
Abstract
Introduction:
Relaxing the ureter prior to endourologic procedures could ease instrument access. In an ex-vivo model, intraluminal nifedipine has been shown to relax the ureter. Chitosan is the deacetylation product of chitin and can alter bladder urothelium. This study examines the effect of nifedipine on peristalsis before and after pretreating the ureter with chitosan.
Methods:
Intact 4-cm tubular porcine ureteral segments were placed in a novel organ bath. To induce peristalsis, phenylephrine (10 μM) was added. Chitosan (0.5% [w/v], 30 minutes) or Krebs (control) was then used to treat the urothelium. The rate and amplitude of ureteral peristalsis was then measured. Intraluminal nifedipine (1 μM) was then added to the intraluminal reservoir. Peristaltic rate and amplitude and the time to aperistalsis were measured. Methylene blue was then added after treatment with chitosan or control to measure diffusion.
Results:
After Krebs pretreatment, intraluminal nifedipine (1 μM) significantly reduced peristaltic frequency (p = 0.0184) but did not stop peristalsis after 60 minutes of exposure in six trials. After chitosan, nifedipine (1 μM) stopped ureteral peristalsis within an average of 12.30 ± 4.72 minutes. Chitosan alone did not cause aperistalsis. Intraluminal methylene blue did not diffuse into the extraluminal bath after saline or chitosan pretreatment. Histological analysis of the ureter before and after pretreatment with chitosan showed no urothelial disruption.
Conclusions:
By pretreating the intraluminal surface of the ureter with chitosan, nifedipine blocks ureteral peristalsis at low concentrations. Chitosan changes ureteral urothelial permeability without barrier disruption and has no observed effect on ureteral contraction.
Introduction
The ureter is normally coapted shut at rest, whereas an obstructed ureter can have a diameter of 5–10 mm (15F–30F). 3 Most currently available ureteral access sheaths, which facilitate access to the upper urinary tract, have a 4–4.5 mm outer diameter. Clinical studies have shown that ureteral calculi <6 mm pass in about one-third of the cases. 4 Larger stones will usually not pass, but have been found in both the proximal and distal ureters, suggesting that parts of the ureter can dilate to at least 10 mm in diameter. Medical expulsive therapy has been shown to improve stone expulsion rates by presumably relaxing the ureter. 5 Using a ureteral pressure catheter in a small clinical trial, Davenport et al 6 showed that, postoperatively, systemic diclofenac and nifedipine gave inconsistent ureteral pressure responses but had little effect on contraction frequency, whereas systemic tamsulosin significantly reduced ureteral pressure but had no effect on contraction frequency. Using medications to relax the ureteral smooth muscle prior to endourologic surgery could be of great future clinical importance as it could allow the passage of larger instruments and sheaths and thereby facilitate the treatment of larger stones with ureteroscopy, thus reducing the indications for the more morbid approach of percutaneous nephrolithotripsy.
As all medications currently used to relax the ureter are also used as blood pressure medications and can have unwanted systemic side effects, local application of these medications would be ideal. The urothelial barrier, however, inhibits passage of substances from the lumen to the ureteral smooth muscle. The umbrella cells, which have contact with the urine, form a barrier with tight junctions between cells. Specialized lipids and proteins in the apical membrane form hinges and plaques that are likely involved in the exocytosis and endocytosis that occur during bladder filling and emptying. 7 Multiple pharmacological agents have been described, which increase bladder urothelial permeability and may be useful for clinical practice. These include dimethylsulfoxide, nystatin, protamine sulfate, and chitosan. 8 Chitosan is produced by partial deacetylation of chitin, a substance found in insect and crustacean exoskeletons and the cell walls of fungi. Chitosan is a biodegradable and nontoxic polymer. 9 In the bladder, chitosan increases urothelial permeability by opening tight junctions between cells 10 or by desquamination of urothelium. 9 Similar studies have not been done in the ureter. In the present study, the effect of chitosan on ureteral contractile amplitude and frequency and ureteral urothelium permeability is measured.
Materials and Methods
Chitosan hydrochloride (Protasan UP Cl 213; degree of deacetylation: 83%, molecular weight: 150–400 kDa) was purchased from Novamatrix. Chitosan solution (0.5%, w/v) was made with water (pH 5.0). Nifedipine and phenylephrine were purchased from Sigma-Aldrich. Standard Krebs bicarbonate solution (pH 7.4) was used. Nifedipine solution (1 mM) was made with dimethyl sulfoxide. Phenylephrine solution (100 mM) was made with water. Dilutions were made using stock Krebs solution and all solutions were maintained at 37°C. Porcine ureters were surgically removed from adult female Yorkshire domestic pigs, weighing 40–50 kg, and immediately placed in Krebs bicarbonate solution at 5°C. All ureters obtained were from animals used in other Institutional Animal Care and Use Committee (IACUC)-approved protocols and would have otherwise been discarded as waste. All ureters were used within 1 hour of harvesting.
