increased. After approximately 200 cases, the rates reached a plateau and then decreased again. This decrease occurred around the time of the second procedural modification, but considering that the modification involved only the bladder neck reconstruction, it is unlikely to have caused the reduction in PSM rates.
Why did such a transient increase in PSM rates occur? The tumors were of larger volume in the later groups, which is a plausible cause for a higher PSM. Another possibility is that cutting an unligated DVC may have resulted in bleeding that obscured the correct dissection plane at the apex. The rates of apical PSMs, however, did not increase after the adoption of this technique. The most likely reason for the transient spike in positive margins was the new type of nerve sparing. The curtain-type nerve-sparing technique needs precise dissection and an experienced eye to recognize the way in which tissue planes interact to avoid PSM and alert the surgeon to the presence of capsular incision. Such skills and visual recognition require a level of experience that likely takes several hundred cases to develop.
This demonstrates a second learning curve related to the adoption of a new and technically demanding technique. Although this second learning curve applied to PSM, it did not appear to affect functional outcomes, which improved with surgeon experience without a new learning curve for the adoption of new techniques. It is possible, however, that a trend in worsening functional outcomes during the second learning curve was obscured by the size of the groups, as this was not measured in continuous fashion.
It is important to recognize that major technical procedural changes can result in a transient worsening of outcomes even among experienced surgeons. While such a change may ultimately lead to improved outcomes, there will be a period of transition during which outcomes might suffer. We report this not to discourage experienced surgeons from changing their technique, but to inform them before undertaking such changes that outcomes may temporarily worsen. These findings suggest that consideration should be given toward notifying patients when a surgeon is making significant modifications to technique.
The current study needs to be considered within the context of its limitations. Most notably, the study was retrospective in nature and limited to procedures performed by a single surgeon. It is a consecutive cohort study, the weaknesses of which were discussed above. Given the limitations of such a study, we are not attempting to make generalizations regarding the efficacy of the individual modifications that we chose to make. Such a comparison can only be addressed by a randomized controlled trial, which we did not perform. Instead, we wanted to assess the role of the learning process itself. This is best studied in a large single-surgeon cohort, because it eliminates intersurgeon variability. Furthermore, by studying the robotic series of a surgeon with previous experience with laparoscopic prostatectomy, the initial robotic learning curve should be minimal.
Conclusion
Increased surgeon experience with RALP results in improvements in oncologic and functional outcomes. Modifications to the robot-assisted prostatectomy technique likely aid in this improvement, especially those related to the nerve-sparing technique. Such modifications, however, are also associated with transient worsening of outcomes during the learning curve of the new technique. Such secondary learning curves may be responsible for the prolonged learning curve seen in laparoscopic radical prostatectomy.
Footnotes
Disclosure Statement
This research was supported by a small (<$25,000) unrestricted research grant from Intuitive Surgical, Inc. No investigators or their close family members have personal financial interests in Intuitive Surgical or any other financial conflicts of interest.