
Abstract
Objectives:
The objective of this study was to describe our experience with laparoscopic simultaneous bilateral dismembered pyeloplasty in two pediatric cases by using three midline ports.
Methods:
A 5-year-old boy and a 5-month-old male infant with bilateral ureteropelvic junction obstruction underwent bilateral laparoscopic transperitoneal dismembered pyeloplasty. A 10-mm trocar was placed through the umbilicus, and two 5-mm trocars were also placed in the midline superior and inferior to the umbilicus. On the left side, dismembered pyeloplasty was performed through a transmesocolic approach. Double-J ureteral stent was inserted through one of the trocars on both sides.
Results:
The postoperative period was uneventful. Patients were discharged on postoperative days 4 and 5. Oral feeding was tolerated on the first postoperative day. In a 6-month follow-up period, excretory urography and renal scan showed resolution of obstruction.
Conclusions:
Laparoscopic dismembered pyeloplasty can be performed in a single session for pediatric patients with bilateral ureteropelvic junction obstruction. This can obviate the need for two sessions of anesthesia induction and intubation. However, more studies with large number of patients are needed to confirm this result.
Introduction
Materials and Methods
Case 1
The case was a 5-year-old boy with a history of episodic abdominal pain for a year. Abdominopelvic ultrasonography revealed bilateral severe hydronephrosis with anteroposterior pelvis diameter of 36.8 and 40.6 mm on the right and left side, respectively. Excretory urography disclosed severe bilateral pelvicalicectasis without opacification of ureters at 2 hours after contrast injection. A nuclide furosemide renogram showed severe delay in cortical transit time and washout on both sides. Voiding cystourethrography revealed no vesicoureteral reflux. The patient was scheduled for bilateral laparoscopic dismembered pyeloplasty in a single session.
Case 2
A 5-month-old male infant was presented because of prenatal bilateral severe hydronephrosis. Postnatal ultrasonography disclosed persistent bilateral severe hydronephrosis. The patient had an episode of febrile urinary tract infection. On voiding cystourethrography, there was no vesicoureteral reflux. Excretory urography showed severe bilateral hydronephrosis (Fig. 1). Diuretic renogram revealed delayed washout confirming bilateral severe UPJ obstruction accompanied by decreased renal function.

Excretory urograph showing bilateral severe hydronephrosis.
Technique
After induction of general anesthesia and placing a urethral catheter, the patient was placed in a right lateral decubitus position by adequate padding. A 10-mm trocar was placed through the umbilicus via an open approach. The second and third 5-mm trocars were placed in the midline ∼10 cm superior and inferior to the umbilicus, respectively (Fig. 2). The white line of Toldt was incised and colon was mobilized. After identifying the ureter and renal pelvis, classic dismembered pyeloplasty was performed (Fig. 2). A Double-J ureteral stent was inserted through one of the trocars (Fig. 2).

(
To perform pyeloplasty for the contralateral kidney, the patient was placed in a left lateral decubitus position. Using the same trocar arrangement, dismembered pyeloplasty was performed on the left UPJ through a transmesocolic approach. A penrose drain was placed through the inferior port site.
Results
The postoperative period was uneventful. Operative time was 320 and 350 minutes in cases 1 and 2, respectively. Patients tolerated oral feeding well on postoperative day 1. The urethral catheter was removed, and the patient was discharged on postoperative days 4 and 5, respectively. Double-J stents were removed at 8 weeks after the operation, with a 2-day interval.
During a 6-month follow-up period, patients had neither abdominal pain nor urinary tract infection. Ultrasonography demonstrated marked improvement of bilateral hydronephrosis. Excretory urography and renal scan revealed resolution of the obstruction (Fig. 3).
