
Abstract
Background and Purpose:
Minimally invasive adrenalectomy is the preferred surgical approach for small, benign adrenal neoplasms. Posterior retroperitoneoscopic adrenalectomy is associated with potential surgical advantages. We sought to investigate the feasibility and early outcomes for robot-assisted posterior adrenalectomy, which has not been previously reported.
Patients and Methods:
Patients were selected for adrenalectomy based on standard clinical indications. The study was conducted under a protocol approved by the Institutional Review Board. Patients with adrenal masses larger than 7.0 cm, or with a body mass index (BMI) greater than 40, were excluded. Patient demographics, clinical and pathologic data, operative times, and patient outcomes were collected prospectively.
Results:
Six consecutive patients underwent robot-assisted posterior retroperitoneoscopic adrenalectomy (RAPRA) between June 23, 2009 and January 21, 2010. Five women and one man, ages 45 to 75 years (mean 55.5 years), with a mean BMI of 30, were included. There were three right adrenal tumors and three left adrenal tumors. Mean operative time was 121 minutes with a mean robot time of 57 minutes for the five patients in whom the entire adrenal dissection was performed robotically. There was essentially no morbidity and no mortality.
Conclusion:
This study represents the first report of RAPRA, and demonstrates the feasibility of performing this procedure with good patient outcomes.
Introduction
The posterior retroperitoneoscopic approach has been studied extensively as an alternative surgical method, with reports of excellent results in large series, principally from Europe. 22,23 This technique has been adopted by several expert endocrine surgery centers in the United States and is rapidly gaining in popularity as an alternate approach. Posterior retroperitoneoscopic adrenalectomy (PRA) has purported advantages over transperitoneal laparoscopic adrenalectomy (TLA), including a more direct anatomic approach with need for less dissection and mobilization of associated organs (eg, spleen, pancreas, liver), 24 –26 shorter operative times, 22 –24,26 –29 reduced risk of sequelae from entering the peritoneal cavity such as obstructing adhesions or unrecognized bowel injury, 23,28 advantages for patients who have had multiple previous anterior peritoneal operations, 6,23 and patients with bilateral adrenal pathology. 8,9 Potential disadvantages include surgeon unfamiliarity with a posterior anatomic approach and prolonged learning curve, potential complications of increased capnoretroperitoneoscopic pressures including possible deleterious intraoperative cardiovascular effects, pneumothorax/pneumomediastinum or massive subcutaneous emphysema, as well as other potential but rare complications from the prone positioning, which have not been reported to date.
Except for only a few of these potential advantages or disadvantages, convincing prospective randomized data to answer these questions are currently lacking. Two available randomized prospective studies that compare TLA and PRA show similar good results for both approaches and support the advantages of shortened patient convalescence and reduced trocar site hernias with PRA. 30,31 Experienced surgeons can achieve excellent and generally comparable results from both TLA and PRA, while marginal or significant advantages may be associated with one of these approaches with further study.
Robot-assisted surgical techniques have been successfully applied to an increasingly broad spectrum of surgical procedures, notably in the fields of urologic surgery, gynecologic surgery, cardiothoracic surgery, gastrointestinal surgery, and endocrine surgery. The advent of robot-assisted surgery has contributed to minimally invasive surgery the potential advantages of improved three-dimensional (3D) visualization and magnification of the operative field, improved ability to work with a smaller physical space, markedly improved instrument degrees of freedom, surgeon ergonomics, tremor filtering, and motion scaling. Potential disadvantages of robot-assisted surgery include the markedly more complex instrumentation, setup requirements, requirements for specialized operative support team, increased costs and total operative time, and importantly, a current lack of evidence-based data for equivalent or superior patient outcomes and patient acceptance associated with a robot-assisted approach.
A natural progression in advancing techniques for the minimally invasive removal of adrenal neoplasms is the further study of feasibility, operative costs, and patient outcomes for robot-assisted adrenalectomy. A few previous reports have described the results of robot-assisted TLA. 32 –38 We report our initial experience with robot-assisted posterior retroperitoneoscopic adrenalectomy (RAPRA) in six patients. This study, to our knowledge, is the first report of the development of this technique and systematic analysis of the early results.
