
Abstract
Ureteral injury is usually iatrogenic after gynecologic or obstetric surgeries. Ureterouterine fistula is a rare complication. It most commonly occurs after a caesarean section. A 24-year-old woman presented with paradoxic incontinence 1 week after caesarean section. Intravenous urography revealed a left ureterouterine fistula. She was treated successfully by laparoscopic ureteroneocystostomy.
Introduction
Case Report
A 24-year-old primipara presented with paradoxic incontinence of urine. One month before presentation, she had undergone a cesarean section for obstructed labor at another center. Because of intraoperative bleeding, the obstetrician had taken hemostatic suture at the left lateral margin of the uterine incision. One week after discharge, however, she noticed urinary leakage from the vagina. A urethral catheter was kept indwelling for 4 weeks, which did not reduce the leakage from the vagina. The patient was then referred to our institution. On speculum examination of the vagina, urine could be seen leaking from the cervical os and no fistulous opening in the vaginal vault. Cystoscopy examination revealed a normal bladder but no left ureteral efflux. Excretory urography revealed moderate left hydroureteronephrosis with narrowing about 3 to 4 cm from the ureterovesical junction, and contrast filled the uterus.
While the patient was under evaluation, fever and left flank pain developed. A percutaneous nephrostomy under ultrasonographic guidance was placed, which drained turbid urine. Urine culture from the nephrostomy grew Escherichia coli. She was treated with appropriate antibiotics. Intravenous pyelogram (IVP) showed bilateral functioning kidneys and left ureter draining directly into the uterus (Fig. 1). CT nephrostography confirmed the same finding (Figs. 2 and 3).