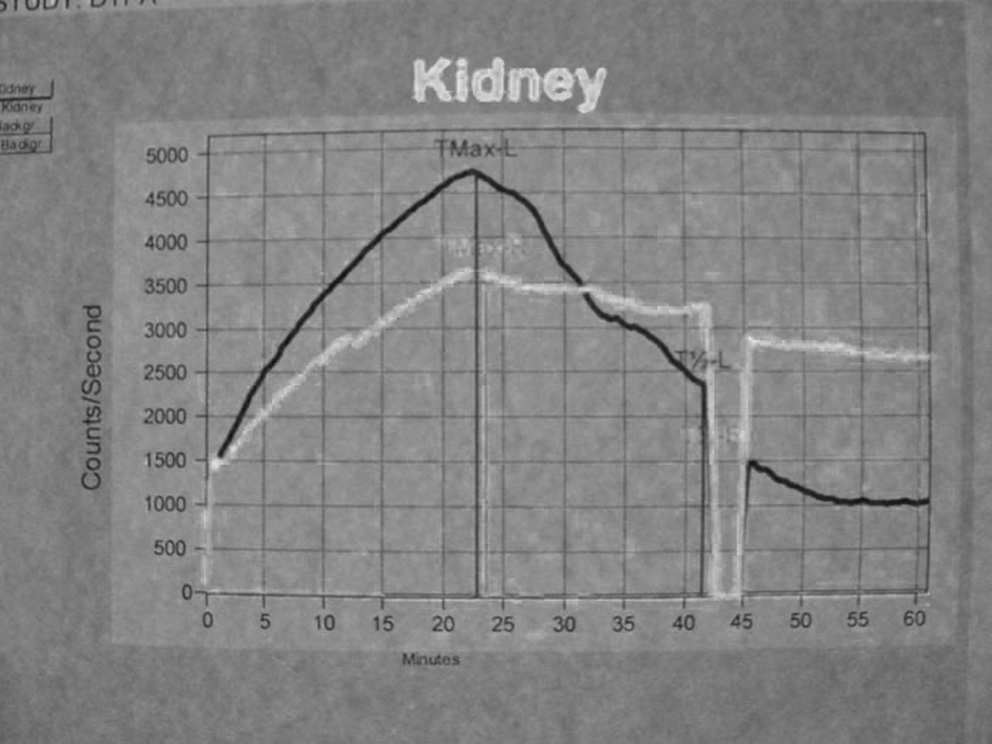
Postoperative excretory renography curve showing resolution of obstruction immediately after Lasix injection.
Discussion
Several reports described laparoscopic pyeloplasty in the pediatric population, with success rates comparable to those of open pyeloplasty. 6,7 Provet and Hannah 2 described synchronous bilateral open pyeloplasty to be safe and cost effective. They reported on 15 children who underwent bilateral dismembered pyeloplasty or ureterocalicostomy with excellent functional and anatomic results. They concluded that bilateral pyeloplasty is an acceptable alternative to staged procedures for bilateral UPJ obstruction.
Synchronous bilateral laparoscopic pyeloplasty was first reported in two pediatric cases by Shcwab and Casale. 5 They used a transperitoneal four-port approach, two ports in the midline and one on each side for each kidney. They reported resolution of obstruction in both patients without any complication. Freilich et al 8 reported concurrent bilateral robot-assisted laparoscopic pyeloplasty in five cases. They also used a four-port approach and concluded that simultaneous bilateral laparoscopic pyeloplasty is feasible and safe. Although a one-stage procedure may take longer if compared with each stage of the staged procedure, it obviates the need for two sessions of anesthesia induction and intubations. Moreover, the scar tissue developed in the place of trocar insertion might make the second procedure more challenging.
To our knowledge, this is the second study on nonrobotic bilateral laparoscopic pyeloplasty, in which three midline ports have been used for the first time. Placing three ports in the midline precluded the need for inserting an extra lateral port on each side. On the basis of our routine technique in unilateral laparoscopic pyeloplasty, 9 we placed the Double-J stent laparoscopically by passing the stent from one of the ports. This eliminates initial cystoscopic stent insertion in lithotomy position, which could be time consuming. With increased experience in laparoscopic techniques, patients with less-frequent situations could benefit from the advantages of minimally invasive procedures. Although more studies with large number of patients are required, synchronous bilateral laparoscopic pyeloplasty in pediatric cases seems to be safe and feasible.
Footnotes
Disclosure Statement
No competing financial interests exist.