Patients and Methods
Patients
The study was conducted at a single institution under a protocol approved by the Institutional Review Board. Beginning in September 2006, all patients who presented with adrenal pathology necessitating surgical excision and appropriate for a minimally invasive approach, based on standard clinical criteria, underwent adrenalectomy by a preferred posterior retroperitoneoscopic approach. In general, patients who were appropriate for this approach had benign, functional, or atypical nonfunctional adrenal neoplasms. Our exclusion criteria for PRA included adrenal masses larger than 7.0 cm and patients with a body mass index (BMI) greater than 40.
Our endocrine surgery group previously described, in a preliminary report, our experience that compared the results of TLA and PRA in 48 consecutive patients. 28 In our experience, mean operative times of PRA are decreased in comparison with TLA, with comparable complication rates and hospital stay. PRA has advantageous features for patients with bilateral adrenal tumors and patients with previous extensive anterior abdominal operations. Since September 2006, PRA has become our preferred approach for the removal of selected adrenal neoplasms.
Technical development
All procedures were performed with the senior author (TCL) as primary surgeon. A previous extensive experience record with advanced laparoscopic techniques with an emphasis on adrenalectomy benefited the approach to technical development planning. 39,40 As a prelude to the transition to robot assistance, our group performed more than 30 PRAs using standard laparoscopic techniques, with acceptable excellent outcomes, 28 comparable with previously published series. The coauthors (ATL, KRW, PSL, HTP) contributed previous experience with advanced urologic and colorectal robot-assisted techniques, and directly assisted with troubleshooting the technical aspects and evolution of the operative procedure in the operating room.
Before initiation of the study, the primary surgeon (TCL) completed training in the use of the da Vinci® Surgical System (Intuitive Surgical, Sunnyvale, CA) at the Robotic Surgery Training and Certification Lab (Hermann Hospital, Houston, Texas). Technical considerations for the planned operation were investigated by the surgeon, including patient positioning, port site placement, optimal robot approach angles, and required instrumentation. After this extensive planning, the robot-assisted operation was successfully performed in a live anesthetized pig model before transitioning robot assistance to surgical care of patients.
The development of the surgical procedure and technique was predicated by the formal medical and surgical training of the authors and appropriate hospital credentialing and proctoring. Patients were entered into the study under a protocol approved by the Institutional Review Board, and appropriate clinical preoperative informed consent was obtained in all patients. Adrenalectomy was performed for standard clinical indications, and the operative procedure was not altered in patients who underwent a robot-assisted operation.
Operative procedure
General endotracheal anesthesia was provided, a urinary catheter was placed, and appropriate hemodynamic monitoring was instituted. An arterial line and/or central venous catheter were placed for patients with hormonally active tumors or as otherwise clinically indicated. Patients were rotated into the prone position on a specialized, padded operating table surgical saddle (#NL999, Cloward® Instruments Corporation, Honolulu, HI), allowing the patient's abdominal viscera to fall anteriorly and for reduction of the lumbar lordosis to optimize exposure. All potential pressure points were extensively padded. Because the robot was advanced from above the contralateral shoulder, the contralateral arm was protected and tucked at the patient's side.
The operation performed is a hybrid procedure, placing the initial ports and creating the operating space laparoscopically. The da Vinci robot (standard) is then docked to complete the dissection of the adrenal gland. Initially, an approximately 1.5 cm transverse incision is made below the 12th rib tip (Fig. 1), and the retroperitoneal space is entered by sharp dissection and minimal blunt digital exploration. Next, small incisions are made a minimum of 5 cm medial and lateral to the initial access incision, and two additional 8.5 mm robotic ports are placed under the direction of a finger placed into the retroperitoneal space. A 12-mm blunt trocar (#OMS-T12BT, AutoSuture/Covidien, Mansfield, MA) with an anchoring inflatable balloon and adjustable sleeve is placed in the center access site. The operating space is created by insufflating with carbon dioxide to a pressure between 18 and 24 mm Hg. In general, lower pressures are initially used and increased only high enough to provide an adequate operative working field. Videoendoscopy is performed initially with a hand-held 5-mm, 30-degree endoscope.