Intravenous pyelogram (IVP) showing left ureter draining directly into the uterus.

CT nephrostogram demonstrates left ureter draining directly into the uterus.

Three-dimensional reconstruction CT nephrostogram shows left ureter draining directly into the uterus.
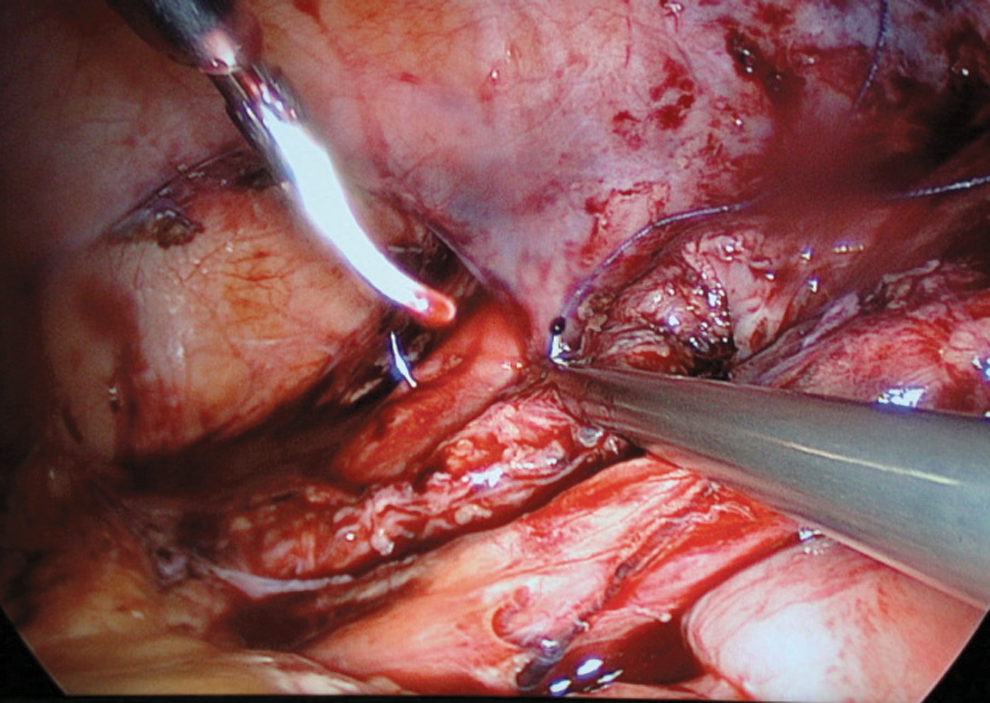
We used a 12-mm port via the umbilicus and two additional working ports in the midclavicular line just below the level of the umbilicus. The left ureter was identified at the pelvic brim and followed distally. The ureter was dissected from the surrounding tissues, keeping its vascularity intact. There was a communication between the ureter and the lower portion of the uterus (Fig. 4). The fistula tract was dissected meticulously and transected (Fig. 5). A 4.8F Double-J ureteral stent over 0.032 Terumo guidewire was placed retrogradely into the ureter (Fig. 6). A tunnel was marked on the bladder surface with electrocautery while the bladder was semidistended. A 4-0 polyglactin traction suture was applied at the proximal end of the detrusor tunnel. The detrusor incision was carried out in a proximal-to-distal direction. The serosa was scored with cautery, but most of the dissection was performed with scissors to prevent injury to the bladder innervation. The ureter was positioned in the new tunnel and 4-0 polyglactin suture was placed at the most proximal end to stabilize the ureter.
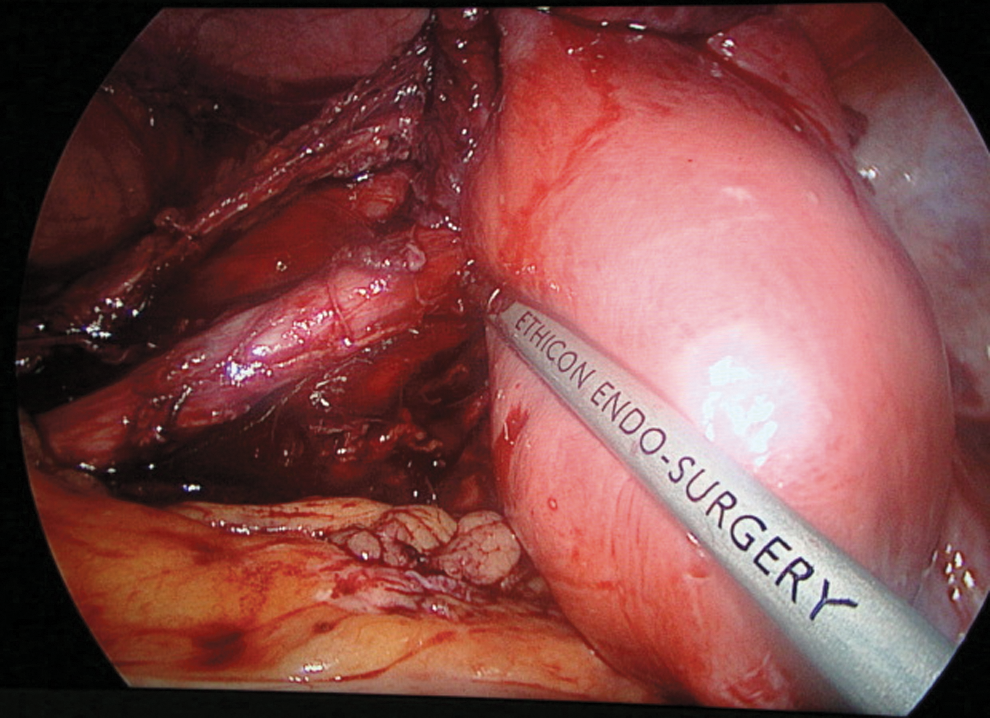
Intraoperative photograph reveals direct communication between the left ureter and uterus.
