
Abstract
Background and Purpose:
Postoperative incontinence is multifactorial after radical prostatectomy. Using endorectal coil MRI, we examined features of the male urethra and accompanying muscular sphincter to predict continence after robot-assisted radical prostatectomy (RARP).
Patients and Methods:
80 patients underwent preoperative 1.5 Tesla endorectal coil MRI. Urethral length was measured in the coronal plane. All patients underwent RARP. Questionnaires were completed by patients at monthly intervals. The primary end point was time to continence defined as necessitating 0 to 1 pad per day (PPD). Statistical analysis was performed using Cox regression models to create both univariate and multivariate survival models.
Results:
Mean age was 59.7 (standard deviation [SD] 7.1); 98% had bilateral nerve sparing. Mean urethral length was 17.1 mm (SD 4.5 mm). Mean prostate size was 34.7 g (SD 17.8). By 3 months, 60 patients achieved 1 PPD (mean 8.1 weeks, SD 9.4) and 34 patients achieved 0 PPD (mean 10.5 weeks, SD 8.0). Time to social continence was significantly related to prostate size both as a continuous variable (P = 0.01), and as a dichotomized variable of ≥50 vs < 50 g (P = 0.02). Increased urethral length was related to decreased time to continence both as a continuous variable (P = 0.06), and when dichotomized to ≥20 vs < 20 mm (P = 0.08). In addition to larger prostate size (hazard ratio [HR] 0.97, P < 0.04), older age (0.95 P < 0.025) was also associated with a longer time to achieve 0 PPD. Multivariate analysis revealed that longer urethral length was associated with a faster recovery of continence (HR 1.11, P < 0.01). After controlling for age and urethral length, patients with a prostate size ≥50 g had 75% lower likelihood of achieving continence at all time points when compared with patients with prostate size <50 g (HR 0.25; 95% confidence interval: 0.06, 1.06; P = 0.06).
Conclusions:
Longer urethral length increased the likelihood of achieving continence at all time points postoperatively. Advanced age and larger prostate size were negatively associated with continence outcomes.
Introduction
Nerve-sparing technique as first described by Eggleston and Walsh 8 and Walsh and Lepor 9 ushered in an era of consciousness in regard to preservation of functional outcomes during radical prostatectomy. Multiple studies have since evaluated the effect that nerve preservation, prostate size, patient age, urethral length, and body mass index (BMI) have on recovery of continence. 10 –13 Few reports, however, have used preoperative endorectal MRI to predict continence after RARP. As such, we sought to take advantage of the precise anatomic prostatic and periprostatic detail that a 1.5 Tesla endorectal MRI provides to analyze anatomic predictors of continence after RARP.
Patients and Methods
Of our database of 970 RARP patients, 80 patients underwent preoperative 1.5 Tesla endorectal MRI. All patients had MRI to complete a staging workup. Urethral length, sphincter thickness, and prostate size were calculated on MRI (Table 1B). Urethral length was measured in the coronal plane, from the prostate base to the bulb. The external urethral sphincter thickness was measured in two dimensions, and the results were averaged. Prostate size was measured and volumes were calculated. MRIs were read preoperatively by radiologists who were blinded to information about the patient's continence preprocedure and postprocedure. Additional variables were nerve sparing, patient age, and BMI.
All patients underwent RARP by a single surgeon. All patients underwent a nerve-sparing technique. Questionnaires regarding pad used were completed by patients at monthly intervals. All patients were stress continent at baseline. We defined complete continence as the use of 0 pads per day (PPD); use of a security pad was considered social continence defined as use of 1 PPD. The primary end point that was analyzed was time to achieving 0 to 1 PPD.
Kaplan-Meier curves were used to compare time to continence between groups. The log-rank test was used to assess differences between curves. Univariate Cox regression analysis was used to examine the relationship between continuous variables and the outcomes. Prostate size and urethral lengths were examined as continuous variables. We also used univariate analysis to examine possible cutoffs for both prostate size (<40 vs ≥40 grams, <50 vs ≥50 grams, <60 vs ≥60 grams) and urethral length (<14 vs 14 cm, <16 vs ≥16 cm, and <20 vs ≥20 cm). Variables with P < 0.10 in the univariate analysis were included in multivariate models. In cases where the continuous and the categorical version of a variable were both significant at the univariate level, the version that was more significant was included in the model. Multivariate Cox regression analysis was used to determine independent predictors of achieving social continence or continence. P < 0.05 was considered statistically significant. Statistical analysis was performed using SPSS version 16.0 (SPSS, Inc. Chicago, IL).
