
Abstract
Purpose:
To describe the safety and feasibility of a running urethrovesical anastomosis (UVA) in robot-assisted radical prostatectomy (RARP) using a unidirectional self-locking barbed suture.
Patients and Methods:
Fifty-one consecutive patients with organ-confined prostate cancer underwent RARP by one of two experienced surgeons. UVA was performed in two layers, using a unidirectional barbed suture fashioned into a double-ended stitch. Perioperative outcomes and 30-day complications were recorded.
Results:
All anastomoses were performed without assistance and without tying a knot. Median time for entire dual-layer anastomosis was 14.0 minutes (interquartile range [IQR]: 12–20) and that for urethrovesical anastomosis was 11 minutes (IQR: 9–15). Not having to rely on an assistant to follow the suture decreased instrument clashes, entangling of the suture around an instrument, and made the anastomosis faster. Eight patients underwent anterior/lateral reconstruction of the bladder neck, and there were no leaks on cystography at 1 week.
Conclusions:
We describe the first reported clinical experience with a novel technique of performing UVA during RARP that is safe and efficient. Using the barbed wound closure device prevents slippage, precluding the need for assistance, knot tying, and constant reassessing of anastomosis integrity.
Introduction
Limitations of the Van Velthoven stitch relate primarily to slippage of the monofilament suture and loosening of the loops. This slippage necessitates constant traction by an assistant or repeated tightening of the suture by the surgeon to prevent loosening of the suture and consequent anastomotic leaks. This prolongs anastomotic times and increases risk of instrument clashes and suture tears of the urethra. Modifications have been proposed to address these issues, 4,5 each with limitations.
We present a novel technique of UVA using a unidirectional barbed suture (V-Loc™ absorbable wound closure device, Covidien, Mansfield, MA). To our knowledge, this is the first report of a barbed suture being used for UVA in humans. The V-Loc barbed wound closure device is a unidirectional, self-anchoring barbed suture composed of an absorbable copolymer of glycolic acid and trimethylene carbonate (polyglyconate). First given Food and Drug Administration approval in March 2009 for soft-tissue closure, it was initially studied in skin closure. Subsequent studies on porcine enteric anastomoses demonstrated closure equivalence with maxon (monofilament polyglyconate) but faster anastomosis times. 6 We postulated that using a self-locking suture for UVA would ameliorate drawbacks of traditional monofilament sutures and make UVA during minimally invasive radical prostatectomy easier and more efficient.
Patients and Methods
Fifty-one consecutive patients undergoing RARP (Vattikuti Institute prostatectomy) by one of two experienced robotic surgeons underwent dual-layer UVA with the V-Loc barbed suture. All patients were counseled regarding the use of the barbed suture for UVA, and written informed consent was obtained.
A single 6-inch, barbed 2-0 polyglyconate suture on a tapered 17 mm (RB-1) needle was used to approximate the Denonvilliers fascia and the periurethral tissues. The UVA suture was preprepared from two similar 6-inch sutures by running the needle of each suture through the looped end of the other suture, thereby creating a sturdy, bidirectional, barbed suture with two needles (Fig. 1). This 12-inch composite suture was then used to perform the anastomosis as described previously. 7
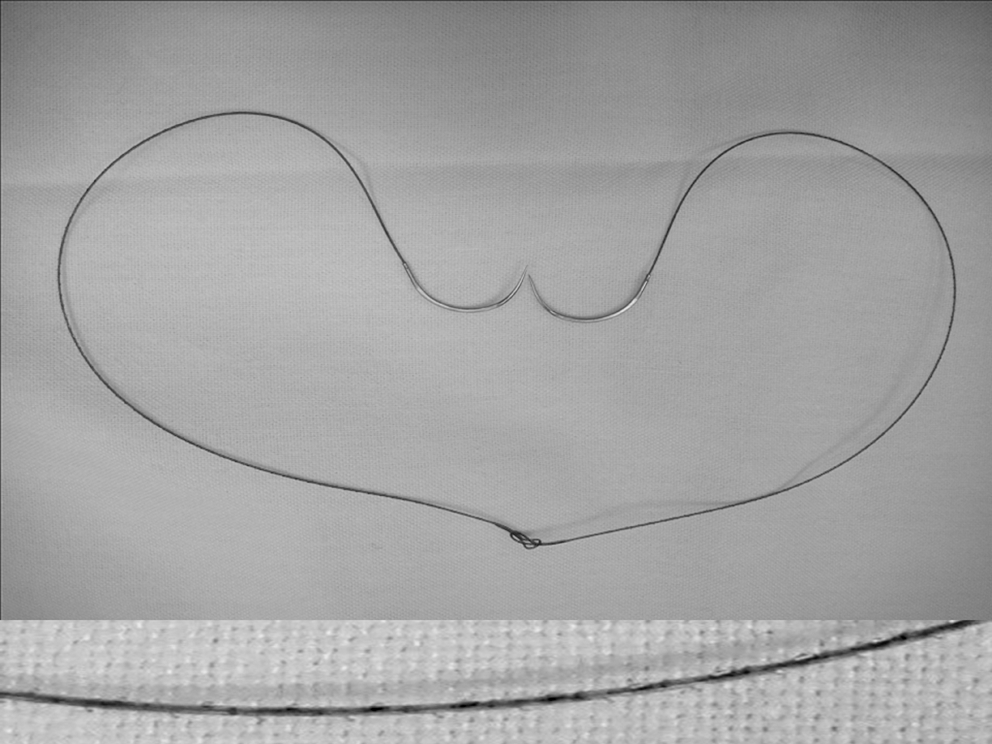
Double-ended barbed suture. The inset (at bottom) shows a magnified view of the barbs on the suture.
