
Abstract
Introduction:
In the era of prostate-specific antigen screening and frequent cross-sectional abdominal imaging, concurrent prostate cancer and renal masses are being identified and treated. Minimizing patient morbidity and cost by avoiding separate surgical procedures is advantageous, provided technical feasibility, and safety data. Our goal was to assess the feasibility and safety of single-setting robotic renal surgery and prostatectomy. We present our initial experience.
Purpose:
To assess the feasibility and safety of single-setting concurrent robot-assisted renal surgery and radical prostatectomy utilizing the same port access scheme.
Patients and Methods:
From February 2009 to June 2009, we performed single-setting concurrent robot-assisted radical nephrectomy/partial nephrectomy and radical prostatectomy on two patients with synchronous kidney tumors and prostate cancer. Identical port sites were used during both aspects of the procedure with the exception of one additional port during prostatectomy. Prostate cancer clinical stage and Gleason scores were T1c and 6 and T2a and 7, respectively. Corresponding renal tumors were 5 cm, respectively.
Results:
Both operations were performed, with no conversion to open surgery. There were no intraoperative complications and the postoperative course was uneventful in both patients. Discharge was on postoperative day 2 and 3, respectively. Patient 2 had an episode of delayed bleeding on postoperative day 9, treated by selective angio-embolization. Mean operative time for nephrectomy and prostatectomy (135 and 139 minutes, respectively) and estimated blood loss (75 and 100 mL, respectively) were reasonable. We began with the renal portion utilizing a lateral decubitus position before re-positioning into the lithotomy position for the prostatic portion. Clamping time was 34 minutes during partial nephrectomy.
Conclusion:
Single-setting robotic radical/partial nephrectomy and radical prostatectomy is technically feasible and safe in properly selected patients who present with synchronous primary renal and prostate malignancies.
Introduction
Patients and Methods
From February 2009 to June 2009, we performed single-setting concurrent robot-assisted radical nephrectomy/partial nephrectomy concurrent with radical prostatectomy on two patients with synchronous kidney tumors and prostate cancer. Patient attributes were as follows. Patient 1 was a 49-year-old man with a history of hypertension and who was found to have clinical stage T1c, Gleason score 3 + 3 = 6 prostate cancer with a PSA of 7 and concurrent 5-cm right renal mass. Of note, this patient had a preoperative hematocrit of 55%, which was evaluated and felt to be likely caused by a paraneoplastic secretion of erythropoietin. Patient 2 was a 72- year-old man with a history of diabetes and hypertension with clinical stage T2a, Gleason score 3 + 4 = 7 prostate cancer with a PSA of 29.1 and synchronous 3-cm right renal mass. Bone scan was negative, and no suspicion for lymph node spread or metastatic disease was present on preoperative cross-sectional imaging (Table 1).
BMI = body mass index; ASA = American Society of Anesthesiologists; PSA = prostate-specific antigen; DM = diabetes mellitus; HTN = hypertension.
We have previously reported our surgical technique for concomitant radical nephrectomy and prostatectomy using the DaVinci® Robotic System (Intuitive Surgical, Sunnyvale, CA). 14 Briefly, the surgery is begun on the renal unit and then proceeds to the prostatectomy portion of the case. Initially, the patients are positioned in a lateral decubitus position at an angle of ∼70° without table flexion. Veress needle access is used to obtain pneumoperitoneum and to introduce the camera before inserting three additional robotic ports (Fig. 1A), one 10–12-mm port, and a 5-mm port for a total of six ports. Radical nephrectomy is performed in the standard fashion using the Ligasure® bipolar cutting cautery device (Valley Lab, Boulder, CO) to cut through the ureter and a universal Endo-GIA® stapler (Covidien, Boulder, CO) across the hilum for control of the major vessels. The kidney is then put inside an endocatch bag and left inside the abdomen. The ports are then all removed and the ports sites covered with sterile adhesive tape. There is minimal variation from the above procedure and the partial nephrectomy performed on patient 2, with the notable addition of hilar clamping and primary repair of the collecting system and closure of the renal capsule. This is all performed robotically.