Results
Demographic data for the 80 patients included in this study appear in Table 1A. Sixty (75%) patients achieved social continence at a median (interquartile range) time of 6.0 (8.0) weeks and 34 (45%) patients achieved complete continence at a median time of 9.5 (6.0) weeks.
SD = standard deviation; BMI = body mass index; MRI = magnetic resonance imaging.
Percentages may not sum to 100 because of missing data.
MRI = magnetic resonance imaging.
Results of the univariate analysis appear in Tables 2 and 3 and Figure 1. Prostate size was a significant predictor of time to social continence both when treated as a continuous variable (P = 0.01) and when categorized as ≥50 g vs < 50 g (P = 0.02). Median time to social continence was 6 weeks for patients with a prostate volume <50 g and 12 weeks for patients with prostate volume ≥50 g. Seventy-five percent of patients with prostates <50 g reached social continence at 3 months postoperatively vs 54% of patients with prostates ≥50 g (Fig. 1).
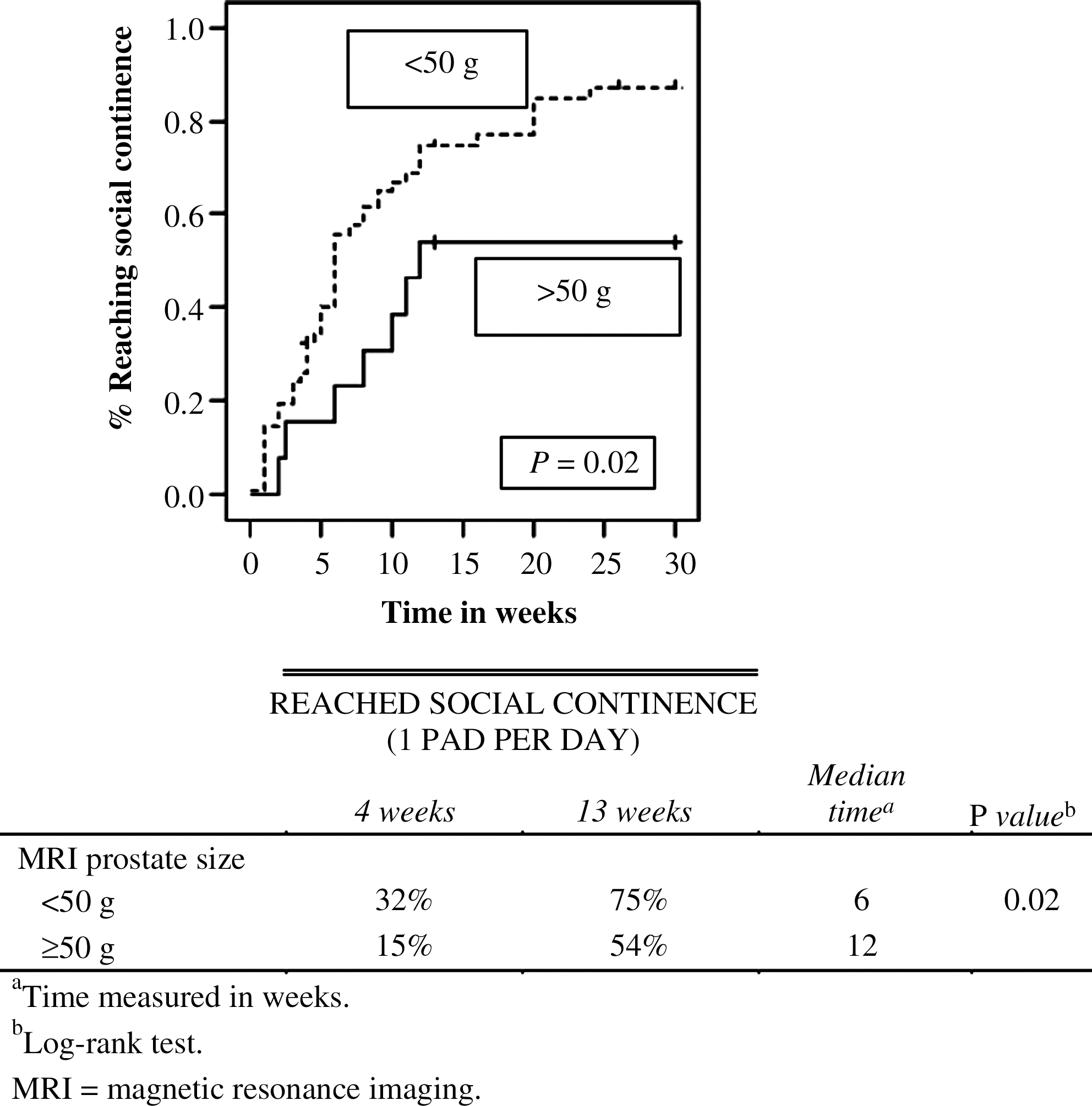
Kaplan-Meier analysis for MRI prostate size cutoff at 50 g (1 pad per day).
