
Abstract
Purpose:
Our aim was to determine the optimal size of access sheath for ureteroscopy and stone lasertripsy to achieve good irrigant flow while maintaining the lowest possible intrarenal pressure.
Materials and Methods:
We used an in vitro anatomic model into which a pressure transducer was incorporated. Cook Peel-Away 10F, Flexor 12F, 14F, 16F single lumen, and a new 14F Flexor dual-lumen sheath were tested. Irrigant flow and intrarenal pressure were measured with an empty ureteroscope working channel and with a 1.4F or 2.4F basket within the working channel with a hydrostatic pressure of 1 m and 2 m, respectively. For the dual-lumen sheath, the irrigation was either connected to the scope or the second channel of the access sheath. Two other configurations were tested: 4F ureteral catheter placed alongside a 10F sheath (configuration 1) or a 5F ureteral catheter within a 16F access sheath (configuration 2).
Results:
With an empty working channel, irrigant flow increased with sheath diameter. The presence of a 1.4F or 2.4F basket, however, reduced flow up to 65% and 90%, respectively. Increasing the hydrostatic column to 2 m height improved the irrigant flow but with a predisposition to a higher intrarenal pressure. Using configurations 1 and 2, the flow rates improved by 250% and 700%, respectively, with a 2.4F basket in the working channel, and could also be used with a 2 m hydrostatic column without raising the intrarenal pressure.
Conclusions:
Increased access sheath diameter does not improve flow when the working channel of a flexible ureteroscope is occupied. Our proposed configuration of a ureteral access catheter placed inside or alongside the access sheath provides by far the highest flow rates without a rise in the intrarenal pressure.
Introduction
The aim of our study was to determine the optimal size of access sheath for ureteroscopy and stone lasertripsy to achieve good irrigant flow while maintaining the lowest possible intrarenal pressure. We investigated the effect of different diameter ureteral access sheaths on the flow of irrigant through an in vitro renal model and also looked at the effect of different irrigation configurations on the flow through it. In addition, we also analyzed the effect of different sizes of baskets on the flow rate through this system. Image analysis was performed using a standardized colloidal solution to quantify the effect of improved flow on image resolution through a flexible ureteroscope. Finally, the influence of the above parameters on intrarenal pressure was investigated.
Materials and Methods
An in vitro polymer anatomic model of a kidney and upper ureter (Fig. 1) was created by rapid prototyping. The model consisted of a renal pelvis, two paired lower and middle calices set at 90 degrees, an upper calix, and 5 cm of upper ureter. A pressure transducer and a contrasting target marker was incorporated into the upper calix. The model incorporated a sealable collar around the ureter through which a ureteral access sheath could be passed, providing a watertight seal. A standard Storz Flex-X™ flexible ureteroscope, 7.5F, was passed along the access sheath into the midpoint of the renal pelvis, 4 cm from the end of the access sheath. A standard Flowfusor® irrigation system with water was connected to the ureteroscope with an initial 1 m hydrostatic head.

In-vitro polymer anatomic model of a kidney and upper ureter.
The main outcome measures were flow rate through the system measured as drainage from the distal end of the access sheath and intrarenal or intrapelvic pressure as measured at the upper calix. These parameters were measured with an empty ureteroscope working channel and with a 1.4F or 2.4F basket within the working channel of the scope.
Cook Silhouette™ Peel-Away® 10F, Flexor® 12F, 14F, 16F single lumen and a new 14F Flexor® dual-lumen sheath were tested. Irrigation was connected directly to the working port of the ureteroscope. In the case of the dual-lumen sheath, measurements were taken with the irrigation connected either to the scope directly (configuration 1) or to the second smaller channel of the access sheath (configuration 2). In addition, two alternative irrigation configurations were tested with the single-lumen access sheaths; namely, with irrigation connected to a 4F open access ureteral catheter placed alongside a 10F sheath or a 5F open access catheter that was placed within a 16F access sheath. Three runs were carried out with each configuration over 5 minutes. These experiments were conducted sequentially with both 1 m and 2 m hydrostatic columns.