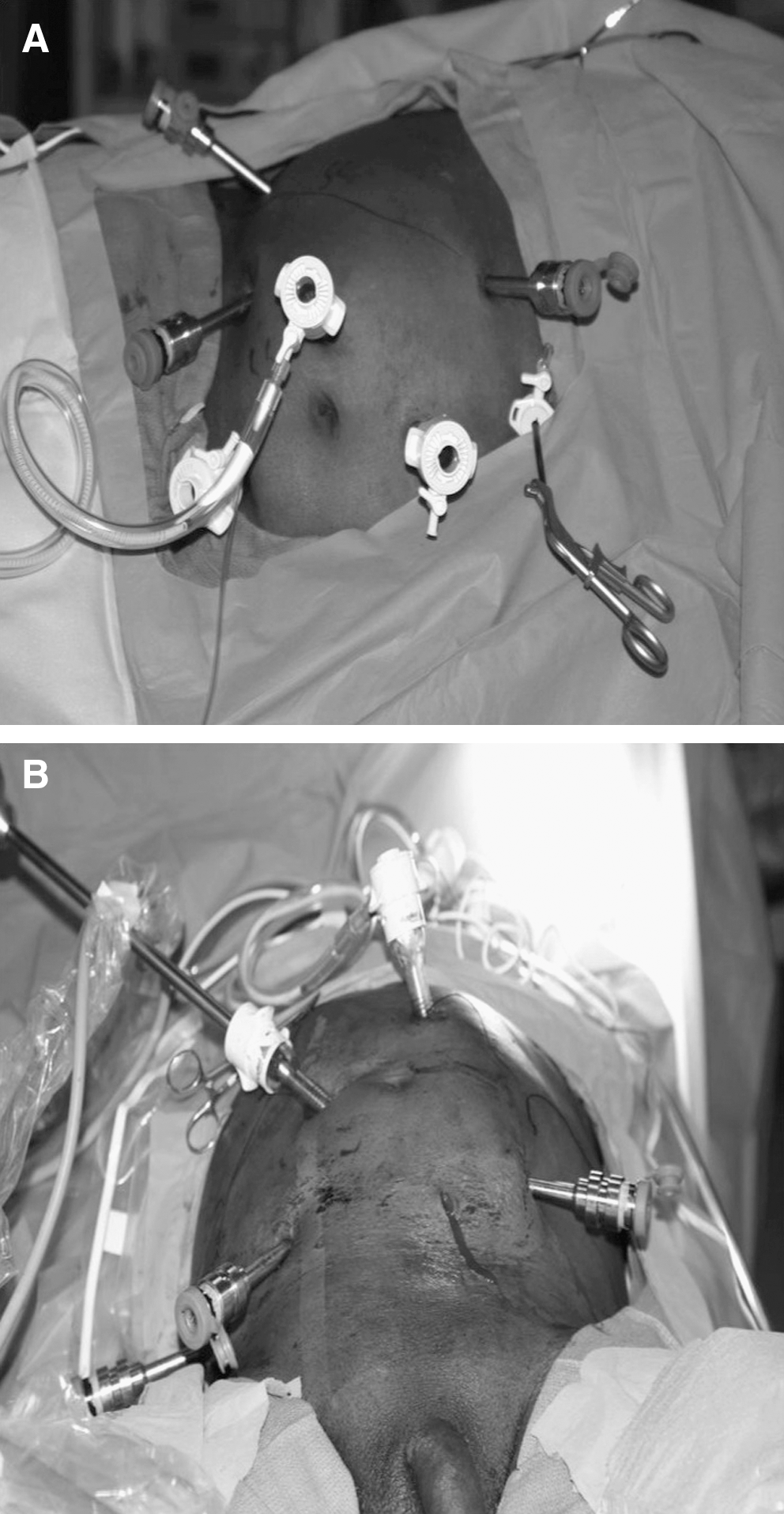
Port placement during nephrectomy (
After nephrectomy, the patient is then re-positioned in a steep lithotomy position and the abdomen and the genitalia prepped and draped. We re-access the same camera, assistant, and robotic ports used for the nephrectomy portion. The camera port used in the nephrectomy part is used as an assistant port (Fig. 2). Likewise, the assistant port in the nephrectomy part is used as a camera port in the prostatectomy portion of the case. We place only one new port on the left side of the pelvis to accommodate the robotic arm on the left (Fig. 1B). The prostatectomy portion is then performed in the standard manner. The prostate specimen is put into a second Endocatch® bag and the robot undocked. The incision of the lowermost port is extended to a 3-cm incision, and the prostate is removed first. To keep the incision small, the edges of the renal specimen in its own Endocatch bag are brought outside the incision (Fig. 3A, B). Then, we mechanically morcellate the kidney using a curved clamp forceps (morcellation of partial nephrectomy specimen is not required). A closed suction drain is inserted at the conclusion of the case (see Fig. 4).