HR = hazard ratio; CI = confidence interval; BMI = body mass index; MRI = magnetic resonance imaging.
HR = hazard ratio; CI = confidence interval; BMI = body mass index; MRI = magnetic resonance imaging.
Prostate size also was a significant predictor of time to complete continence when treated as a continuous variable (P = 0.02) and when categorized as ≥50 g vs < 50 g (P = 0.02). The median time for patients with <50 g prostates to reach complete continence was 20 weeks while those with larger glands had not reached median time to continence after 30 weeks (Fig. 2).
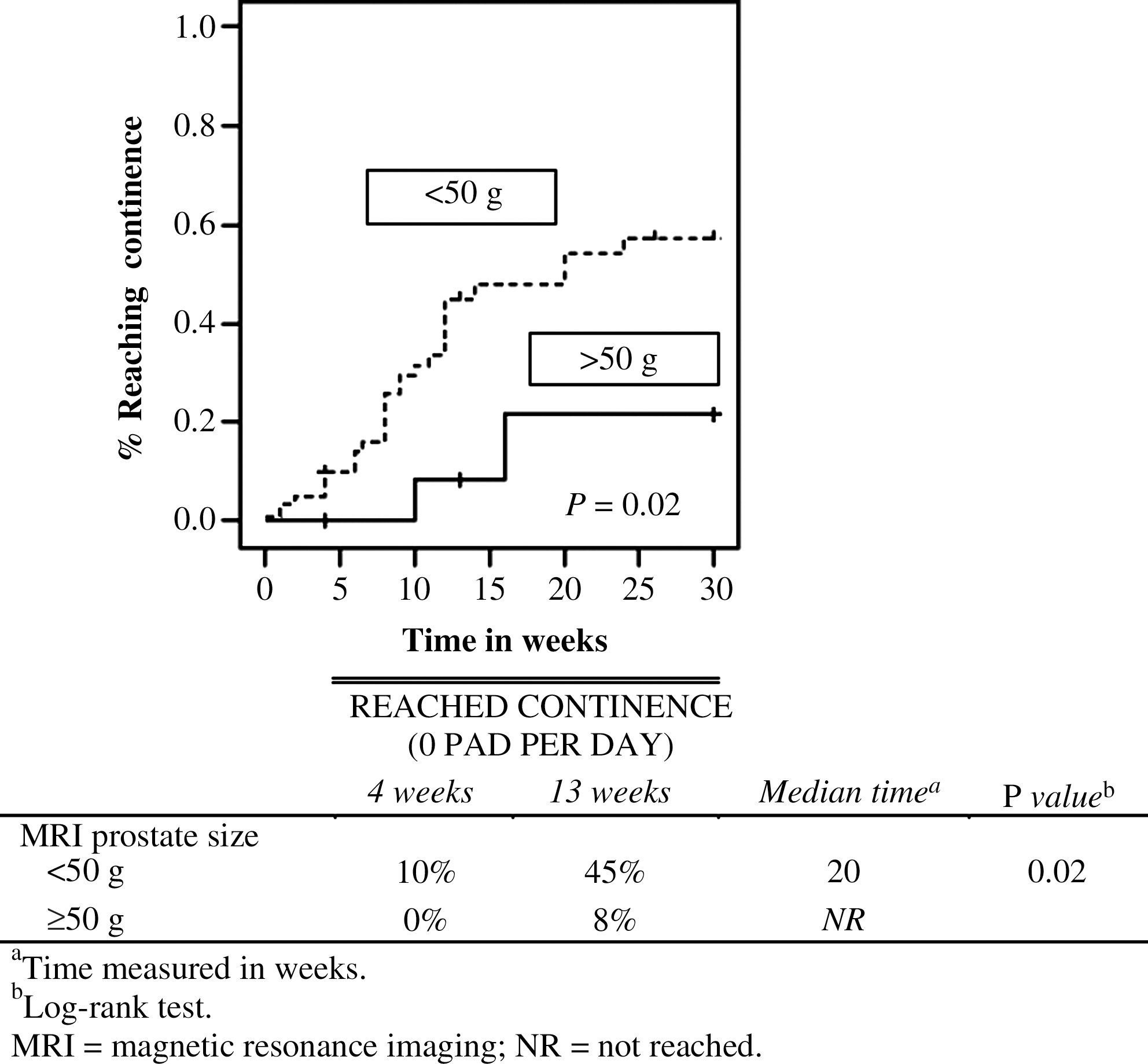
Kaplan-Meier analysis for MRI prostate size cutoff at 50 g (0 pad per day).
MRI urethral length was marginally related to time to continence when treated as a continuous variable (P = 0.06) and when categorized as ≥20 vs < 20 (P = 0.08). Patients with a urethral length of 20 mm or more had swifter return to total continence (Fig. 3). Thirty-four percent of patients with a urethral length <20 cm had reached continence at 3 months vs 52% of patients with a urethral length >20 cm who reached continence. Increased age was also a significant predictor of longer time to continence (P = 0.01).

Kaplan-Meier analysis for MRI urethral length cutoff at 20 cm (0 pad per day).
Tables 4A and 4B present the results of the multivariate Cox regression analysis. Independent variables were entered in the form most significant in univariate prediction. Multivariate analyses indicate that larger prostate size (HR 0.97; 95% confidence interval [CI] 0.95, 1.00; P = 0.04), and older age (HR 0.95; 95% CI 0.90, 0.99; P = 0.025) were associated with a longer time to achieve continence. Longer urethral length was associated with a decreased time to achieve continence (HR 1.10; 95% CI 1.02, 1.19; P = 0.01). Adjusting for age and prostate size, increased urethral length, as measured