
Abstract
Background and Purpose:
Percutaneous nephrostomy (PCN) still plays a significant role in decompressing the renal collecting system. Percutaneous nephrostomy tubes (PNTs), however, which are flexible and may not be protected well by patients, are vulnerable to mechanical drag, although they are carefully fixed to the skin with silk suture. We developed a simple method to reinforce the nephrostomy tube against dislodgement from the skin.
Patients and Methods:
A total of 133 adult patients underwent ultrasonography-guided PCN; 85 patients received a conventional method to fix the tubes, while the other 48 patients received a new one. We used a rubber drainage tube, about 2 cm long, sheared longitudinally, as the outer tube to encase the nephrostomy tube, and then sutured the cutting edges together with the skin suture to reinforce the nephrostomy tube.
Results:
Compared with the 85 patients who received the conventional method, there was not any tube dislodgement after PCN in the 48 patients who received the new one at the end of 2 weeks (0 vs 7, P = 0.049) and 4 weeks (0 vs 10, P = 0.014) follow-up.
Conclusions:
This is a simple, effective, and inexpensive method that can significantly decrease the dislodgement incidence of PNTs and keep them fixed well after surgery.
Introduction
Nephrostomy tube dislodgement (11%) has been a more common complication for PCN despite the fact that other complications, including massive hemorrhage necessitating transfusion or embolization (1%–3%), pneumothorax (<1%), urine extravasation (<2%), death (0.2%), and sepsis (1.3%), have been reported. 5 With technologic improvement, however, the complications of PCN now have become less and less. Even so, recently Rana and associates 6 still found tube dislodgement in 11 of 667 (1.64%) patients. When the tubes are dislodged, insufficient drainage may result in deleterious effects. 2,7,8 In patients who should retain the tube permanently, the effect of tube dislodgement was more obvious.
Because there has not yet been an effective method to avoid nephrostomy tube dislodgement, it has become necessary to develop some novel means to prevent the dislodgement of the PNTs. Recently, a new fixation method for the PNT that has been used in our clinical practice has significantly reduced the rate of tube dislodgement. To further evaluate this method, we conducted a single-center retrospective study of a cohort of 133 patients who have received PCN at our hospital from 2006 to 2009. In this present study, we introduced this new fixation method in detail and tried to illustrate its advantages for retaining the PNTs well.
Patients and Methods
Patients
From January 2006 to November 2009, a total of 158 adult patients, aged 24 to 75 years, underwent PCN at our hospital. Of these, 25 patients with either bilateral nephrostomy or retention of the tube less than 4 weeks were excluded. Indications for nephrostomy were supravesical urinary tract obstruction because of malignancy in 111 cases, obstructive pyonephrosis from ureteral calculi in 11, postsurgical iatrogenic stenosis in 9, and retroperitoneal fibrosis in 2. From June 2008 to November 2009, the new method was used to fix the tube (group A) while the conventional one was used from January 2006 to May 2008 (group B).
Ultrasonography-guided PCN
Initially, the patients were positioned prone with the back skin exposed. An optimal calix was targeted and punctured by an 18-gauge needle under the guidance of ultrasonography; if there was a urine spout from the needle after removing the stylet, access to the collecting system could be confirmed. Then a 0.032 inch zebra guidewire (Urovision, Germany) was inserted into the collecting system via the needle, and there was sequential tract dilation with 10F, 12F, 14F, and 16F fascial dilator (Urovision, Germany) followed by insertion of a 14F nephrostomy tube (Cook Inc. Spencer, IN).
New method for fixation of the PNT
Commonly, silk suture (Mersilk 3-0, Ethicon, New Brunswick, NJ) was used to fix the nephrostomy tube. First, a surgical knot was tied tightly above the skin. Then, both ends of the silk suture were tied with a double knot approximately 1 to 2 cm above the skin before being wrapped around the tube several times. Finally, both ends of the suture were tied off with a surgical knot to secure the tube. Usually, two sutures were recommended.
In the present study, to reinforce and secure the PNT, we developed a simple, effective, and inexpensive method. Briefly, before surgery, we chose an ordinary rubber drainage tube with an inner diameter equal to the outer diameter of the PNT. Then we cut this tube into a section 2 cm long or so, based on our previous study that showed that a longer tube might limit the flexibility of connections, while a shorter one (less than 1 cm) also disturbed its effectiveness, especially in overweight patients. After that, the 2-cm rubber fragment was sheared longitudinally as an outer sleeve to encase the nephrostomy tube. Then silk suture, introduced above, was used, but before being wrapped around the rubber tube, the suture penetrated both cut edges of the rubber tube and was tied off with a double knot to close the cut edges. Similarly, two sutures were recommended to reinforce the PNT (Fig. 1).