The first three throws, beginning at the 5 o'clock position, along the posterior urethra and bladder neck are placed before attempting to approximate the two structures (Fig. 2). The left side of the anastomosis is completed in a running fashion until 12 o clock. After each set of throws through the bladder neck and urethra, the suture is tightened down. The barbs hold the suture and prevent slippage and recoil. It is unnecessary for the assistant to follow the suture or place traction on it. The right side of the anastomosis is completed with the other half of the double-ended stitch. The first two throws on the bladder neck are performed “backhand” to ensure a watertight closure in the posterolateral region of the anastomosis (Fig. 3).
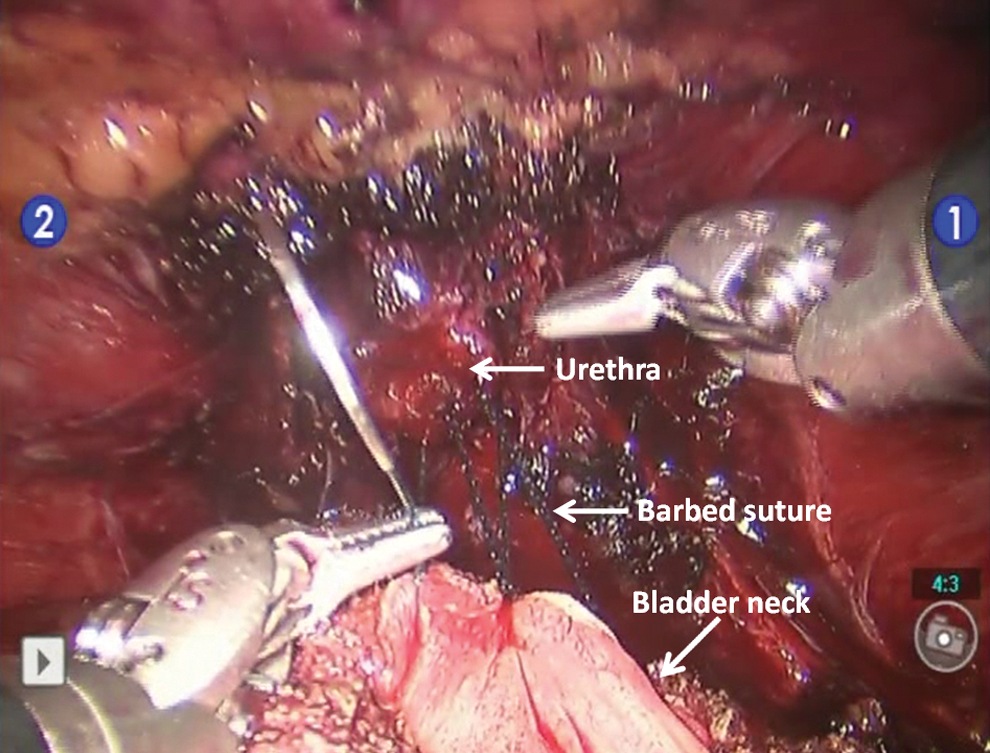
Three throws of barbed suture placed through bladder neck and urethra. The bladder neck is about to be approximated to the urethra.