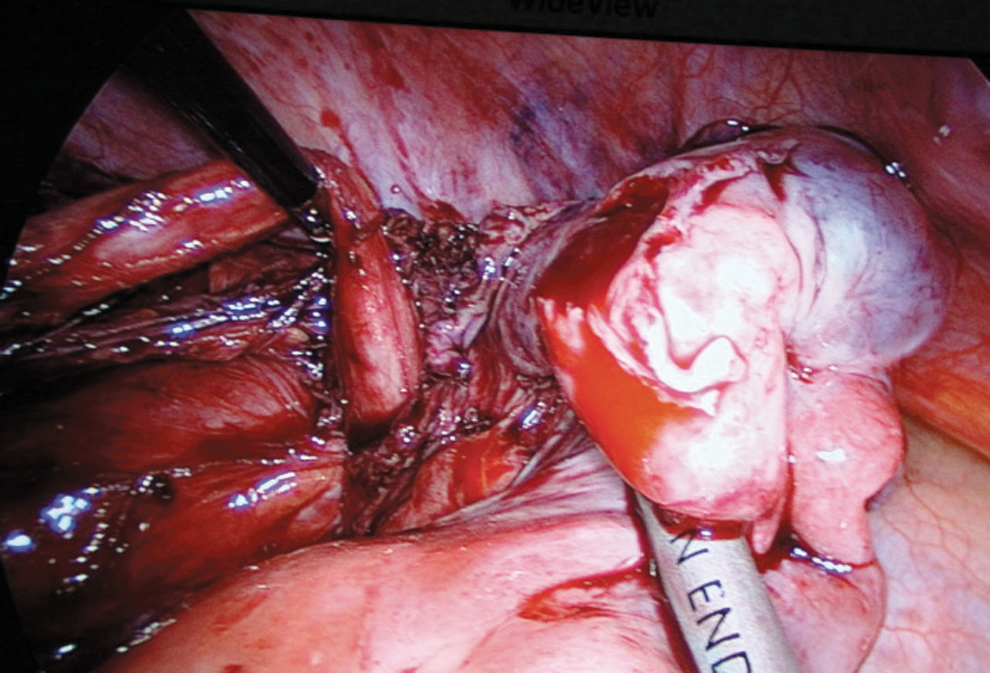
Ureter opening into uterus after further dissection.

Insertion of 4.8F Double-J stent retrogradely into the left ureter after spatulation.
The distal end of the Double-J shaped stent was placed in the bladder through the cystotomy site. Ureterovesical anastomosis was performed with 4-0 polyglactin interrupted sutures (Figs. 7 and 8), starting at the ureteral orifice distally. Psoas hitch sutures were applied (Fig. 9). A nonsuction drain was placed near the anastomotic site. A catheter was left in the bladder for 1 week postoperatively. Postoperative nephrostography showed complete healing of the fistula and good drainage into the bladder (Fig. 10). The postoperative hospital stay was 3 days.
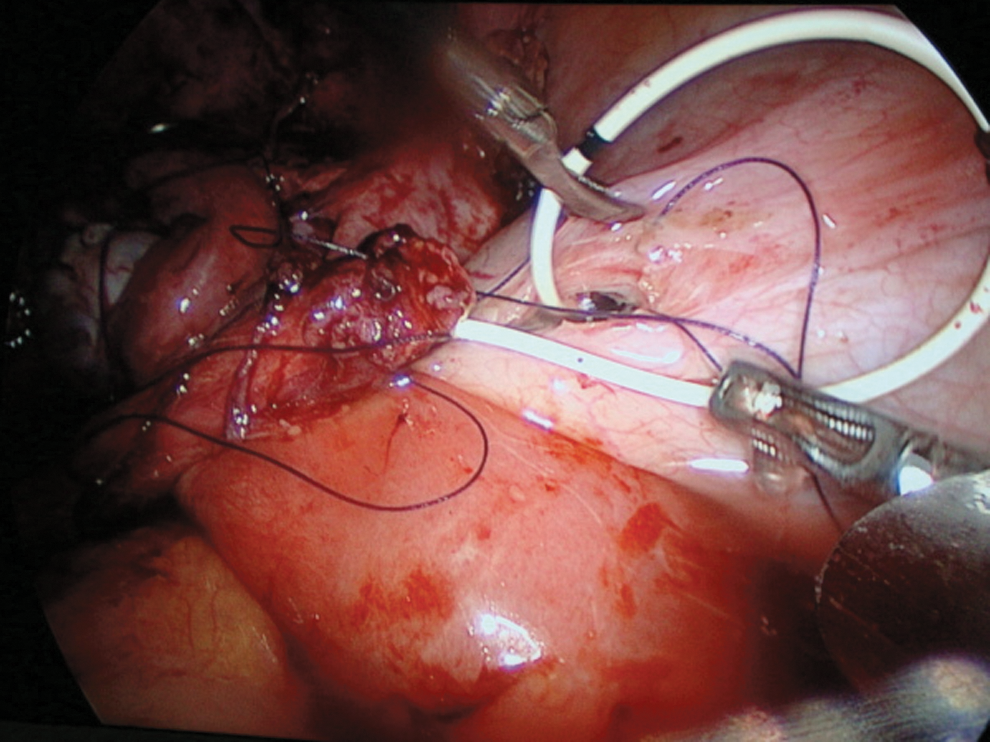
Ureterovesical anastomosis in progress over Double-J stent.

Completed ureterovesical anastomosis using interrupted polyglactin sutures.
Applying psoas hitch sutures to relieve the tension of the anastomosis.
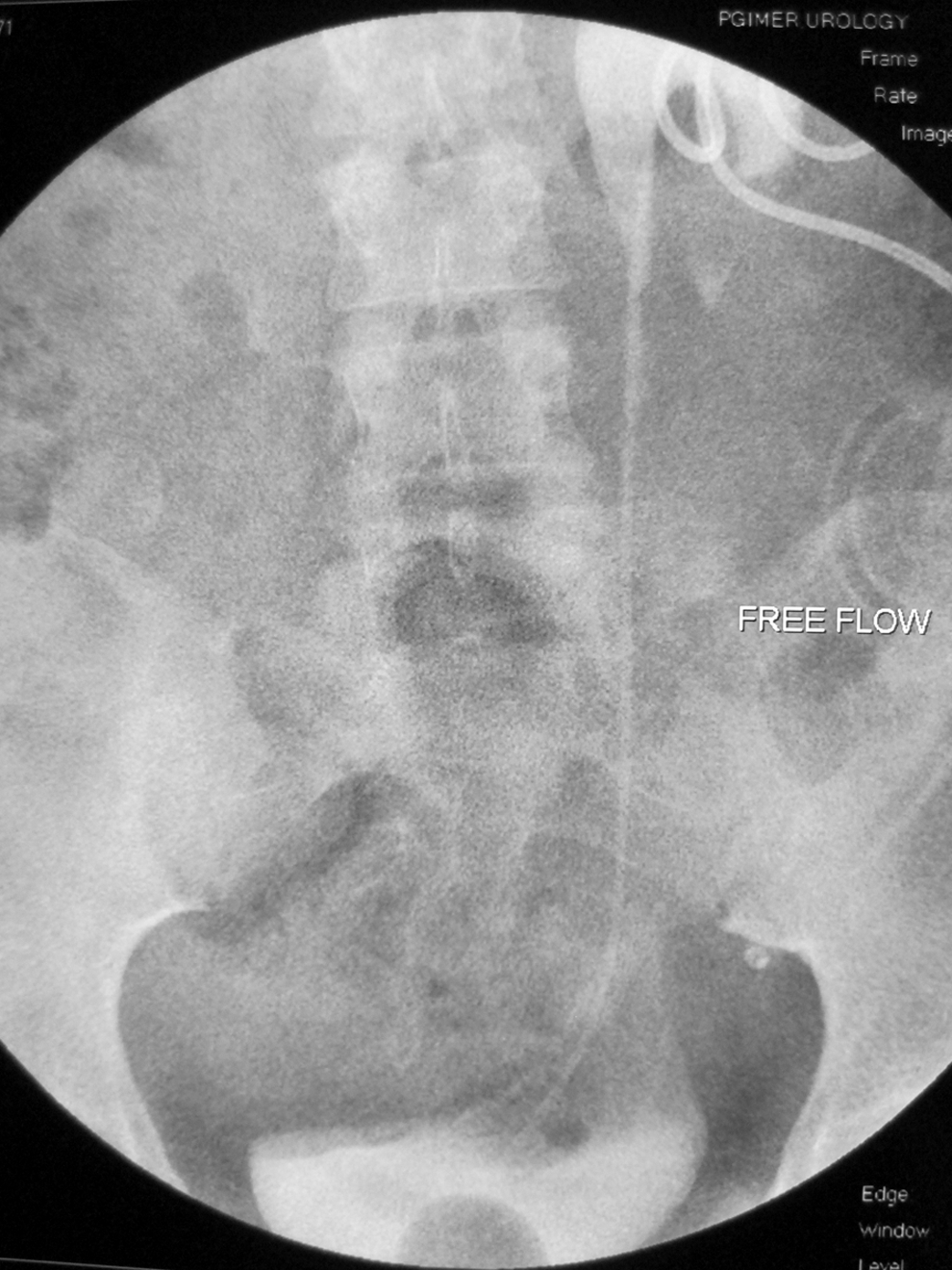
Follow-up nephrostogram shows free flow of contrast into urinary bladder.
Discussion
Ureterouterine fistula is a rare complication after gynecologic or obstetric surgeries. 