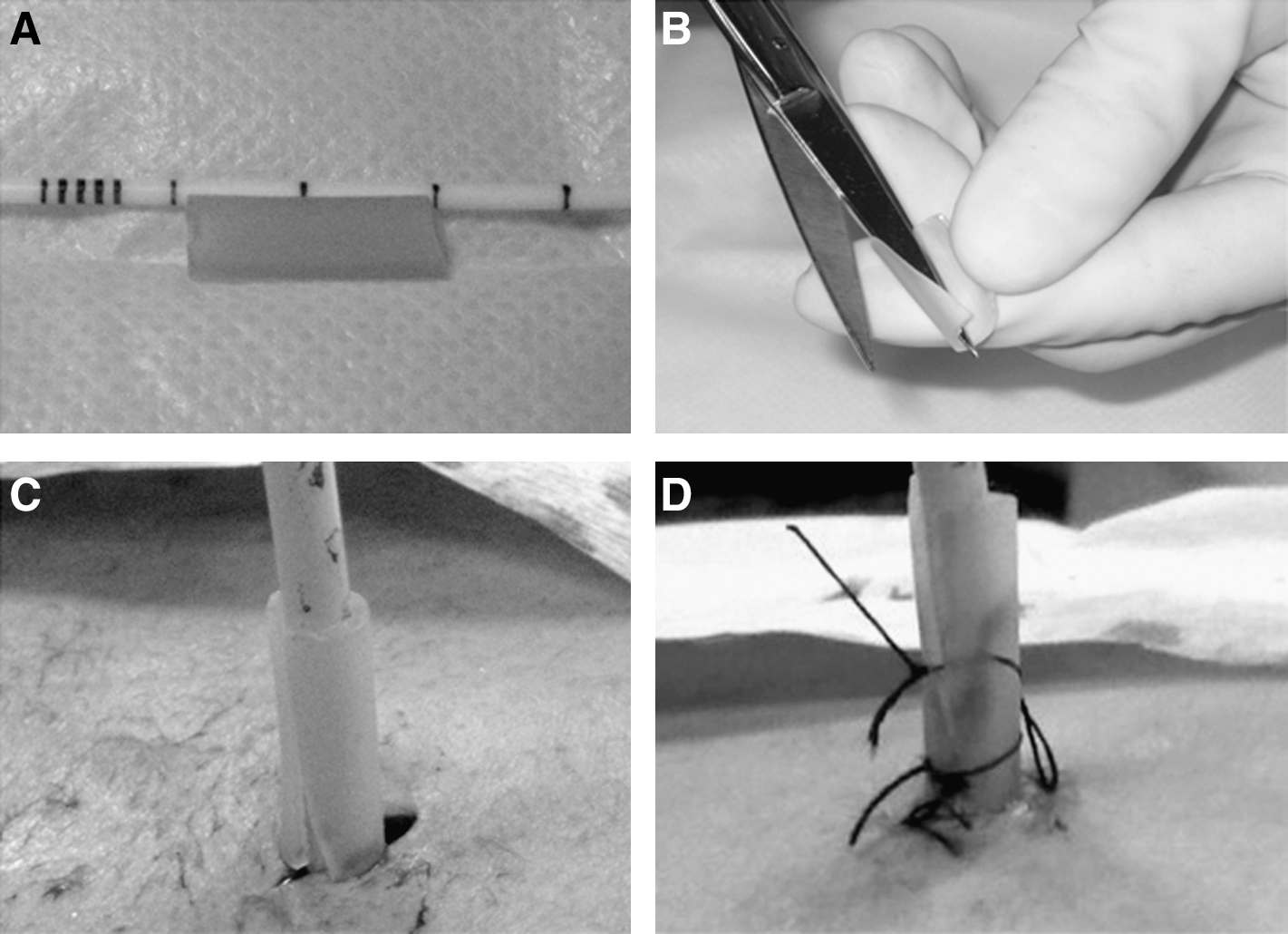
Reinforcement of nephrostomy tube.
