
Abstract
Background and Purpose:
Shockwave lithotripsy (SWL) is considered a standard treatment for patients with upper-tract stones that are less than 10 mm in diameter, whereas stones that are larger than 20 mm are best managed by percutaneous nephrolithotomy (PCNL). The management of stones between these sizes remains controversial. Our purpose was to review our contemporary series of SWL, ureteroscopy (URS), and PCNL outcomes for intermediate-sized upper tract calculi (100–300 mm2).
Patients and Methods:
Analysis was restricted to those patients who were treated for a renal calculus that measured between 100 and 300 mm2 during a 4-year span. Demographic, stone, patient, treatment, and follow-up data were collected from a prospectively maintained database.
Results:
A total of 137 patients were referred with nonstaghorn calculi with an area between 100 and 300 mm2. Fifty-three (38.7%) patients were treated with SWL, while 41 (29.9%) and 43 (31.4%) underwent ureteroscopy and PCNL, respectively. Mean stone area was higher in the PCNL group (P < 0.001), whereas stone density was higher for patients undergoing SWL (P = 0.002). Single treatment success rates were better for PCNL at 95.3%,vs 87.8% for ureteroscopy and 60.4% for SWL, P < 0.001. When allowing for two SWL treatments, the success rate improved to 79.2%, thus equalizing the success of the three treatment modalities (P = 0.66). Auxiliary treatments were more common after SWL (42.3%; P < 0.01).
Conclusions:
For intermediate-sized upper-tract stones, when allowing for up to two SWL treatments, there was no significant difference between treatment modalities. Thus, SWL is a reasonably successful treatment alternative for patients who are not fit for a general anesthetic or who prefer SWL over competing treatments, provided they accept a potentially higher number of treatments.
Introduction
The endoscopic management of urolithiasis has matured over the past decade, with improved instrumentation and techniques for performing both ureteroscopy (URS) and percutaneous nephrolithotomy (PCNL). These two techniques have benefited from the miniaturization of endoscopic instrumentation, the emergence of novel energy devices, such as the holmium laser, improvements in instrumentation flexibility and accessories (ie, basket devices), and the ongoing dissemination of and increasing familiarity with proper technique. Several recent reports demonstrate acceptable success rates with retrograde ureteroscopy for large renal stones. 1 –3
As with most novel technologies, after their introduction, SWL was considered a panacea for the management of the majority of upper-tract stones with high success rates, and its indications for urolithiasis management were broad. 4,5 Limitations of SWL were soon identified, however. The detailed description by Sampaio and Aragao 6 of such anatomic parameters as infundibulopelvic angles and length and spatial arrangements of lower calices, followed by the meta-analysis by Lingeman and associates 7 that demonstrated higher stone-free clearance rates for PCNL vs SWL provided some guidance for urologists in recommending SWL as a viable treatment option for specific clinical situations.
Few randomized trials exist that compare SWL, URS, and PCNL. The Lower Pole Study Group has published two multicentered randomized controlled trials that examined the efficacy of PCNL, SWL, and URS in certain clinical scenarios. The initial study demonstrated that stone clearance from the lower pole after SWL worsens as the stone diameter increases beyond 10 mm, whereas PCNL maintains its efficacy as stones increase in diameter. 8 The subsequent study examined lower pole caliceal stones less than 10 mm in diameter and found no statistical difference in stone-free rates between SWL and URS, with the caveat that SWL was associated with greater patient acceptance and shorter convalescence. 9
With results from randomized controlled trials, there exists good evidence with which to make treatment decisions for stones less than 10 mm and greater than 20 mm. There is a paucity of clinical research, however, that compares the efficacy of the three treatment modalities for stones that measure between 100 and 300 mm2 in area, regardless of location in the upper urinary tract. The purpose of this study is to review the outcomes of a modern series of patients who were referred for treatment of upper-tract calculi with a stone area between 100 and 300 mm2 at a single Canadian tertiary care center. The cost-effectiveness of SWL, PCNL, and URS for intermediate stones in a single-payer, government funded health care system is the subject of future reports.
Patients and Methods
The study population was abstracted from prospectively maintained databases that record stone and treatment parameters of patients who were receiving SWL, URS, and PCNL at St. Michael's Hospital in Toronto, Ontario, Canada. Analysis was restricted to those patients with a pretreatment noncontrast CT scan conducted at our center that demonstrated an upper-tract calculus measuring an area between 100 and 300 mm2, and to patients who returned to our unit for follow-up. Regionalization of SWL resources requires many of our patients to travel great distances for treatment and to have follow-up with their local urologist. As such, patients were excluded if they did not have at least one follow-up visit with imaging at our center. Selection of treatment modality was influenced by a variety of factors, including urologist choice, patient preference, and stone characteristics. In addition, at our lithotripsy unit, patients are referred specifically for SWL by their own urologist, and as a result, many patients with higher stone density or skin-to-stone distance (who might have higher treatment success rates with other treatment modalities) receive SWL.