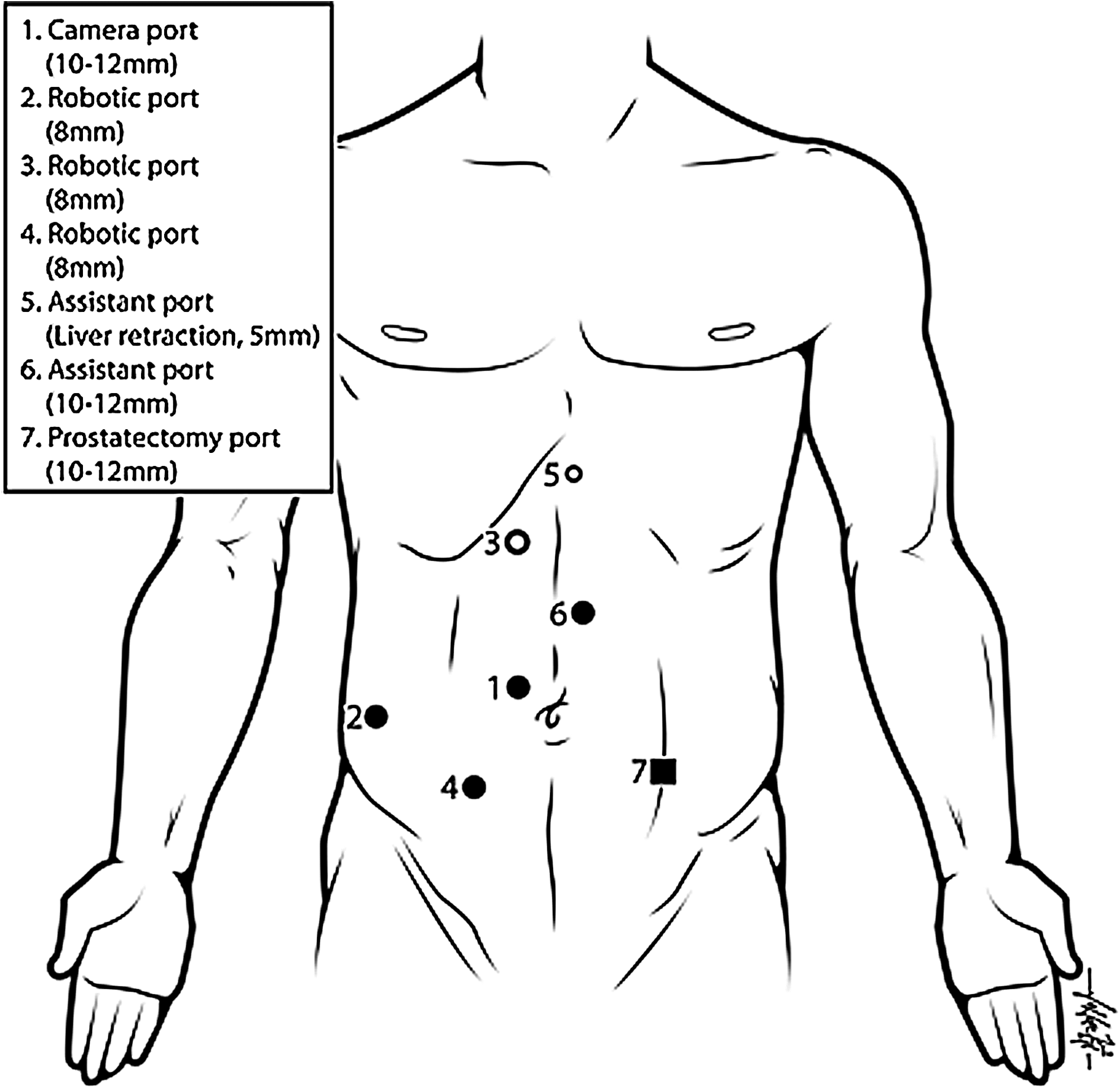
Schematic of port placements during nephrectomy (circles) and additional prostatectomy port (square). Drawing by Thomas Nowacki.