Analysis of the new fixation method
Tube dislodgement included the PNT slipping out of the renal collecting system or the PNT was malpositioned but not out of the collecting system. We assessed tube dislodgment by antegrade pyelography. The outcomes of both groups were also evaluated at the end of follow-up, including fever, bleeding, and organ damage.
Statistics
The SAS 9.1 software was used for data processing. Statistical analysis was performed using the chi-square test. Statistical significance was defined as P < 0.05 for a two-tailed test.
Results
We used this new method in 48 patients from June 2008 to November 2009. As a result, there was no tube dislodgement in this group after surgery. In the control group of 85 patients who had received the conventional method to fix the nephrostomy tube, there were 7 patients whose tubes dislodged within 2 weeks (0 vs 7, P = 0.049). There was no significant difference for age, sex, and body mass index of patients between the two groups (Table 1).
BMI = body mass index.
By the end of the fourth week, tube dislodgement in each group was assessed again. There was not any tube dislodgement in group A. In group B, however, three more patients had tube dislodgement in the third week (0 vs 10, P = 0.014). We found more and more patients with tube dislodgement as time went on in group B, and the number of patients who still kept the tube decreased significantly.
For seven patients with tube dislodgement during 2 weeks of follow-up, another ultrasonography-guided PCN was performed. Of three patients with tube dislodgement beyond 2 weeks of follow-up, one patient had a failed attempt to reinsert another tube because of fistulous tract loss and received an additional ultrasonography-guided PCN. At the end of follow-up, there were no severe complications, such as fever, bleeding, or organ damage, in both groups.
Discussion
Percutaneous drainage of the renal collecting system is a suitable, even crucial, method for hydronephrosis and pyonephrosis. Nephrostomy tube is routinely placed at the end of PCN to decompress an obstructed kidney. Even now, PCN still plays an important role in the urologic field.
Initially, PCN was performed mainly under the guidance of fluoroscopy or combined with ultrasonography. Now, ultrasonography-guided PCN has become common, and even some urologists use MRI to guide their operations. 6,9 –11 In general, all these great improvements in imaging guidance have made PCN a safer and more effective procedure in urologic practice.
In many cases, however, the drainage tube should remain in the renal collecting system for a very long time, which has made tube dislodgement a common event. For one thing, the flexible and slippery nephrostomy tube can be easily pulled out by the careless patient. For another, the tube is just tied by a skin suture, and the tube can easily slip out when the silk suture goes looser and looser because of the long time.
In the present study, we developed a new technique to reinforce the PNTs. First, we cut a 2-cm long rubber segment from an ordinary tube to encase the PNT, which can help prevent the tube from sliding. Then, we sutured the outer tube instead of just tying it, which may still fix the tube even when the suture becomes loose.
All patients were followed for 4 weeks after surgery. Our data showed that there was no tube dislodgement in the patients with the new fixation method. This advantage remained until the end of the fourth week, when there were 10 cases of tube dislodgement in the group with only silk suture (P < 0.05). In addition, we found that there was no indwelling induced complication in the group with the new fixation method at the end of follow-up, which suggested its safety in clinical use.
During our practice, we have compiled some tips for this method. For one thing, the outer rubber tube should not be too long, and the suitable length is about 2 cm; a longer tube may limit the flexibility of connections. For another, it is appropriate for the outer tube to just wrap the nephrostomy tube, preferring to be a little tight to increase friction. Therefore, the outer tube's diameter should be in accord with that of the nephrostomy tube. Last, the cutting edges must be sutured together with tight knots, which may transmit the mechanical stress from the connector to the body and consequently decrease the incidence of tube dislodgement.
Applying this new method, we can remarkably decrease the dislodgement of PNTs and keep them well in position for a necessary long time. In addition, this method is simple, effective, and inexpensive. Compared with about an 11.7% incidence of drainage tube dislocation by the usual fixation method, there is no drainage tube dislodgement in patients with the new fixation method, which strongly proves the validity of this method.
Traditionally, silk suture was chosen for drain fixation because it can be easily handled and facilitates grip of the drain tubing. Silk suture, however, has disadvantages such as skin irritation and easy degradation over time. Although no skin erythema to the silk suture and eventual extrusion of the stitch have occurred in the present study, nylon sutures, which are inert, nonabsorbable, and can remain in situ for a long period should be preferred for future patients. Otherwise, we believe there are other nice methods to avoid tube dislodgement that have not yet been reported; even so, the new method introduced in the present study is still comparable with those good ways to avoid tube dislodgement.
Footnotes
Disclosure Statement
No competing financial interests exist.