Anatomic landmarks (patient, posterior view) and locations of access incisions for left adrenalectomy.
The Gerota fascia is bluntly opened and the retroperitoneal fat swept away to expose the upper pole of the kidney. The da Vinci patient side cart is then brought in superiorly, over the patient's contralateral shoulder, along an oblique line connecting the surgeon, operative target, and the main axis of the robot (Fig. 2), and docked for the robotic portion of the procedure. A 12-mm, 30-degree or 0-degree da Vinci endoscope camera is then used, depending on anatomic considerations. The camera arm is docked to the central port site, and two (left and right) instrument arms are used for the medial and lateral smaller port incisions. Because of lack of additional space in the operative field, the da Vinci fourth arm was rotated out of the way and not used.

General operating room procedure setting for left robot-assisted retroperitoneoscopic adrenalectomy.
The majority of the necessary dissection of the adrenal gland is completed with either the ProGrasp™ and Cadiere grasper, combined with the Fenestrated Maryland bipolar or PreCise™ bipolar cautery (Endowrist® 8 mm instruments, Intuitive Surgical, Sunnyvale, CA) used in the surgeon's two operative hands. The Harmonic® curved ultrasonic energy shears can be helpful in dividing small arterial branches when dissecting the periadrenal fat. The adrenal vein is divided between surgical clips (Hem-o-lok® clip applier, Intuitive Surgical, Sunnyvale, CA; Endo Clip* II M2 reference #176657 or Endo Clip™ III reference #176630, AutoSuture/Covidien, Mansfield, MA).
Using standard laparoscopic technique, the dissection is begun using the upper pole of the kidney as the initial anatomic landmark (Fig. 3). Specifically, the elements of the operation completed laparoscopically include accessing the retroperitoneal space, placing the additional trocars under digital guidance, and the initial blunt dissection of the Gerota fascia and sweeping apart of the retroperitoneal fat to expose the upper pole of the kidney.
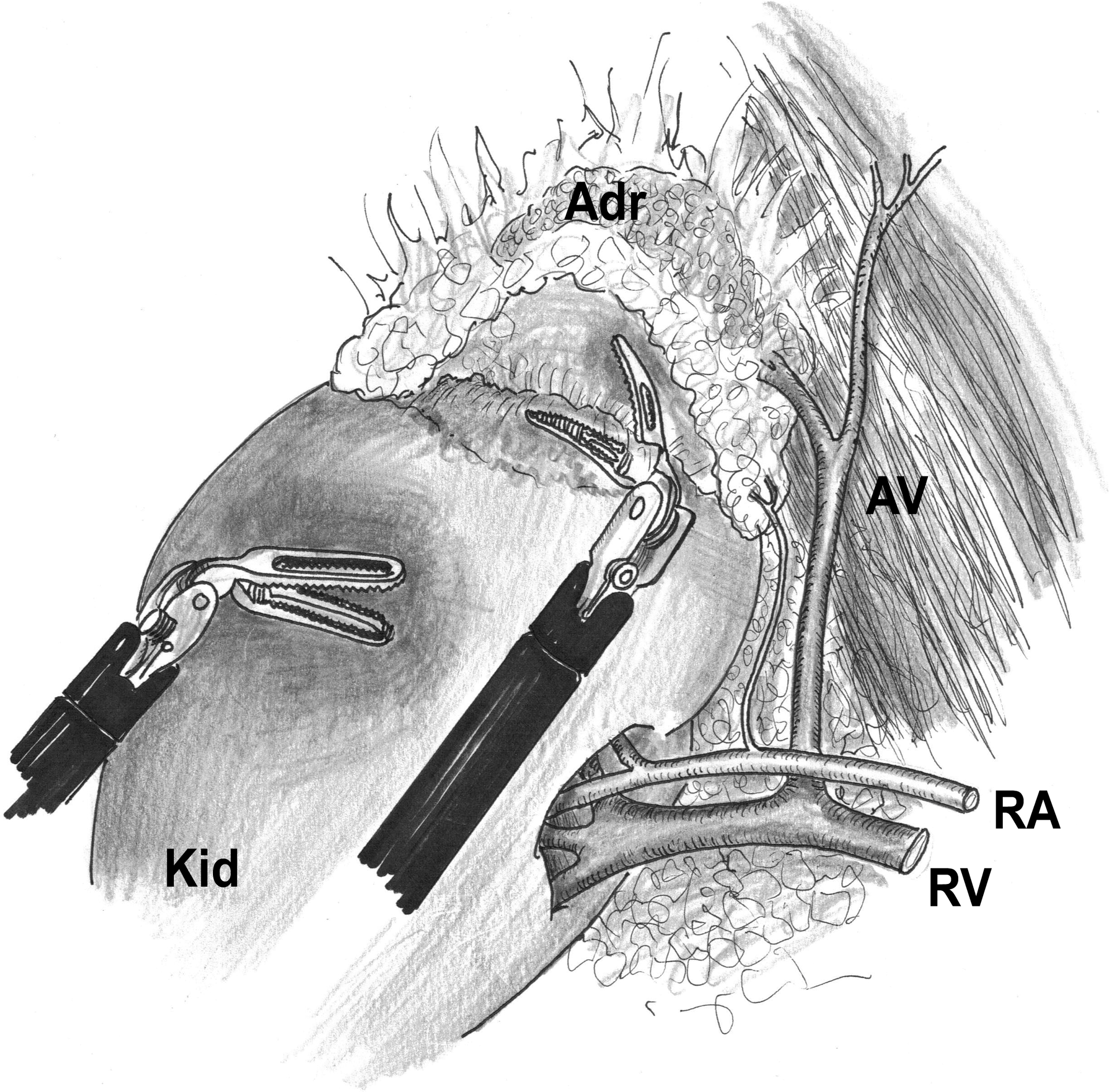