To demonstrate that improved irrigation flow through the system correlated with greater clarity of vision, image analysis was used. This was performed using image capture of stills of a contrasting target taken via the ureteroscope at regular time intervals within the renal pelvis after the introduction of a standard solution of titanium oxide colloid. Captured images were converted to grayscale.bmp files for analysis. The converted .bmp files had a line of interest plotted that traversed the target and was the same in each image series to ensure comparability. A higher grayscale value equated to greater target resolution. The mean grayscale value was plotted against time after introduction of the colloid into the system. A faster recovery of grayscale value equated to a more rapid recovery of image resolution with irrigant flow.
Results
With an empty ureteroscope working channel, flow through the system generally increased with wider sheath diameters in a nonlinear manner (Fig. 2), the exception being the 10F Silhouette access sheath, which was superior to the 12F Flexor access sheath. This was because the 10F Silhouette sheath had a wider internal channel diameter than the 12F reinforced Flexor sheath (Table 1). There was a difference of 580% in flow rate between the maximum and minimum flow rates achieved between different sheaths (141 mL/5 min with a 16F Flexor vs 23 mL/5 min for a 12F Flexor access sheath). With a 1.4F or 2.4F basket in the ureteroscope working channel with a 16F Flexor access sheath, the flow rate was reduced by up to 65% (141 mL/5 min to 49 mL/5 min) and 90% (141 mL/5min to 17 mL/5 min), respectively compared with an empty channel (Fig. 2). Larger diameter access sheaths were associated with the largest percentage falls in flow with a 1.4F or 2.4F basket within the working channel compared with an empty channel. With the 2.4F basket in situ, there was little absolute difference in flow rates between different access sheath diameters (range 10.0–22.0 mL/5 min).
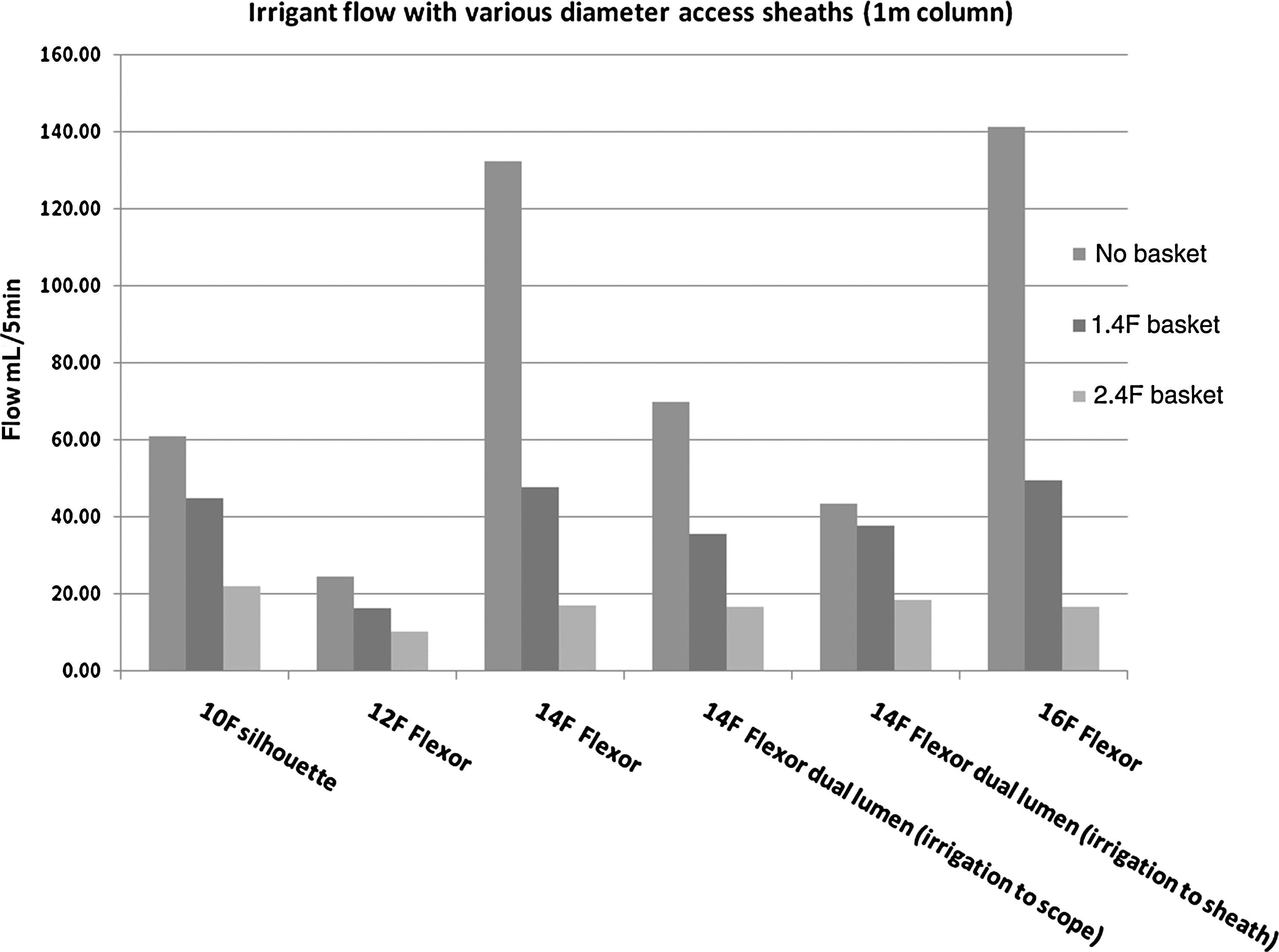
Irrigant flow through various access sheath configurations—no basket, 1.4F basket, and 2.4F basket at 1 m column height.