Specimen extraction (
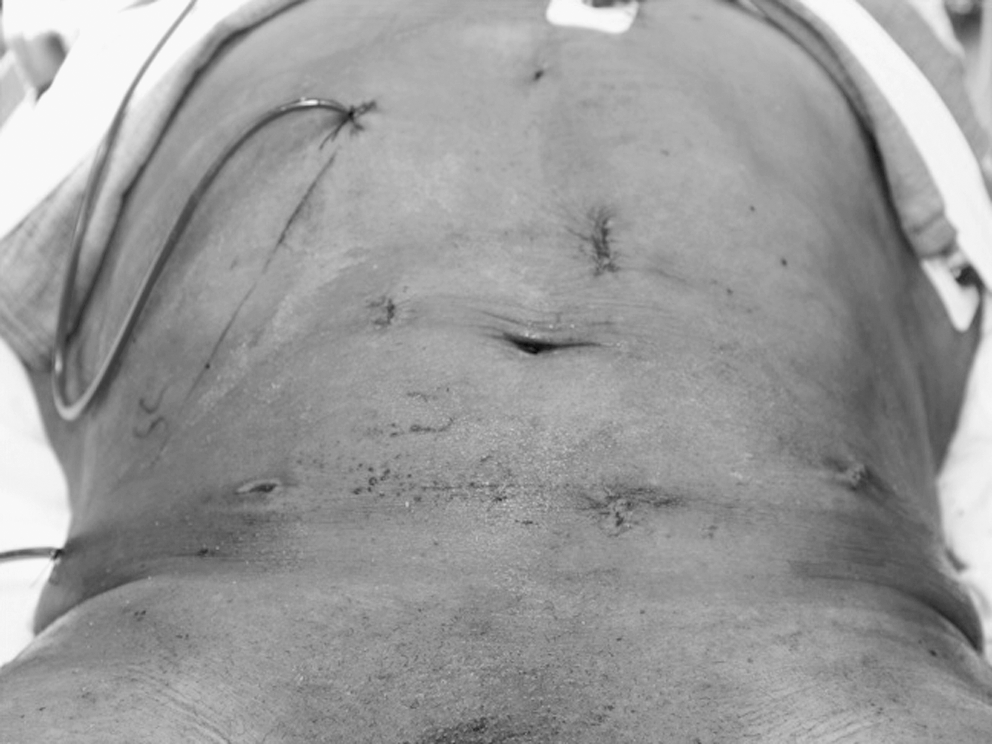
Postoperative incision appearance and drain placement.
Results
There were no intraoperative complications and neither case required conversion to an open procedure. Identical port placements were used for both portions of both cases, except for the planned addition of one further port for the prostatectomy portion in both cases. Patient 1 was discharged home on postoperative day 3 and patient 2 was discharged home on postoperative day 2. Both patients passed their trials of void and had uneventful recovery. Patient 2 did have bleeding necessitating angio-embolization on postoperative day 9.
The mean estimated blood loss for the renal portion of the surgeries was 100 mL and for the prostatectomy portion was 100 mL. Mean surgical time for the renal surgery was 135 minutes. Hilar clamping time was 34 minutes in the partial nephrectomy case. Mean robotic surgical time for prostatectomy portion was 139 minutes (Table 2).
EBL = estimated blood loss.
Pathological analysis postoperatively revealed Gleason score 7 (3 + 4) prostate cancer involving 30% of the prostate with negative margins and Fuhrman grade 3 renal cell cancer with negative margins for patient 1. At this time, there is no evidence of recurrence at 6-month follow-up. Pathological characteristics for patient 2 were Gleason score 7 (3 + 4) T3b prostate cancer with negative margins and 3 cm Fuhrman grade 2 renal cell carcinoma with negative margins with no evidence of recurrence. Functionally, creatinine in patient 1 leveled off postoperatively at 1.8 (preoperative 1.2) and in patient 2 at 1.0 (preoperative 1.4) (Table 3).
RCC = renal cell carcinoma; F/U = follow-up.
Discussion
Robot-assisted laparoscopic surgery has been widely incorporated into urologic surgeries, particularly in radical prostatectomies. Nationwide, the majority of prostatectomies are being performed via the robotic approach 8 and utilizing the robotic approach for renal surgery is becoming increasingly common, as safety and feasibility have been reported. 10,12,13 This surgeon (R.M.) routinely performs robot-assisted radical prostatectomies and renal surgeries, including partial nephrectomy.