Dissection of left adrenal gland with robotic instruments; operative view from the posterior approach. Kid = kidney; Adr = adrenal; AV = adrenal vein with phrenic branch; RA = renal artery; RV = renal vein.
After exposing this critical landmark, the robot is docked, and adrenal dissection is completed robotically. The upper pole of the kidney is gently retracted laterally and inferiorly, and the inferior and medial border of the adrenal gland is dissected. The superolateral (diaphragmatic) and anterior (peritoneal) attachments of the adrenal gland are left intact until later, leaving the gland anchored for optimal dissection. Inferomedially, the adrenal vein is identified early and divided between surgical clips. The adrenal vein anatomy can be variable, especially on the right (as reviewed by Walz et al 23 ). Using gentle blunt retraction of the adrenal gland, the remaining periadrenal fat and attachments are divided to complete the dissection. The robot is then undocked, and the adrenal gland is removed in a specimen bag.
Results
Six consecutive patients underwent RAPRA between June 23, 2009, and January 23, 2010. The demographic and clinical data are presented in Table 1. There were five women and one man, with an age at the time of operation ranging from 45 to 75 years (mean 55.5 years). The BMI for the patients was between 28 and 36, with a mean BMI of 30. The tumors were equally divided with regard to laterality, including three right adrenal tumors and three left adrenal tumors.
BMI = body mass index; EBL = estimated blood loss; LOS = length of stay.
The RAPRAs were performed for two functional (aldosteronomas) adrenal neoplasms, and four adrenocortical adenomas that were atypical or suspicious by radiographic criteria, or that had increased in size over serial radiographic evaluation. The size of the resected adrenal tumors was 1.1 cm to 4.3 cm (mean 2.8 cm). There were no malignant adrenal masses. In accordance with the initial candidate criteria for RAPRA, all tumors were benign and well less than 7.0 cm, and no patient with a BMI greater than 40 was included.