5 The terminal ureter can be injured by sutures or ligation in the process of achieving hemostasis. The predisposing factors are prolonged obstructed labor; continued compression of the terminal ureter and cervix against the pelvic brim, leading to pressure necrosis, especially in cephalopelvic disproportion; and lateral extension of the transverse incision on delivery of the fetal head in a thinned out lower segment. 2 During cesarean section, this can occur if the incision on the uterus is low and extends too far laterally to involve the ureter; if the ureter is damaged during attempts to achieve hemostasis at the lateral margin; or a small collection or hematoma forms around a partially damaged ureter that becomes infected. 2 The dextrorotation of the uterus brings the left ureter near to the left angle of incision, injuring it more frequentaly. 6 Ureterovaginal or uterus fistuli are often the result of distal obstruction (traumatic or ischemic) beyond the point of injury—therefore allowing for the development of fistula and passage of urine through the path of least resistance (ie, fistula).
Presentation of such fistulas is usually in the form of paradoxic incontinence. The goals for management of ureterouterine fistulaa are preservation of renal function and restoration of ureteral integrity through ureteroneocystostomy or end-to-end anastomosis. 7 In patients who present early and with an intact ureter distal to the fistula, this can be achieved by placing a ureteral catheter or stent. 8 In our case, the left ureter was opening directly into the uterus with no contrast entering the ureter distal to the fistula. Percutaneous nephrostomy may be used to divert urine and ensure adequate drainage, thus conserving renal function and allowing any infection and inflammation to settle. We feel that a waiting period of 6 weeks is enough for ureteroneocystostomy, because by that time, the uterus would have involuted and there would not be any significant inflammation in the ureter and uterus. Alternatively, ureteral reimplantion may be performed primarily. In the literature, all the cases have been managed by open ureteroneocystostomy or sometimes endoscopically when ureteral catheterization was successful. Laparoscopic ureteroneocystostomy is a minimally invasive procedure with excellent postoperative recovery and good short-term result. 9
Conclusion
It is mandatory for gynecologists and obstetricians to pay careful attention to the anatomy of the urinary tract to avoid iatrogenic injury. Percutaneous nephrostomy can be used as temporary management for some of these injuries. Ureterouterine fistula can be successfully managed with laparoscopic ureteroneocystostomy with minimal morbidity. The short convalescence period associated with laparoscopic surgery helps the mother resume nursing care at the earliest.
Footnotes
Disclosure Statement
No competing financial interests exist.