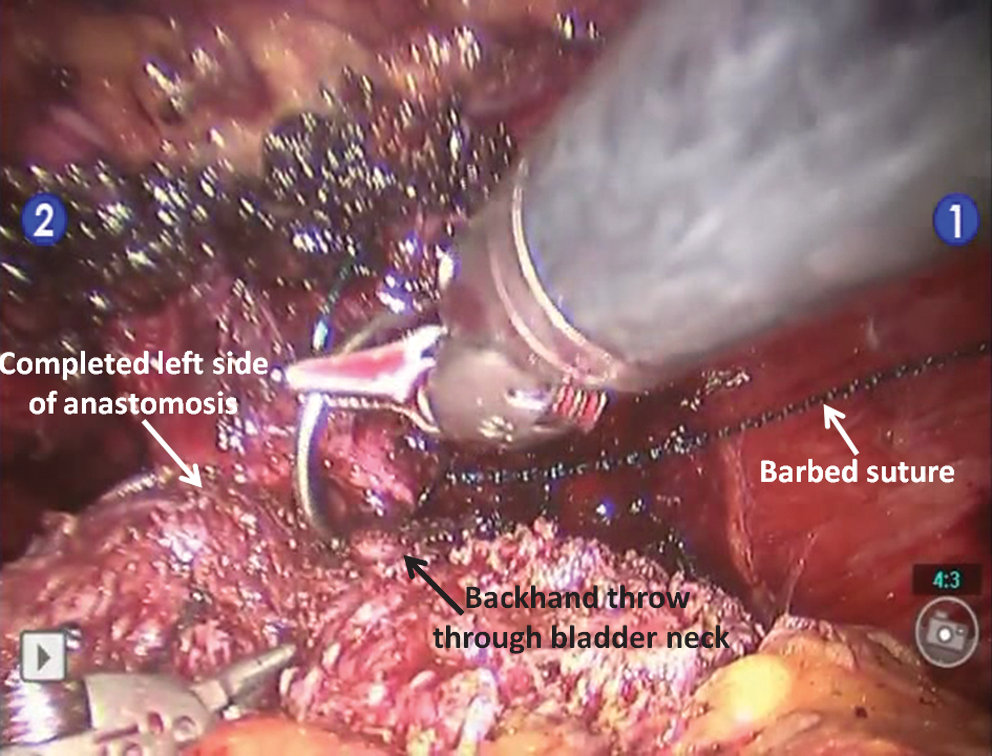
The posterior and left side of the anastomosis has been completed. First stitch of the right side of the anastomosis using a backhand throw.
At the conclusion of the anastomosis (Fig. 4), it is not necessary to tie a knot, and the two needles are simply cut; the barbs hold the suture in place and prevent loosening of the UVA. Integrity of the anastomosis was tested intraoperatively by instilling 240 mL of saline in the bladder. Cystography was performed at 7 days, and any extravasation of contrast was noted.
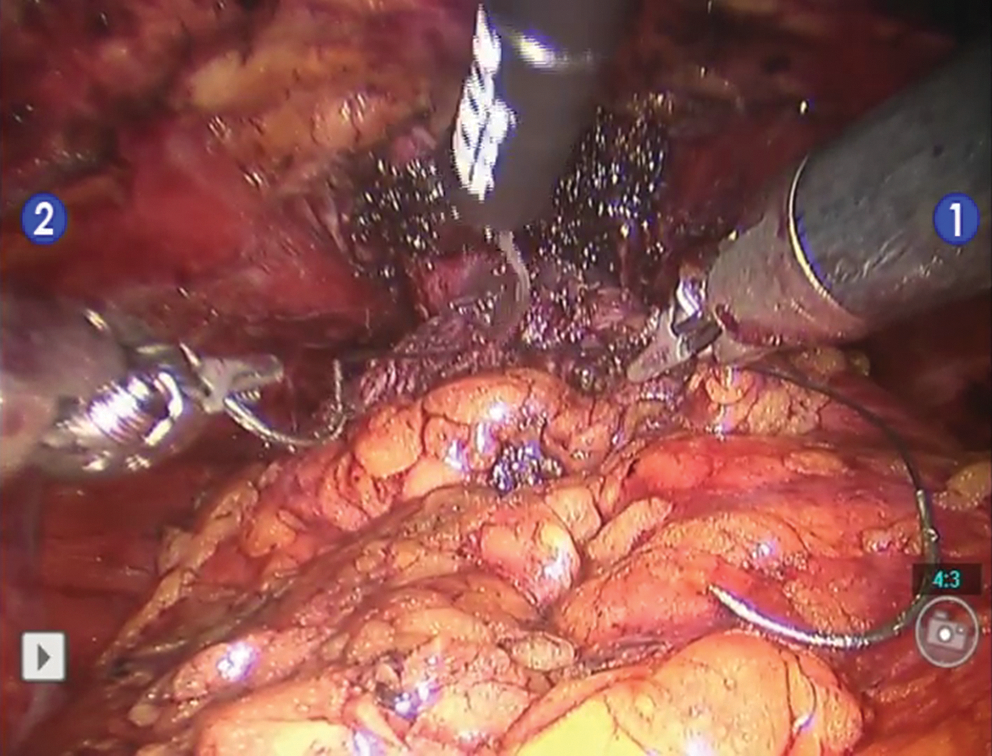
Anastomosis is completed. The two sutures are cut without having to tie a knot.