The operative data from the six patients undergoing RAPRA is depicted graphically in Figure 4. For the series, the mean operative time from incision to dressing application was 143 minutes, with a mean robot time of 57 minutes. The second attempted robot-assisted adrenalectomy in the series was a 52-year-old man with a BMI of 36 (the largest in the series). This case occurred early in our experience with the technique and proved to be a very difficult operation for anatomic reasons. Only a portion of the case was completed with robot assistance, because of failure to progress at a satisfactory rate. For this reason, the robot was undocked, and the adrenal gland dissection was successfully completed with standard laparoscopic instrumentation. Although this may be the result of a learning curve for posterior robotic adrenalectomy, the possibility that standard laparoscopic techniques may prove superior even after more experience should also be considered.
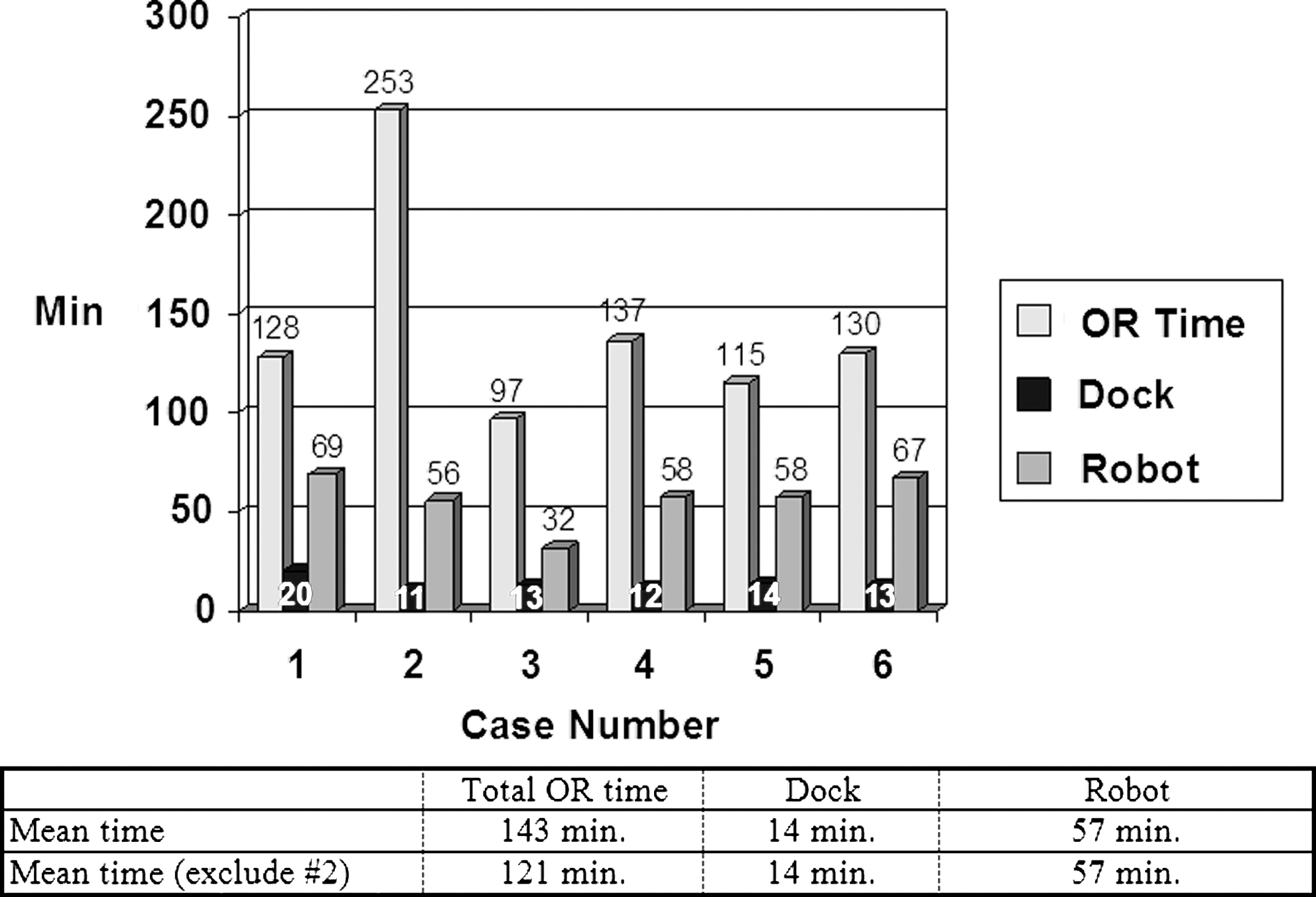
Graphic representation of operating room (OR) times, docking times, and robot times for the six consecutive robot-assisted posterior retroperitoneoscopic adrenalectomy cases. The times in minutes are indicated numerically above each bar in the Figure. The mean times for all cases, and for all cases except case 2, which could not be completed robotically, are indicated below.