With a hydrostatic column of 1 m, the intrarenal pressure measurement for most of the sheath and working channel irrigation configurations was less than 20 mm H2O, the minimum detection limit of the equipment. The 12F Flexor sheath, however, consistently gave intrarenal pressures above this threshold of between 29 cm H2O (2.4F basket) and 57 cm H2O (empty channel). In addition, when the irrigation was connected to the secondary lumen of the 14F Flexor dual-lumen access sheath, an intrarenal pressure of 38 cm H2O was measured with the 2.4F basket in situ (Fig 3).

Access sheath configuration associated with intrarenal pressure >20 cm H2O at 1 m column height. dl = dual lumen.
The two tested configurations in which irrigation was connected to a separate ureteral catheter running alongside the access sheath were not associated with higher system flow rates when the working channel of the ureteroscope was empty. Flow rates with a larger instrument within the working channel of the scope, however, were markedly improved over any of the previously tested configurations. The use of a 5F open-ended ureteral catheter for irrigation within the 16F sheath provided flow seven times greater (122 mL/5 min vs 17 mL/5 min) than any other configuration with a 2.4F basket in situ (Fig. 4). A 4F catheter alongside a 10F sheath provided flow 1.9 times greater (42 mL/5 min vs 22 mL/5 min) than with the irrigation connected to the scope with a 2.4F basket in situ.

Irrigant flow with 10F access sheath and 4F ureteral catheter alongside, and 16F access sheath with 5F ureteral catheter within the access sheath at 1 m column height.
Raising the hydrostatic column to 2 m resulted in improvement to the system flow by approximately 200% as might be expected (Fig. 5). There was no change in the order of configurations associated with the best and worst flow, however. In addition, predisposition to higher intrarenal pressures was seen with the 12F Flexor and 14F dual-lumen access sheaths with peak measured pressures in excess of 100 mm H2O (Fig. 6).

Irrigant flow through various access sheath configurations—no basket, 1.4F basket, and 2.4F basket at 2 m column height.