Preoperative, demographic, and perioperative data were recorded prospectively (Table 1). Intraoperative adverse events (including shearing of the urethra or bladder neck, need for revision of the anastomosis, and intraoperatively detected anastomotic leaks) and postoperative complications (especially cystography-detected extravasation of contrast, episodes of urinary retention and anastomotic strictures) were recorded. All patients were followed for at least 1 month.
SD = standard deviation; BMI = body mass index; PSA = prostate-specific antigen; IPSS = International Prostate Symptom Score; SHIM = Sexual Health Inventory for Men.
There were two important differences, however, between the traditional technique and our method: The patient side assistant did not follow the suture or provide any help with the anastomosis (except for moving the catheter tip in and out), and the two sutures were not tied at the conclusion of the anastomosis but merely continued across the anastomosis for one additional throw. If considerable discrepancy was noted in the diameter of the bladder neck and urethra, an anterior or lateral bladder neck reconstruction was performed again using the barbed suture.
Results
All anastomoses were completed by the console surgeon independently, without any assistance whatsoever from the patient side assistant. Specifically, the assistant or surgeon did not provide traction on the suture during anastomosis. Each throw was pushed down by the surgeon, and the barbs held the suture in place without any loosening of suture loops. The median time for UVA was 11 minutes (interquartile range [IQR], 9–15) including the time for bladder neck reconstruction, with 45% performed in 10 minutes or less. The median time for posterior reconstruction was 4 minutes (IQR, 3–6). Eight (16%) patients needed anterior bladder neck reconstruction that was performed by extending the anastomotic suture across the anterior bladder neck in a figure of eight pattern. Subjectively, the suture did not shear through the bladder neck or urethra. No patients had either intraoperative or cystography-detected urinary leak, and there were no episodes of urinary retention after removal of the catheter (Table 2).
Did not require anastomosis to be redone.
SD = standard deviation; IQR = interquartile range; UVA = urethrovesical anastomosis.
Discussion
RARP has undergone numerous modifications over the past 8 years, with UVA second only to nerve sparing in terms of degree of scrutiny. Van Velthoven and associates 2 described using two 6-inch monofilament sutures of polyglycolic acid tied together at the ends. This composite suture was then used to perform a running anastomosis that was watertight, reproducible, and efficient. In their initial experience, anastomosis times ranged from 14 to 80 minutes. 8
Modifications to UVA have been made in pursuit of increased efficiency while preserving safety and anastomosis integrity. One characteristic of the traditional monofilament suture is its tendency to slip, leading the surgeon to retighten the anastomosis with every throw and revisit each throw several times throughout the anastomosis to assure integrity. Assistants have been used to hold the suture in place between throws, 9 but this necessitates experienced assistants performing delicate retraction. To avoid posterior slippage, tearing of urethral tissue, suture breakage, and postoperative urinary leakage, Ball and colleagues 5 described using a Lapra-Ty to hold the posterior approximation tight. Berry and coworkers 4 described using three posterior interrupted sutures for the same purpose. Drawbacks of the preceding techniques include reliance on the assistant, foreign bodies adjacent to the urethrovesical anastomosis, and sutures tied within the bladder, respectively. Complications of Hem-o-lok clips used in close proximity to the UVA have recently been reported. Clip migration into the bladder has been associated with bladder neck contractures, 10 irritative voiding symptoms, 11 and stone formation. 12
We used two unidirectional barbed sutures to fashion a double-ended suture similar to one described by Van Velthoven and associates. 2 This is used to complete the anastomosis and any bladder neck reconstruction, if needed. Our technique eradicates most of the vexing challenges of performing the UVA. The barbed suture prevents slippage and obviates the need for assistance, as well as the frequent revisiting of each throw. The barbs also perform the function of Lapra-Ty and Hem-o-lok clips without introducing a foreign body into the area of the anastomosis. In addition, no knots are tied intracorporally.