Excluding case #2, which was performed with robot assistance in part but completed laparoscopically, the mean operative time in the remaining five patients was 121 minutes. The robot time was similar for all patients in the series, with a range of 32 to 69 minutes (mean 57 min). Docking times for all patients in the series were also very comparable and acceptable, including a range of 11 minutes to 20 minutes (mean 14 min). The single outlier was the first case with a docking time of 20 minutes, which included a redocking secondary to robot arm collision. Docking times for the remaining cases were between 11 and 14 minutes.
With regard to the portion of the procedure completed without robot assistance, the average total laparoscopic time (total operative time minus docking time, minus robot console time) is 50 minutes, compared with an average robot console time of 57 minutes. In addition to the initial laparoscopic blunt dissection to identify the upper pole of the kidney (as detailed above), this nonrobot time also includes the time needed for initial access of the retroperitoneal space, optimal trocar insertion under direct digital guidance, the removal of the adrenal gland in a laparoscopic catchment bag, and fascial as well as skin closure.
Hemodynamic changes during the procedure were not specifically studied. Typically, developed mild transient hypercapnia with the increased capnoretroperitoneoscopic pressures of 18–24 mm Hg developed, which was self-limiting and resulted in no evident deleterious sequelae. There were no major adverse intraoperative cardiovascular complications, anesthetic complications, or complications related to the prone positioning.
All patients did well after RAPRA, with a postoperative course similar to patients who were undergoing TLA or laparoscopic PRA. The hospital length of stay was 23 hours or less (1 day) in four patients, and 2 days in the remaining two patients. Estimated blood loss was minimal for all patients (range <50 mL to 100 mL; mean <60 mL). There was no morbidity. No patient experienced a grade II or III 41 complication, such as pneumothorax, acute blood loss anemia/transfusion, postoperative fluid collection necessitating drainage, or need for additional procedures. The patients with hormonally active (aldosterone-producing) adenomas demonstrated improvement in their signs and symptoms of primary hyperaldosteronism after adrenalectomy, in keeping with evidence from removal of these tumors by other minimally invasive approaches. 40
Postoperative analgesic requirements were reviewed from the available hospital chart records, and time for convalescence/return to work was recorded where information was available. This information was sought to get an idea of the patient's typical postoperative course, but no direct comparative study with other surgical approaches was attempted or appropriate in the small initial series of patients in this feasibility study. Postoperative intravenous narcotic analgesia requirements ranged from approximately 0 to 20 mg morphine sulfate or equivalent in divided doses, usually over the first 16 to 20 hours postoperatively. Two patients received supplemental intravenous ketorolac, 60 to 180 mg. Patients were transitioned to oral narcotic pain medications on the first or second postoperative day before discharge. In general, oral narcotics were needed for 8 days or less, except for one outlier who continued for 8 weeks secondary to a described “dull,” mild discomfort in that flank that eventually completely resolved.
Completed convalescence and return to work ranged from 2 to 6 weeks, except for one outlier who did not need any oral narcotic pain medications after discharge and returned to full-time work on postoperative day 4. No patient in this initial small series experienced prolonged numbness or severe flank pain from segmental nerve injury, and there were no evident muscle weaknesses of the flank or abdominal wall or trocar site hernias. Although no direct comparative analysis of results was attempted or could be performed comparing RAPRA with TLA or laparoscopic PRA procedures, these features of postoperative recovery and pain and convalescence appeared similar to that of other minimally invasive approaches for adrenalectomy.