SWL was conducted by several academic urologists with a single lithotripter (Healthtronics Lithotron Ultra) in the Kidney Stone Centre. All patients were treated under neuroleptic sedation to a maximum of 3000 shocks at a maximum power of 23 kV. Oral anticoagulation therapy and nonsteroidal anti-inflammatory medications were discontinued before treatment. Our policy dictates that all patients with stones that are greater than 15 mm in maximal diameter should have a ureteral stent inserted before SWL.
All PCNL and URS were performed under a general anesthetic by one of two urologists in an academic environment. URS was performed as a day procedure with the use of access sheaths, stone retrieval devices, and ureteral stents (left to the discretion of the surgical team). PCNL was performed in a single stage with antegrade access to the renal collecting system acquired by the urologic team after insertion of a ureteral occlusion catheter. Ultrasonic and ballistic lithotripsy were chosen at the discretion of the treating urologist, in conjunction with flexible nephroscopy and holmium laser lithotripsy when necessary. All patients were left postoperatively with an 8F to10F nephroureteral catheter.
Successful URS and SWL treatment of patients with calculi was defined as those patients who were stone free or had asymptomatic, clinically insignificant residual fragments <4 mm in diameter 3 months after a single treatment; patients who needed adjuvant treatments (such as repeated SWL, URS, or PCNL) were considered as primary treatment failures. Successful PCNL treatment of patients with calculi was defined as patients being stone free 2 weeks post-treatment. Treatment outcomes were assessed with a combination of kidneys-ureters-bladder (KUB) radiography, tomography, ultrasonography, and noncontrast CT.
Patient demographic, stone, treatment, and follow-up data were collected from a prospective database, and review of CT and KUB imaging was performed by two independent urologists and one radiologist. Data were analyzed with chi-square analysis and analysis of variance, where appropriate, using Statistical Package for Social Sciences (SPSS), version 16 (Chicago, IL).
Results
Data from 137 patients with nonstaghorn calculi with an area between 100 and 300 mm2 were analyzed. Across groups, there were 89 (65%) males, 61 (45%) right-sided stones, an overall mean age of 53.1 years (standard deviation [SD] 14.2 y), and body mass index of 29.0 kg/m2 (SD 6.6 kg/m2). As delineated in Table 1, mean stone area was significantly larger in those patients who were treated with PCNL (211.1 ± 56.8 mm2) when compared with those patients who were treated with SWL (172.6 ± 58.2 mm2) and URS (162.9 ± 54.9 mm2), P < 0.01. In addition, stone density, as measured by averaging Hounsfield units on CT scan, was significantly higher in those patients who were treated with SWL (1008 ± 244 HU) when compared with those patients who were treated with URS (786 ± 289 HU) and PCNL (837 ± 326 HU), P < 0.01.
Data are expressed as mean (standard deviation) or n (%), where applicable.
SWL = shockwave lithotripsy; URS = ureteroscopy; PCNL = percutaneous nephrolithotomy; BMI = body mass index; HU = Houndsfield units; NS = not significant.
Single treatment success rates were significantly better for PCNL at 95.3% vs 87.8% for URS and 60.4% for SWL, P < 0.01. When up to two SWL treatments were administered, however, the SWL success rate improved to 79.2%, thus removing any significant difference between the success of the three treatment modalities, P = 0.66. If up to three SWL treatments were administered, success rates improved further to 85.0%. Of note, 21 (39.6%) patients underwent repeated SWL for their original stone, and of those patients, 4 (7.5% of all SWL patients) underwent three treatments. Auxiliary treatments, defined by repeating the initial treatment modality or progressing to one of the two alternative modalities, were more common after SWL (42.3%) vs 9.8% and 7.0% in the URS and PCNL groups, respectively. Five (9.4%) patients who underwent initial SWL needed subsequent URS for definitive stone management. Success rates across modalities are seen in Figure 1 and Table 2.