Ureters were then cleaned of periureteral fat and connective tissue. Visually, the most proximal portion of the ureter was dissected out and discarded to maintain physiologic homogeneity throughout the ureter. This was because the most proximal portion of the ureter differs from the remainder of the ureter both anatomically and physiologically: it showed frequent spontaneous contractions (pacemaker rhythms) with small amplitude and had a larger internal diameter and a thicker wall. The remaining ureter was then divided into 5-cm segments, yielding 2–4 segments per ureter. All segments were visually screened for perforations and those that failed inspection were discarded. Using a novel experimental setup developed in our lab (S.S.), each segment was cannulated horizontally in separate chambers of a double-walled 50-mL polystyrene organ bath (Fig. 1). A total of four organ bath chambers were used simultaneously. A 50-mL double-walled reservoir (height: 50 cm) was attached at the proximally cannulated end of each organ bath and drained at 1 mL/minute via an IV flow regulator (RF2500; Wolf Medical); the distal cannulated end of the organ bath was drained to gravity. The entire double-walled system was maintained at 37°C via an immersion circulator (Haake DC10; Thermo Scientific). Peristalsis was detected using a pressure transducer (TRN050; Kent Scientific) connected in series on the inflow end of the ureter. The output signal of the pressure transducer was processed using MacLab/400 and monitored in real time with Chart v3.4 (AD Instruments) (see Figure 2 for a complete experimental setup).

Two porcine ureteral segments cannulated in a polystyrene organ bath. Scale is 1 cm between marks.

Novel ex-vivo ureteral apparatus developed in our lab, capable of testing four ureteral segments at one time.
Both the organ bath (extraluminal) and upper reservoir (intraluminal) contained stock Krebs solution and these were aerated with 95% O2/5% CO2. Each ureter segment was equilibrated for 60 minutes, and then phenylephrine (10 μM) was added both intraluminally and extraluminally to stimulate peristalsis. This tested the viability of the tissue, and ureters that did not contract were removed from the study. After 10 minutes of peristalsis, the intraluminal and extraluminal environments were washed out with Krebs to remove all phenylephrine. Either chitosan (0.5%, w/v) or Krebs solution (control) was added intraluminally for 30 minutes at a flow rate of 1 mL/minute and then washed out for 30 additional minutes. Phenylephrine was again added to a concentration of 10 μM both intraluminally and extraluminally for 10 minutes and the frequency and amplitude of the peristalsis were measured. Nifedipine was then added intraluminally at a concentration of 1 μM. The primary outcome measured was the time to cessation of peristalsis, but changes in amplitude and frequency were also monitored throughout the experiment. If peristalsis did not stop after treating with 1 μM nifedipine for 60 minutes, the trial was stopped.
In an additional experiment, methylene blue was added to the intraluminal reservoir after treatment with chitosan or control solution as above. The external bath was visually inspected for methylene blue diffusion, and after removing the external bath, the ureteral segments were placed in formalin. A SmartSpec Plus spectrophotometer (BioRad Laboratories) was used to quantify the amount of methylene blue that had diffused through the urothelium into the external bath and this was compared with positive and negative controls. Hematoxylin and eosin (H&E) staining was performed and the ureteral pieces were transected across the lumen and mounted for histological staining. All histological analyses were done by one individual (J.T.-I.). All statistical analyses were performed using GraphPad Prism v4 (GraphPad Software). Paired t-tests were used to compare the pretreatment and posttreatment arms.
Results
Our primary outcome measure was the time to cessation of contraction after administration of 1 μM nifedipine intraluminally. These data are presented in Table 1. Control experiments demonstrated no change in contractile frequency or amplitude with administration of Krebs solution, and contractions continued in the presence of 1 μM intraluminal nifedipine even after 60 minutes of exposure. The amplitude of the contraction was similar before and after the administration of 1 μM intraluminal nifedipine, whereas the frequency was found to be significantly less (p = 0.0184) after 1 hour of 1 μM intraluminal nifedipine exposure. The time between contractions increased to ∼10 seconds. The control experiments were stopped after 60 minutes of observation of continued peristalsis. Next, the contractile frequency and amplitude were measured before and after administration of 0.5% (w/v) chitosan for 30 minutes. Intraluminal and extraluminal phenylephrine were given to cause peristalsis both before and after treatment with chitosan. Krebs was used to wash out all substances between arms. There was no significant difference between the contractile amplitudes of the pretreatment and chitosan tracings (p = 0.5226). For peristaltic frequency, treatment with chitosan followed by administration of phenylephrine caused a significantly (p = 0.0420) faster frequency, on average 1.5 times faster than the control arm.