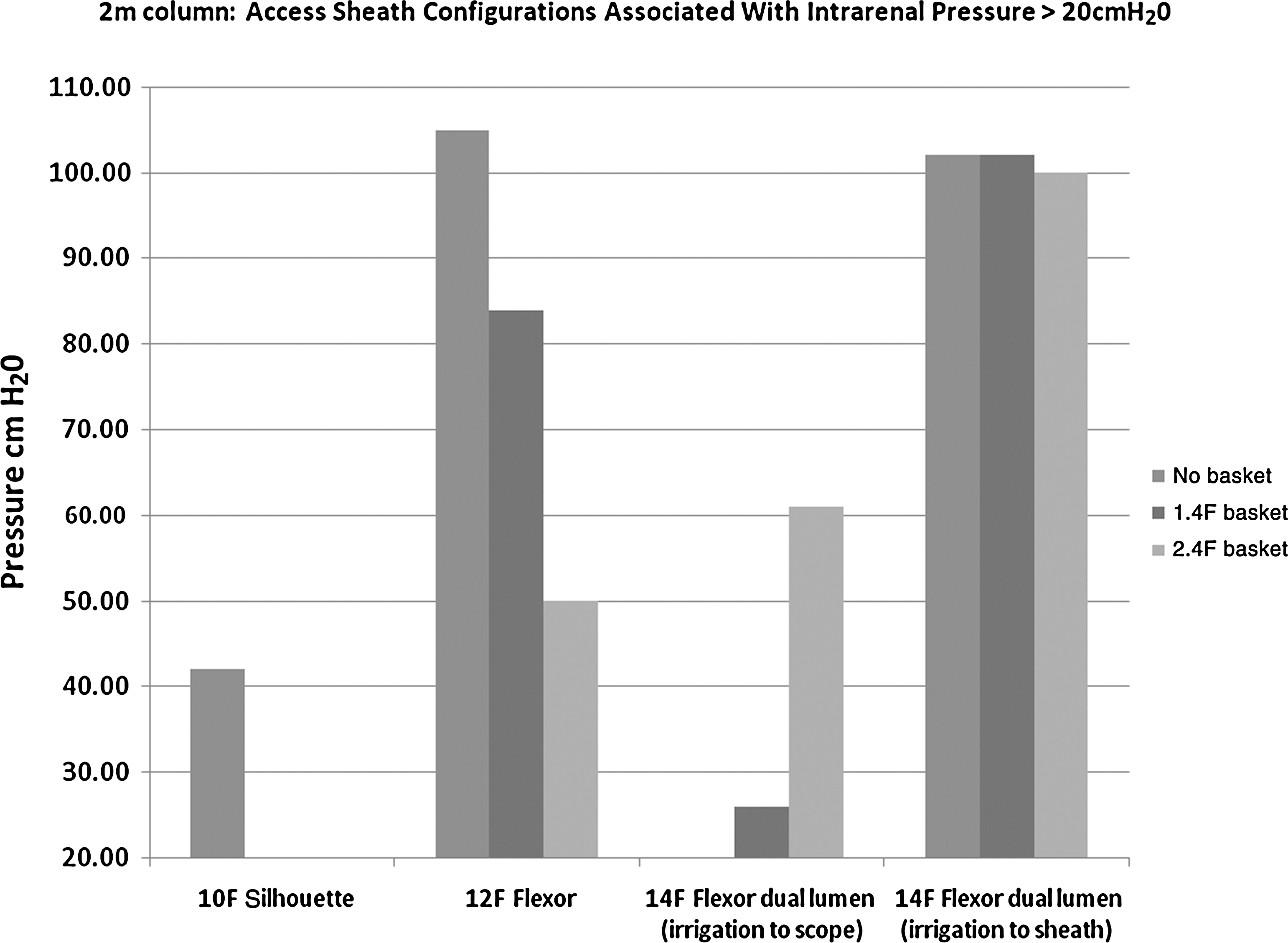
Access sheath configuration associated with intrarenal pressure >20 cm H2O at 2 m column height.
Image analysis was carried out with the two sheath configurations yielding the highest and lowest flow rates; namely, the 16F Flexor sheath with an empty ureteroscope working channel and a 2 m hydrostatic column vs the 14F dual-lumen sheath, a 2.4F basket within the ureteroscope working channel, and a 1 m hydrostatic column. The recovery of image resolution after introduction of colloid for both scenarios is shown in Figure 7. It can be clearly seen that recovery to baseline greyscale value and, hence, image resolution is approximately five times faster for the optimal access sheath configuration associated with the best flow.

Recovery of image resolution after introduction of colloid for 16F Flexor sheath with an empty ureteroscope working channel and a 2 m hydrostatic column (best flow rate configuration) vs the 14F dual lumen sheath, a 2.4F basket within the ureteroscope working channel, and a 1 m hydrostatic column (poorest flow rate configuration).
Discussion
Principal findings
Our results demonstrated that increasing the diameter of an access sheath alone improved flow up to sevenfold (12F Flexor vs 16F Flexor) during flexible ureteroscopy, provided that the working channel of the scope was empty. This size effect was less pronounced with a 1.4F basket in the working channel and further diminished with a 2.4F basket in situ.
The commonly used technique of raising the hydrostatic column to improve flow was indeed associated with improvement in flow, regardless of access sheath configuration. These improvements, however, in absolute terms with regard to an occupied ureteroscope working channel, were small and may not be beneficial in a clinical setting. In addition, intrarenal pressures were demonstrated to be higher with a raised hydrostatic column, which could potentially be significant in a clinical setting in terms of potential bacterial translocation or renal impairment.