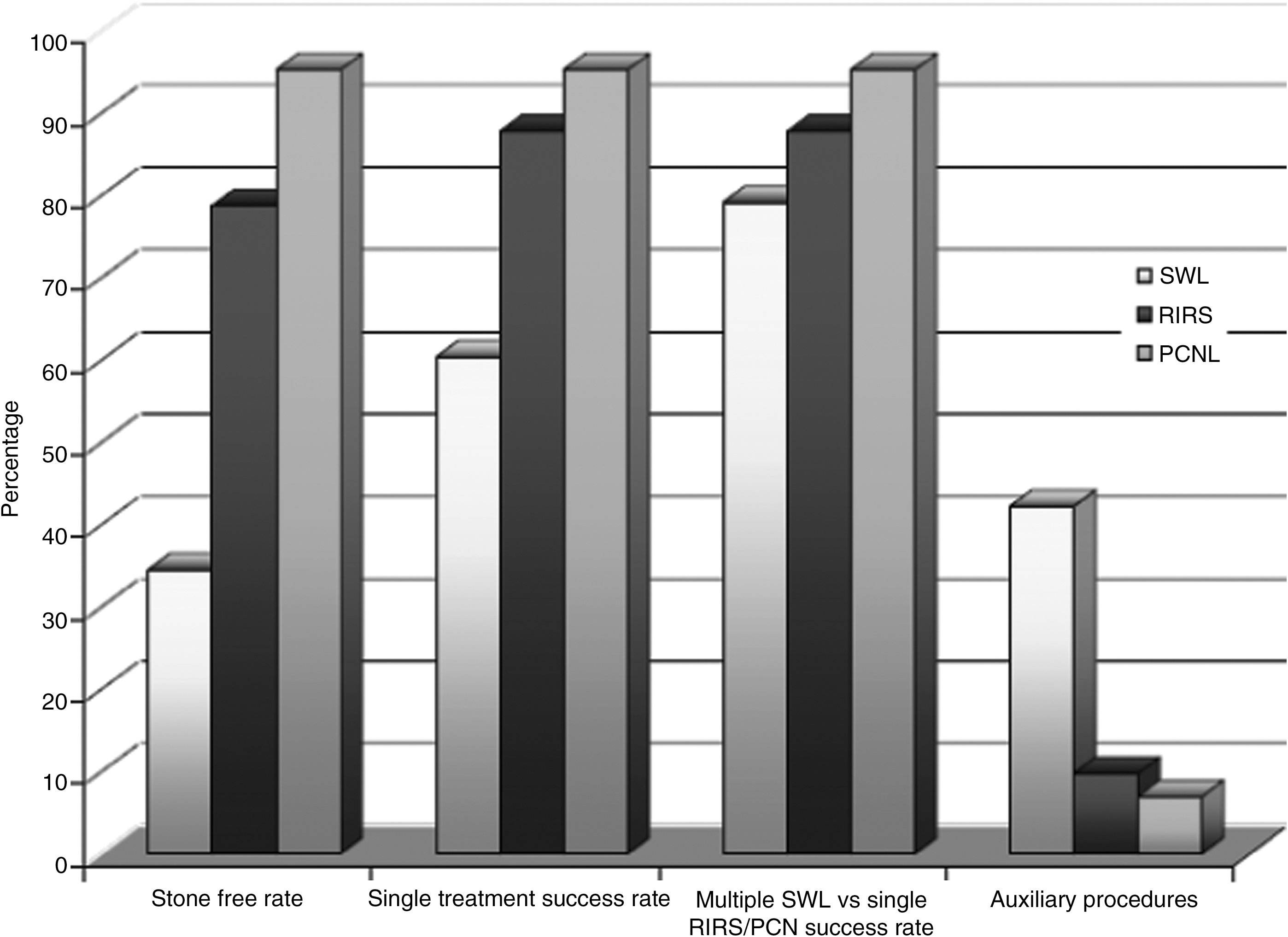
Treatment outcomes and auxiliary procedures across groups. SWL = shockwave lithotripsy; RIRS = retrograde intrarenal surgery; PCNL = percutaneous nephrolithotomy.
Data are expressed as n (%).
SWL = shockwave lithotripsy; URS = ureteroscopy; PCNL = percutaneous nephrolithotomy; NS = not significant.
There is a difference among treatment arms for post-treatment hospitalization, with all patients undergoing PCNL admitted overnight for observation, P < 0.01. When measuring the mean length of hospital stay postoperatively, there was a significant difference between the SWL therapy (0.17 days), URS (0.35 days), and PCNL (2.9 days), P < 0.01. All PCNL patients underwent ureteral stent placement perioperatively (with the use of a nephroureterostomy tube postprocedure), whereas 90.2% of patients who were undergoing URS and 35.9% of patients in the SWL group had periprocedural ureteral stent placement, P = 0.04. “Procedural outcomes and Clavien grade complications are found in Table 3.”
Data are expressed as mean (standard deviation) or n (%), where applicable.
SWL = shockwave lithotripsy; URS = ureteroscopy; PCNL = percutaneous nephrolithotomy.
Complications were equivalent across treatment groups, as classified by the Clavien grading system. Complications were dichotomized by Clavien grade, such that Clavien grades I to II complications were considered minor and Clavien grades III to V complications were major. All minor complications in the SWL arm were in patients who returned to either the clinic or emergency department with renal colic secondary to steinstrasse. The two minor complications in the URS treatment arm included mild hypotension intraoperatively and urinary retention postoperatively. In the PCNL group, there was one major complication that consisted of a minor bleed from the access tract that necessitated neither a blood transfusion nor embolization, and five minor complications that consisted of postoperative atelectasis (n = 3) and urinary tract infections (n = 2).