As mentioned earlier, 1 μM intraluminal nifedipine had no effect on ureteral peristalsis in the control arm after 60 minutes. After treatment with chitosan, 1 μM intraluminal nifedipine stopped peristalsis, with a mean time to cessation of contraction of 12.30 ± 4.72 minutes (Fig. 3). After the addition of intraluminal methylene blue, 50 μL aliquots of the external bath from the untreated and pretreated arms as well as positive and negative controls were collected and analyzed using the spectrophotometer. There was no evidence of any diffusion of methylene blue across the ureteral wall in either the control (untreated) or chitosan arms (Fig. 4). Histological analysis (Fig. 5) after H&E staining showed a consistent difference in the thickness of the urothelium from ∼5–6 cell layers in the control group to 1–2 cell layers in the chitosan-pretreated group. There was also no evidence of methylene blue stain extending beyond the urothelial cells.
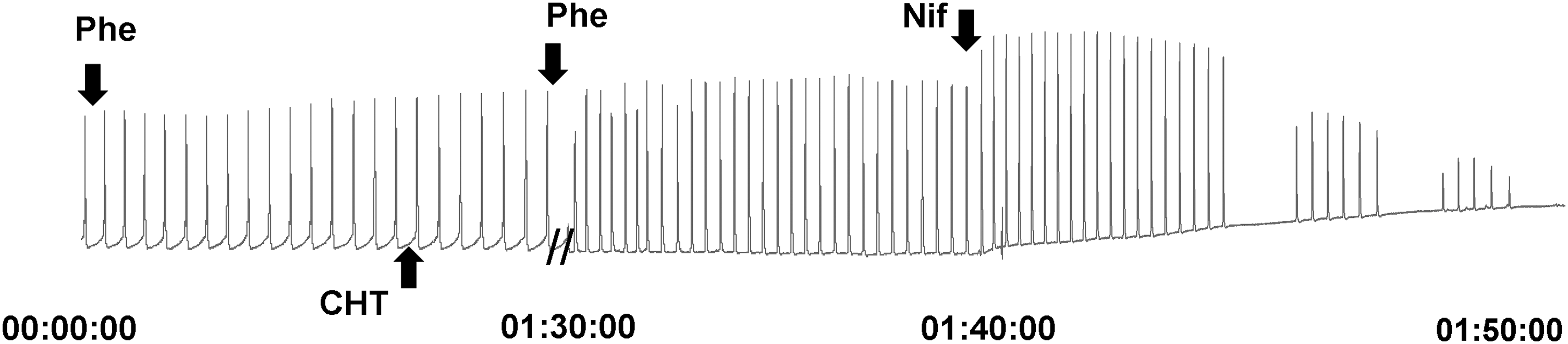
Sample tracing showing 1 hour equilibration, addition of phenylephrine (Phe), chitosan (CHT), and nifedipine (Nif ), and cessation of peristalsis. Time scale is in hours and minutes at bottom.

Graph showing difference in optical density of extraluminal bath for untreated and chitosan-treated ureteral segments after intraluminal exposure to methylene blue, compared with positive and negative controls.

Cross section of hematoxylin and eosin–stained porcine ureteral segments.
Discussion
Chitosan is produced by deacetylation of chitin, and when compared with chitin, it has an amine group that has a pK a of 6.2–7.0. Thus, in an acidic solution, chitosan is negatively charged, which allows interaction with the positively charged epithelium. Artursson et al 10 demonstrated that increasing the acidity of the chitosan solution increased the permeability of the epithelium. Chitosan can vary in both molecular weight and degree of acetylation. Schipper et al 11 studied various formulations of chitosan and found that absorption was enhanced with a low degree of acetylation and a high molecular weight. The chitosan formulation tested here had both a high molecular weight (150–450 kDa) and a low degree of acetylation (17%). In our experiments, chitosan appears to partially desquamate the urothelium and thereby increase the permeability, allowing medications to diffuse from the inside of the ureter and reach the smooth muscle, where they can more directly affect ureteral peristalsis. In this regard, of note is the statistically significant increase of the frequency of peristalsis that occurs after pretreatment with chitosan and repeat dosage with intraluminal and extraluminal phenylephrine. It is hypothesized that the chitosan changes the diffusion coefficient and allows more phenylephrine to reach the smooth muscle.