Discussion
Minimally invasive techniques have been firmly established for the management of an increasingly broad spectrum of surgical pathologic entities. Continuing advances in technology and instrumentation are being applied to achieve improved outcome goals. The logical progression of advances that are provided by laparoscopic techniques is the incorporation of robotic surgical systems. The application of robot-assisted surgery techniques may have significant potential in contributing to procedures that require increased surgeon flexibility, maneuverability, and dexterity in a relatively small working space. Additional significant advantages may include 3D visualization and magnification, tremor minimization, and scale movements for improved accuracy of delicate dissections.
Still, many potential obstacles to further advancement of this technology continue to exist. A few of these include the loss of the surgeon's operative tactile (haptic) sensation and feedback, cost, increased infrastructure and support personnel needs, more complex setup requirements, and the large size of current robotic surgical systems. Although these current deficiencies continue to be addressed, the application of robotic technology to a minimally invasive surgical procedure carries potential advantages in operative efficiency and comparable or improved results and patient outcome.
Minimally invasive adrenalectomy is the preferred surgical treatment for the removal of small, benign adrenal neoplasms. Current laparoscopic approaches include TLA, lateral posterior adrenalectomy, and PRA. PRA has the potential advantages of a more direct anatomic approach, fewer laparoscopic port sites and/or fewer incisions, and increased operative simplicity in patients with bilateral tumors or multiple previous anterior operations. A few important aspects of this operation include the small working space and limitations in maneuverability and operative angles for dissection or application of surgical clips.
In general, PRA does not require complex or advanced suturing techniques. The single major vascular structure to be identified and divided between clips is the adrenal vein. The arterial vascular supply consists of multiple small vessels in the periadrenal fat, and these can be effectively divided using bipolar cautery, or preferably by an ultrasonic energy device, such as the Harmonic curved shears.
Robot-assisted surgery has the potential to offer advantages, including the ease and precision of identifying and dividing the adrenal vein and dissecting the adrenal gland in a small working space with limited access and surgical approach angles. Important potential limitations are the small area of the back for surgical access and difficulty in achieving separation of more than 5 to 8 cm for the access incisions, and preventing physical conflict of the robot arms. Any potential surgical advantages of the robot-assisted technique for PRA require additional experience and study, and no conclusions can be made with this initial feasibility study.
We used a hybrid procedure with robot assistance to dissect the adrenal gland in an initial series of six patients. After initial access of the retroperitoneal space by standard laparoscopic techniques, successful complete dissection of the adrenal gland was achieved in five of the six patients. The second case attempted was characterized by difficult anatomic considerations, and only a portion of the dissection could be performed robotically. Because this was early in our experience, it was elected to complete this complex operation laparoscopically. As for all new procedures, technical challenges and a surgeon learning curve may exist. Alternatively, standard laparoscopic techniques may ultimately prove superior after further experience and study.
The results reported indicate that RAPRA can be safely performed with reasonable operative times. The mean total operative time for the five procedures in which the entire adrenal dissection was completed robotically was approximately 2 hours (121 minutes), with a range of 97 to 137 minutes. Even in this initial series, these times are only marginally greater than reported operative times for other minimally invasive adrenalectomy approaches. Total mean robot time was 57 minutes, indicating that the dissection progressed adequately after successful docking. Although not evident in this small series, docking times and operative times should be expected to decrease with experience and increased familiarity.
Potential advantages and/or limitations may be associated with the addition of robot assistance to PRA. The magnified 3D image visualization and enhanced instrument degrees of freedom are features of the robotic system that may have potential surgical advantages for PRA, but more experience and study is necessary to answer these questions. While robot assistance provides the greatest advantage in reconstructive procedures that necessitate precise laparoscopic suturing (not adrenalectomy), the articulating Endowrist instruments have the potential to provide some advantages in working within the confined small space of the retroperitoneum. Although a Harmonic scalpel is available for the da Vinci system, its energy source does not currently allow for articulation of the instrument tip. We found the Maryland Bipolar and Monopolar Curved Shears to be more useful in dissecting and ligating small vessels around the adrenal gland.