Not having to rely on an assistant to follow the suture decreases the risk for instrument clashes, suture entanglement, and inadvertent breakage of the suture and tearing of the urethra. It also makes the anastomosis faster and more efficient. This advantage is likely to be most apparent to the inexperienced robotic surgeon in not having to use an assistant and to the experienced surgeon by significantly shortening the anastomotic times. In a comparative study performed at our institution, 36 consecutive patients each underwent UVA using the barbed suture and monofilament polyglecaprone, respectively. We noted a 27% reduction in time taken for a double-layer anastomosis (21.8 min vs 15.9 min), which was statistically significant. There were no differences in other perioperative outcomes or adverse events. 13 Moran and colleagues 14 used the barbed suture to perform UVA in an inanimate model and demonstrated that anastomosis with the barbed suture was faster, with no difference in subjective assessment of the quality of the anastomosis. Similar results have also been reported by Demyttenaere and coworkers 6 in using the V-Loc suture for bowel anastomoses in pigs.
Hypothetical concerns with this suture include excessive inflammation caused by the barbed suture, tearing of tissues, and strangulation or overtightening of the anastomosis, presenting as anastomotic strictures or prolonged urinary retention. Weld and associates 15 noted significantly higher lamina propria fibrosis and perianastomotic fat fibrosis, but no differences in muscle fibrosis and granulation tissue with the polydiaxonone barbed sutures (Quill,™ Angiotech, Vancouver, BC) compared with polyglactin (Vicryl,™ Ethicon, New Brunswick, NJ) sutures when used for bladder neck anastomosis in pigs. There was also no difference in inflammatory response with the same two sutures when used for pyeloplasty. They concluded that additional studies would be necessary to evaluate the clinical significance of the excessive fibrosis with the barbed stitch.
The suture we describe is composed of polyglyconate, which is different from the polydiaxonone suture that Weld and colleagues 15 used for their study. It is unclear, however, whether suture composition or barbs are responsible for the inflammatory response.
Other investigators have not seen any evidence of excessive inflammation with either the Quill or the V-Loc suture. Rodeheaver and coworkers 16 and Leung and associates 17 compared the inflammatory response of barbed suture with conventional monofilament suture in porcine and canine dermis, rat abdomen, and rabbit muscle. A composite score was assigned based on the degree of necrosis, coagulative necrosis, floccular degeneration, inflammation, neutrophils, lymphocytes, plasma cells, macrophages, fibroendothelial proliferation, fibrosis, giant cells, fatty infiltration, and relative size of the involved area. They found no differences between the barbed and conventional suture in any of the aforementioned sites. Demyttenaere and associates 6 performed a randomized controlled trial of V-Loc and polyglyconate (Maxon,™ Covidien, Mansfield, MA) sutures for gastrointestional anastomosis in pigs; on histopathologic evaluation of the anastomoses at 3, 7, and 14 days, they found no evidence of any difference in the inflammatory response between the two sutures. We have not seen prolonged urinary retention, urinary tract infections, or anastomotic strictures in any of our patients, although our maximum follow-up is only 3 months. We continue to monitor these patients closely for evidence of bladder neck fibrosis.
One important drawback is that since the barbs do not allow the suture to be retracted once placed through tissues, any mistake in placing throws would necessitate the suture to be cut and anastomosis to be redone. As a safety precaution, the first inch of the suture is without barbs, and if a technical misstep is recognized early (before the barbs are pulled through), the needle can be retracted and the suture replaced without adverse effects. No patients in our study needed the suture to be cut and anastomosis redone for this reason; however, this fact should be kept in mind while using this suture.
We wish to emphasize that our results are early outcomes and, while there have been no short-term adverse sequelae, long-term results still need to be borne out with additional follow-up. Although this suture has been in widespread use by plastic surgeons for fascial closures, face-lifts, and tendon repairs without complications, our report represents the first clinical use for anastomosis. As of the writing of this article, this technique has been used in more than 100 patients and is the standard of care for UVA during minimally invasive radical prostatectomy at our institution.
Conclusion
We present the first clinical application of a barbed self-locking suture for UVA during RARP that is safe and efficient at 3 months follow-up. Using this novel technique addresses many of the limitations of current techniques, obviates the need for assistance, prevents slippage, and allows for a knotless anastomosis. Long-term follow-up is necessary to evaluate the potential for fibrosis.
Footnotes
Disclosure Statement
No competing financial interests exist.