The biggest effect of chitosan in our study was the change in permeability that resulted in 1 μM intraluminal nifedipine causing a complete cessation of peristalsis. This low dosage of nifedipine by itself failed to produce an aperistaltic state. Although nifedipine in the absence of chitosan pretreatment did significantly reduce the frequency after 1 hour of exposure, there was no effect on peristaltic pressure (ureteral contractile amplitude). This reduction in frequency may also be due to desensitization of the ureter to phenylephrine (which is seen over time) as well as tissue degradation that occurs over time after the ureter is removed from its blood supply, oxygen, and nutrients. This may be due to comparing the 10-minute control period to the longer 60-minute test period in the control (no chitosan) arm. Although there are no other published experiments that examine the use of chitosan in the ureter, there are multiple studies that show this change in permeability in the bladder urothelium and also attempt to elucidate the mechanism for this change. Kos et al 12 found that chitosan caused a change in bladder wall permeability to moxifloxacin, and that this was time and chitosan concentration dependent. Scanning electron microscopy analysis shows large areas of desquamation of urothelium after 60 minutes of exposure to 0.5% (w/v) chitosan, which is much more intense than that of tissue exposed for only 15 minutes at the same concentration. 12 Transmission electron microscopy analysis shows tight junctions between cells partially opened at very low concentrations (0.0005%, w/v), whereas exposure for 15 minutes at 0.005% (w/v) shows cell necrosis and damaged mitochondria. 12 In this experiment, methylene blue did not penetrate or stain the muscle.
In this study, exposure to chitosan does not appear to have caused such severe damage, which may be due to the lower exposure time. It is unclear if there is any variation in diffusion rates due to the difference between incubation in solution compared with a pressurized system with solute flow past the urothelium; however, with the latter, one might expect a larger effect. 13 Additional experiments with scanning electron microscopy to quantify the degree of desquamation or the use of uroplakin antibodies or urothelial antibodies such as cytokeratin 20 are needed to better define the impact of chitosan on the ureteral urothelium. H&E staining did show evidence of urothelium thinning, suggesting that the umbrella cells and the superficial and intermediate urothelial cells were no longer intact, but the methylene blue studies suggest that this does not affect the barrier function of the urothelium. This could be the reason that the methylene blue does not stain the ureter, or there could be gap junctions between muscle cells 14 or other urothelium connective tissue that maintains the barrier. Although both protamine and chitosan have been shown to increase permeability in the bladder urothelium, 8 chitosan may prove to be better tolerated. Protamine was used to damage the urothelium in an interstitial cystitis model, 15 whereas chitosan (in a sulfated form) has been shown to decrease bladder inflammation in a rat model. 16 Chitosan is also generally recognized as safe by the Food and Drug Administration. 17 Although protamine is a relatively safe drug, it can cause anaphylactic reactions, 18 significant systemic hypotension, noncardiogenic pulmonary edema, severe pulmonary hypertension, thrombocytopenia, 19 or even death. 20
Multiple experiments have been done to relax the ureter. Using human ureteral ring preparations where the extraluminal and intraluminal environments were not separated, Sahin et al 21 were able to show that nifedipine at 0.1 or 1 μM was able to stop ring contractions. Davenport et al 6 showed in human studies that oral nifedipine had an inconsistent effect on ureteral peristalsis. In an in-vivo porcine model, Ames et al 22 showed an immediate increase in peristaltic frequency and a 5F increase in proximal ureteral diameter with 80 mg intraluminal verapamil. Although serum verapamil concentrations were below therapeutic values, there was a significant 22 mm Hg decrease in systolic blood pressure at 30 minutes. We have shown that a significantly lower dose of nifedipine is needed to cause aperistalsis when the ureter is pretreated with chitosan. This may make it possible to safely relax the ureter by precluding systemic side effects as above.
Conclusions
Treatment of the intraluminal surface of the ureter with chitosan increases the diffusion of nifedipine across the urothelial barrier. Although it does appear to thin the urothelium, chitosan was shown here to change the permeability of the ureteral urothelium without disrupting the barrier function of the urothelium. It has no direct effect on the contractile amplitude and does not stop ureteral peristalsis. Chitosan may allow the use of lower doses of medication and decrease systemic side effects when using medications to create an aperistaltic ureter. As such, it may be useful as an excipient for both intravesical and intraureteral drug administration.
Footnotes
Disclosure Statement
No competing financial interests exist.