As noted, we were able to use the same ports for both procedures. The only change was that we added one additional port in the left lower quadrant to accommodate one robotic arm. The two robotic ports placed on the side of the kidney surgery were used with ease for pelvic surgery. The renal camera port and the assistant port were used also in the prostatectomy part. Modifying the placement of the renal camera point into a more medial position was crucial as this maneuver allowed this port to be accessible for usage either as a camera port or as an assistant port when performing the prostatectomy portion. Such an arrangement might be harder to achieve in an obese patient, as all the instruments are usually shifted more laterally in obese patients. In addition, both specimens were extracted from the same incision, which was kept small (3 cm). We feel compelled to also address the issue of morcellation. Previously, this topic has previously been addressed and discussed extensively. The risk of compromising oncological principles by removing the specimen by in a morcellated fashion has not been demonstrated. 15 It is the routine practice of R.M. to offer morcellation as an option that has the advantage of maintaining a small incision.
Incorporating surgical procedures involving multiple organs in one setting is not a revolutionary idea. In fact, within the urologic community, we routinely combine surgical procedures on the vagina, bladder, bowel, ureter, and uterus during such operations as pelvic exenteration, radical cystectomy with diversion, ileal ureters, and surgery for pelvic organ prolapse. Further, during radical cancer surgeries, resecting the tumor can involve surgically violating multiple organs. Until recently, however, there has been little attention directed at the potential for treating multiple surgical disease processes in a single setting. In part, this has been because of the incidence of synchronous disease discovery being low. As mentioned above, this pattern is changing, however. As such, the manner in which we manage this issue of synchronous pathology is evolving. For example, single-setting bilateral hand-assisted laparoscopic partial nephrectomy has recently been reported. 16 To our knowledge, this is the largest series of the emerging technique of concurrent robotic renal and prostatic surgery for malignancies. Although other groups have performed similar surgeries, we are the only group to report the technique of performing this procedure using the identical port placement during both the renal and prostatic portions of the surgical procedure. 5,7 Of note, in the experience of others, as in our own brief experience, thus far the safety of single-setting laparoscopic surgeries has been demonstrated.
Utilizing a single setting for multiple surgical procedures has as potential advantages a decrease in the exposure to anesthesia risk and surgical trauma (e.g., no lysis of adhesions), shorter overall hospitalization and convalescence, and a potential significant financial advantage. Using our approach to port placement, there is the additional advantage of decreased risk of trocar injury by minimizing trocar entry frequency, of improved cosmesis (fewer scars), and potentially less psychological stress on both the patient and family, as well as a decreased loss of productivity by limiting time off of work. The potential disadvantages of this new approach include increased total surgical, and thus anesthesia, time, as well as the potential for higher complication rates or harmful effects of prolonged pneumoperitoneum that may be secondary to increased procedural length. Of note, several investigators have reviewed laparoscopic complications caused by pneumoperitoneum, and duration of pneumoperitoneum seems to cause minimal alterations in pulmonary mechanics and does not affect overall hemodynamic parameters that are only transiently affected during the first 30 minutes of insufflation. 17 –19 One concern is the prolonged elevated intraabdominal pressure, which might affect the function of the remaining kidney. However, we did not believe that to be an issue in our particular case, as the creatinine trended down as we usually expect after a nephrectomy (creatinine was 1.8 upon discharge).
Assuredly, one should mention the importance of both surgical experience with robotic techniques of each portion of the procedure, itself, as well as the importance of patient selection. A prospective patient's overall health condition and body habitus are crucial elements to review before offering this type of procedure. At this junction, we would recommend surgeons proceed with patients with minimal comorbidities, particularly respiratory, as well as those of a more slender body habitus. In the latter case, port positioning might be significantly altered from our scheme as usually the ports are placed more laterally for renal surgery in these patients and might become unusable for the pelvic approach.
Conclusions
Concurrent single-setting surgery for renal and prostatic malignancies using the same port placement is technically feasible in select patients. To date, safety and oncological outcomes seem on par with expectations from each individual portion of the combined procedure were it to be done as a separate surgery. Further investigation into identifying which patients and what other pathological processes might be amenable to this approach is warranted.
Footnotes
Acknowledgment
Thanks to Thomas Nowacki for assistance with illustration.
Disclosure Statement
None of the listed authors have any conflicts of interest to disclose.