
Abstract
A novel technique for achieving complete laparoscopic excision of the intramural ureter with a bladder cuff is presented using the bulldog clamp without opening the urinary tract.
Problem
The technique presented here uses the bulldog clamp and allows for the precise excision of the complete bladder cuff without opening the urinary tract. This method prevents spillage and enables the removal of the entire specimen en bloc. This technique also eliminates the need for a stapler, thus reducing the potential risk for stone formation.
Technique
Under general anesthesia, the patient was placed in a semilateral position. The camera port was inserted via an infraumbilical incision, and two additional trocars were placed under direct laparoscopic vision in a triangular shape. Another port was placed on the posterior axillary line for assistance, and, if necessary, an additional 5-mm port was used for liver retraction on the right side. Transperitoneal laparoscopic nephrectomy was performed using the standard technique while leaving the ureter intact. After identification of the ureter at the level of the pelvic brim, the patient was repositioned in the Trendelenburg position. An additional working port was placed in the lower quadrant of the contralateral side to aid the ureteral dissection. The ureter was traced and mobilized to the detrusor hiatus. The superior vesical artery and vein were secured at the level crossing the dissected ureter and transected. The ureter was further caudally dissected until the detrusor muscle fibers of the ureterovesical junction could be identified. The intramural part of the ureter was dissected under direct vision and freed from the surrounding detrusor muscle by sharp and blunt dissection. The detrusor muscle was sharply incised and further dissected away from the underneath bladder mucosa with 1 cm around the ureteral orifice. A well-circumscribed bladder mucosal cuff could be identified around the ureteral orifice. The dissected mucosa appeared as a cone-shaped structure when applying traction on the distal ureter (Fig. 1). A laparoscopic bulldog artery clamp (Aesculap, Tuttlingen, Germany) was inserted through the upper midline 12-mm port and placed at the base of the mucosal tent. The ureter was clipped with a Hemolock™ clip (Weck Systems, Triangle Park, NC) proximal to the site of the bulldog clamp (Fig. 2). The bladder mucosal cuff was sharply excised using endoscissors (Fig. 3).
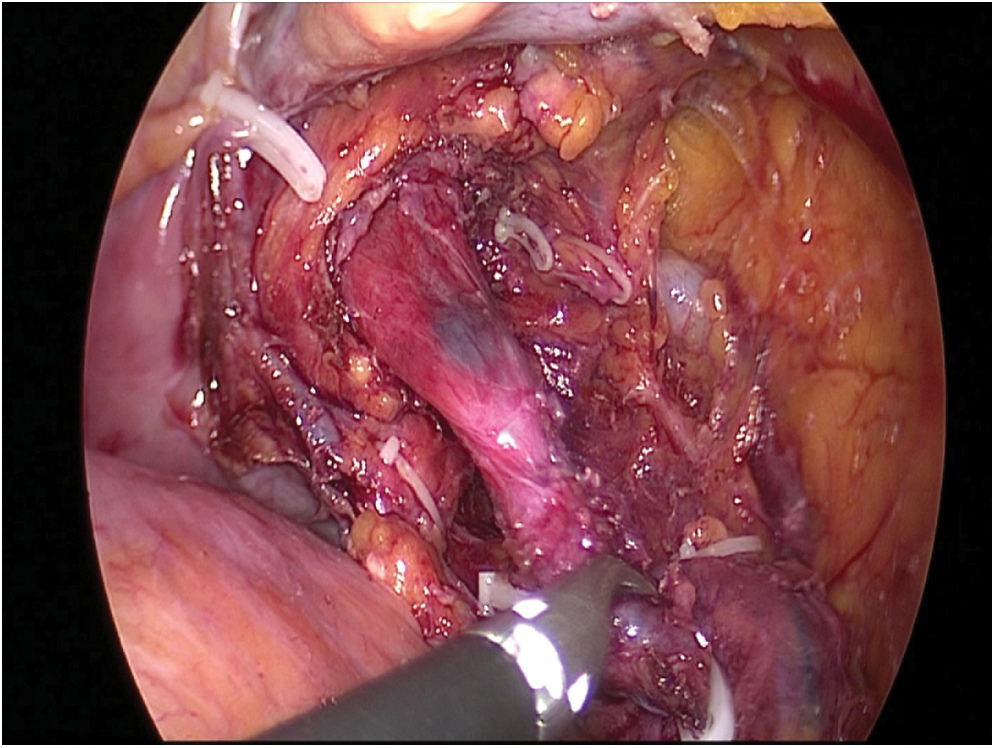
A tent-shaped bladder mucosal cuff.

A bulldog clamp was placed in the bladder mucosal cuff.

Pathological specimen: note the completely resected bladder cuff.
When suturing the bladder mucosa, the clamp was still in place to block the urine. The bladder was closed in two layers using free-hand intracorporeal suturing with 3–0 absorbable polygalactin (Vicryl) sutures. The mucosa was sutured in a running fashion, and the clamp was removed. The second seromuscular closure was then repaired with two or three intermittent sutures. The peritoneal reflection was also closed using 3–0 Vicryl sutures. The specimen was removed intact in a Lap bag (Sejong Medical, Seoul, Korea) through a 7-cm Pfannenstiel incision.
The most crucial element during distal ureterectomy and bladder cuff excision is complete resection of ureter orifice. When detrusor muscle is sharply incised and dissected from underlying mucosa, traction of distal ureter will reveal cone-shaped bladder mucosa. This phenomenon ensures that enough bladder cuff is resected. Further, tactile sense of the bladder mucosa through laparoscopic forcep is different from that of the ureteral wall, which should further ascertain the surgeon that the entire ureter orifice is being resected.
This technique was technically simple and effective in all cases. We have used this technique to treat five male and three female patients. During dissection of distal ureter, intestine or colon did not obscure our view or instruments. However, in female patients, ovary and fallopian tube became an obstacle. These structures were temporarily sutured to peritoneum to provide better visualization. Laparoscopic bladder suturing can be challenging due to a relatively difficult area to suture, but if the surgeon has the technique to perform urethrovesical anastomosis during laparoscopic radical prostatectomy, pure laparoscopic suturing after cuff resection should not be difficult.