on MRI, was also significantly related to decreased time to continence; a 1 mm increase in urethral length was associated with a 10% increase in the likelihood of reaching continence at any time point. While controlling for age and MRI urethral length, patients with prostate volumes ≥50 g had 75% lower likelihood of achieving continence at any time point than did patients with <50 g prostates (HR 0.25; 95% CI 0.06, 1.06; P = 0.06).
Reference category.
HR = hazard ratio; CI = confidence interval; MRI = magnetic resonance imaging.
BMI and sphincter thickness were not significant determinants of urinary outcomes in this analysis. Degree of nerve sparing included minimal, partial, unilateral, and bilateral. Nerve sparing, if performed, was quantified as 50%, 75%, or >90%. Effect of nerve sparing was not included in the analysis.
Discussion
Our study provides evidence that increasing urethral length, measured by preoperative endorectal MRI, correlates with faster return to continence and a higher likelihood of achieving complete continence after RARP (HR 1.11 ; 95% CI 1.02, 1.20; P = 0.01). Our data confirm the work of Coakley and coworkers, 10 which showed that men with urethral lengths of ≥12 mm achieved continence significantly more often than those with shorter urethras at 1 year postoperatively (89% and 77%, respectively). We examined several urethral length cutoffs, however, and found only a length greater than 20 mm trended toward a swifter return to total continence (P = 0.08).
A follow-up study from Memorial Sloan Kettering again demonstrated the role of urethral length in continence preservation but also reported on postoperative length, suggesting that preservation of preoperative length is needed to speed recovery of continence. 11 Our study adds to their work and extends the preoperative endorectal MRI findings to robot-assisted prostatectomy.