Meaning of the study
In a typical working situation with a basket or, indeed, a similar sized laser fiber in place, there appears to be little benefit in using a larger diameter access sheath. The detrimental effect of suboptimal flow on vision through the ureteroscope is self-evident clinically, and we saw this using image capture techniques with a fivefold increase in time taken to clear a clouded visual field between optimal and poorest configurations.
The tested Flexor 14F dual-lumen sheath did not seem to provide any significant improvement in flow. When an attempt was made to improve flow by connecting the irrigation to the second channel of the access sheath, a significant rise in intrarenal pressure was seen while flow improved by only 10%.
The two novel alternative configurations for ureteroscopy using a ureteral access catheter purely for irrigation in addition to a single-lumen access sheath were found to improve flow rates by up to 250% and 700%, respectively, with a 2.4F basket occupying the working channel of the scope (Fig. 4). This was achieved while keeping intrarenal pressures below 20 mm H2O. The optimum configuration in terms of flow was with the use of a 16F access sheath with a 5F open access ureteral catheter placed within the sheath for irrigation. The alternate, more practical option was using the smaller 10F flexible access sheath with a 4F open-ended ureteral catheter for irrigation placed outside of the sheath. Both of these configurations could be used with a higher 2 m hydrostatic column without raising intrarenal pressures above the threshold 20 mm H2O level.
A 2.4F basket equates to a 0.8 mm diameter. A typical 365 μm laser fiber used for lasertripsy has an outer core diameter of approximately double that of the inner core (0.73 mm), and so results using the larger basket should be applicable to the use of a typical laser fiber.
Weaknesses of the study
The main limitations of this study are related to its in vitro design. This enabled us, however, to create a realistic controllable environment that allowed the reproducible investigation of parameter changes on the outcomes of irrigant flow and intrarenal pressure. We have not factored the deflection of the scope during ureteroscopy. Scope deflection with an instrument in the working channel of a scope can reduce flow by 62% to 90%. 5 This further reinforces the need to develop ways to improve irrigant flow during ureteroscopy.
Strength and weakness of the study in comparison with other studies
The sizes of stone baskets are inversely proportional to the irrigant flow. 6,7 As with our study, the use of the access sheath was seen to cause a decrease in intrapelvic pressure and an increase in irrigant flow. 3,4 Newer radially dilating ureteral access sheaths have undergone trials in a porcine model and shown to have a better flow rate and lesser urothelial trauma compared with standard sheaths and are undergoing human trials. 8 Larger diameter sheaths have been shown to decrease ureteral blood flow by up to 65%, 9 and although not shown to increase the ureteral stricture rate clinically, this remains a potential concern with longer procedures because of ischemic injury. 10 With the use of larger diameter access sheaths, there appears to be a transient drop in ureteral blood flow that returns to baseline intraoperatively, not resulting in any histologic ischemic damage. 9 Although a formal cost-effectiveness analysis has not been performed, results seem to favor the use of the access sheath because it decreases the overall cost by reducing operative time. 11
Conclusion
Increasing the access sheath diameter does not improve intrarenal irrigant flow when the working channel of a flexible ureteroscope is occupied with a basket. We have proposed two configurations that improve irrigant flow with a larger basket in situ while maintaining low intrarenal pressures. Specifically, a 10F Peel-Away sheath used in conjunction with a 4F ureteral access catheter for irrigation inflow placed alongside is to be recommended for virtually all cases. Where conditions are favourable, the use of a 5F ureteral access catheter for irrigation placed inside a 16F access sheath provides by far the highest flow rates.
Raising the hydrostatic column to 2 m improves irrigant flow but could increase the intrarenal pressure to above 20 mm H2O in some situations. The commonly used 12F Flexor sheath is less favorable in terms of irrigant flow than other tested sheaths and may be associated with comparatively higher intrarenal pressures when the hydrostatic column is raised above 1 m.
Footnotes
Acknowledgment
We would like to thank Cook Medical for providing the ureteral access sheaths and catheters as well as an educational grant. We thank Storz endoscope for the loan of the Flex-X ureteroscope.
Disclosure Statement
No competing financial interests exist.