Discussion
SWL is minimally invasive and necessitates only neuroleptic anesthesia, making it the preferred initial treatment choice by many patients and physicians for a wide range of urolithiasis. 5,10 Stone-free rates are poor, however, for stones that are located in the lower calix, especially if the stones are >10 mm in diameter. 8 Although associated with a higher morbidity than other stone treatments, PCNL for larger stones and staghorn calculi has replaced SWL and URS as the primary treatment modality. 11 –13 Some series publish somewhat acceptable success rates with URS for staghorn or larger renal calculi 1,14 ; however, this is not widely performed nor considered the standard of care in the urologic community. 13
Selecting the optimal treatment of intermediate-sized stones (those between 100 and 300 mm2) can be challenging for patients and urologists alike, because each treatment modality has unique advantages and disadvantages. In the current study, when comparing single treatment rates across groups, the stone-free and success rates were significantly lower in those patients who were treated with SWL than in those patients who were treated with PCNL or URS. When comparing the success rates of up to two (or up to three) SWL treatments vs a single treatment of either PCNL or URS, however, there was no significant difference. Auxiliary treatment rates are significantly higher for patients in the SWL arm, but this is largely because re-treatment rates are higher. The equivalency of success across groups, if one allows up to three SWL treatments, is balanced by the decreased rate of hospitalization, length of stay, need for ureteral stents, and morbidity.
With respect to complications, there were no significant differences between those patients who were treated with SWL, PCNL, or URS. Complications of PCNL are typically between 4% and 15%, depending on the case series, location of percutaneous access, and the type of specialist who is gaining percutaneous access. 15,16 For URS treatment of patients with stones between 1 and 2 cm, Hollenbeck and colleagues 17 reported a complication rate of 21% with an admission rate of 17%. Regardless of stone size, other studies report intraoperative complication rates of <5% and postoperative complication rates between 10% and 25%, with major complications comprising fewer than 1%. 3,18 Complication rates for SWL range from 4.7% to 56.2%, depending on the reported series. 19,20 Our retrospective series demonstrates low complication rates with no significant difference, regardless of treatment modality.
Being a retrospective study, there are some inherent limitations. The patients were not randomized between treatment modalities, which might magnify any inherent biases held by either the urologist and patient toward the specific treatment modalities. For example, CT attenuation values were higher for stones that were managed with SWL when compared with both URS and PCNL because most pure uric acid stones are not managed with SWL (and fluoroscopic targeting) at our center; thus, uric acid stones will be over-represented in the URS and PCNL groups. In addition, because of the regionalization of SWL resources, patients are referred by several urologists and from great distances. Patients are referred to the lithotripsy unit directly; thus, the true denominator of patients with intermediate-sized stones is unknown, because many patients might be treated with PCNL or URS in the various referral centers. Furthermore, many patients are followed up with their referring urologists post-SWL if they have traveled from great distances; thus, these patients who did not organize follow-up at our center were excluded from our analysis.
Each treatment modality has its specific advantages and disadvantages, and several patient factors and physician biases will influence their treatment of choice. Urologists who favor URS balance the moderately invasive nature of the procedure with its greater one-time success rate, lack of hospitalization, and absence of a costly lithotripter machine. In our system, urologists must decide whether to treat the patient themselves with an endoscopic procedure or refer the patient to a lithotripsy unit where they do not have privileges. Urologists who favor SWL treatment for these sizes and locations of stones might base their decision on the minimally invasive nature of the day procedure and negligible anesthetic requirements with the caveat of potentially multiple treatments and the need for a ureteral stent with stones greater than 15 mm in diameter. Lastly, urologists favoring PCNL do so based on the excellent single-treatment success rates with the moderately invasive procedure, possible anesthetic difficulties in the prone position, need for nephrostomy tubes or stents, and a short postoperative hospitalization. In any regard, the final choice will be based on a combination of patient preference, clinical scenario, the equipment and resources available, and lastly, the urologist's biases and expertise with the three treatment modalities.
Conclusions
This study demonstrates that PCNL, URS, and up to two SWL treatments are safe and comparably effective in treating patients with intermediate-sized upper urinary tract stones with an area between 100 and 300 mm2. Although necessitating repeated treatments to match the efficacies of PCNL and URS, SWL is less invasive and obviates the need for a general or spinal anesthetic, postoperative hospitalization, and in a significant percentage of patients, periprocedural insertion of ureteral stents or nephrostomy tubes for many patients.
Footnotes
Disclosure Statement
No competing financial interests exist.