Postoperative incontinence remains a major setback for many men undergoing prostatectomy. Despite advances in technique, 5% to 30% of men have some degree of incontinence after surgery, demonstrating the wide variation in surgical technique, surgeon experience, and definition of continence used by different authors. Currently, we have little objective way to predict which men will regain continence and how quickly they will do so. The use of routine preoperative endorectal MRI has become increasingly common in some academic practices, because it can be more precise, accurate, and less operator dependent than transrectal ultrasonography. 17 It also provides additional information about possible invasion into the capsule or periprostatic tissue.
If endorectal MRI imaging proves to be an accurate prediction tool, it will provide an additional variable to advise patients on the risk of postoperative complications. For some men who place a high value on achieving total continence and who have low-grade cancers, imaging information may allow them to choose a treatment modality that better serves their needs. If urethral length is short, this will not preclude a patient from pursuing RARP for his prostate cancer; however, it may provide him information about his individualized risk for stress incontinence postprostatectomy.
Our study also suggests that increasing prostate volume calculated by preoperative endorectal MRI correlates with a slower return to continence, and patients were less likely to achieve continence after RARP as compared to those with smaller glands (HR 0.97; 95% CI 0.95, 1.00; P = 0.04). Patients having preoperative prostate volumes of <50 g trended toward better continence achievement than those ≥50 g (HR = 0.25 [0.06, 1.06], P = 0.04). Furthermore, as demonstrated in Figure 2, 45% of patients with prostate sizes <50 g achieved complete continence at 3 months while only 8% of those with larger glands were pad free at 3 months (p = 0.02). Similarly, for social continence, 75% of patients with prostates <50 g were wearing 1 PPD at 3 months vs 54% for those with larger glands (P = 0.02). Prostate size can make robot-assisted prostatectomy more challenging, because of increased blood loss and operative time. 18 The etiology of postoperative incontinence is multifactorial, but nerve injury during more complex procedures may be contributing.
This is one of the earliest studies that have used MRI-measured prostate volume to specifically look at continence outcomes. It is true that prostate volume can be measured with transrectal ultrasonography preoperatively; however, MRI has already been used in some academic practices because of the advantages noted above. The volume determined by MRI has been shown to correlate highly with specimen weight. 18
While previous studies have suggested that prostate volume has little or no effect on continence postradical prostatectomy. 13,14,18 our results add to those of several other studies that also showed patients with larger prostates (≥50 g) took significantly longer to achieve postoperative continence after laparoscopic radical prostatectomy, 12,15 and studies that show both prostate size and age were predictors of continence. 16
Our study has a number of limitations. Only 80 of our patients who underwent preoperative assessment with endorectal MRI had appropriate follow-up, limiting the power to detect any small, yet significant differences. In addition, we were not able to obtain postoperative endorectal MRI images, which would have allowed us to evaluate the percent change of the urethral length and the presumed correlation between preoperative and postoperative urethral lengths. Furthermore, by using solely an imaging modality, our urethral and sphincter length measurements were also entirely anatomic.
In this study we used the expanded prostate cancer index composite, a validated questionnaire that assesses pad usage. There is sometimes a concern that even one PPD may not meet the definition of continence for some men. A study done by Lepor and colleagues 19 noted that men who indicated they use 1 pad daily ranged between those who use it for reassurance and those who used it for some degree of absorption. The majority of men in that study who wore 1 pad considered themselves continent, and it was thought that these men were using the pad primarily for reassurance.
Obtaining functional measurements of the sphincter length through urodynamic flow studies may yield additional information beyond MRI studies alone. In addition, performing postoperative endorectal MRI to determine the association between preoperative and postoperative urethral lengths would be helpful. Obtaining these studies in a large group of patients, however, will likely be difficult because of cost and the invasive nature of the test. Further investigation is also necessary into the multitude of techniques used to repair the sphincter complex during RARP.
Conclusion
Longer urethral length increased the likelihood of achieving continence at any time point. Increasing age and larger prostate size were negatively associated with achieving continence. Further research may look to determine the relationship, if any, between the anatomic measurement of urethral length and urodynamic findings, both before and after surgery.
Footnotes
Disclosure Statement
No competing financial interests exist.