There are some current instrumentation and technologic limitations that warrant some comment. The da Vinci system lends itself to the small, fixed field within the retroperitoneum; however, the PRA also necessitates trocar placement that is relatively close. This can lead to instrument and camera arm collisions that may lead to impaired mobility on the right or left side. To minimize collisions, it is crucial to dock the patient-side cart precisely in a parallel line along the axis from the camera trocar to the target organ and provide as much separation as possible between all three trocars. The three trocar configuration also limits the ability for the scrubbed assistant to provide continuous suction and/or countertraction during the procedure. In our experience to date, when intermittent suction was needed for bleeding and or cautery smoke, it was provided by removing the robotic instrument and having the assistant surgeon insert a standard laparoscopic suction device into the robotic port and manually provide suction. Alternatively, for more significant bleeding, the authors would recommend placing an accessory trocar to allow for dynamic suction. A robotic suction instrument is not currently available, but we have been in discussions to advocate its development for this procedure. In the future, smaller or flexible robotic platforms may address some of the technical limitations of the current technology.
Lastly, but not least important, cost for use of the robot-assisted approach remains a major consideration. Even when the initial acquisition cost of the system is not included, fixed costs of disposable equipment are a barrier that may be justified if operative times are significantly decreased with further experience. Cost savings of operative charges with increased experience have been reported with other robot-assisted procedures, including prostatectomy. 42 Despite these savings, a major criticism of robot-assisted prostatectomy is that open and standard laparoscopic approaches are less costly. 42,43 Whether these cost analyses may translate to adrenalectomy is unknown.
In this small initial series, patients who were undergoing RAPRA had expected good outcomes with essentially no morbidity and no mortality. These results are comparable to those of other patients who were undergoing minimally invasive adrenalectomy. The study demonstrates the feasibility of robot-assisted posterior adrenalectomy and reports its successful performance with good results in an initial series of patients. Currently, there is insufficient experience with the results of this operation to make any conclusions regarding improved patient outcome. There are several potential technical advantages to this surgical approach as described above. These significant potential advantages must be weighed against the increased cost, requisite surgeon learning curve, and requirements for complex instrumentation and specialized support staff to complete the procedure. More experience will be needed to answer these questions. The inclusion of other current advances such as robotic adaptations of single incision laparoscopic surgery represent future areas for study.
Conclusion
We performed RAPRA in an initial six patients with acceptable operative times and expected excellent outcomes. To our knowledge, this report represents the first description of the use of robot assistance for PRA and analysis of early results. In this small series of patients, we found the procedure to be safe and effective. This is a feasibility study to demonstrate that RAPRA can be performed. Further study is needed to determine whether the robotic approach to PRA has operative advantages, is clinically superior, or is cost-effective.
Footnotes
Acknowledgments
The authors would like to acknowledge John C. Hendricks, M.D., for contributing original illustrations (Figures 1, 2, and ![]() ); Samuel K. Snyder, M.D. (Scott & White, Temple, Texas) and Jeffrey E. Lee, M.D. (M. D. Anderson Cancer Center, Houston, Texas) for assistance with learning and developing the posterior adrenalectomy approach at Scott & White; Kamran S. Hamid, M.D., for assistance with the manuscript preparation; and Jose Armando Garcia, ORT, Surgical Robot and Coordinator and Trainer, Robotics Program, Memorial Hermann Hospital, Texas Medical Center, Houston, Texas, for technical advice and assistance with the robotic surgical system.
); Samuel K. Snyder, M.D. (Scott & White, Temple, Texas) and Jeffrey E. Lee, M.D. (M. D. Anderson Cancer Center, Houston, Texas) for assistance with learning and developing the posterior adrenalectomy approach at Scott & White; Kamran S. Hamid, M.D., for assistance with the manuscript preparation; and Jose Armando Garcia, ORT, Surgical Robot and Coordinator and Trainer, Robotics Program, Memorial Hermann Hospital, Texas Medical Center, Houston, Texas, for technical advice and assistance with the robotic surgical system.
Disclosure Statement
No competing financial interests exist.