
Abstract
Background and Purpose:
Horseshoe kidney (HSK) is the most common renal fusion anomaly, with a prevalence of ∼1 in 400 and an incidence of urolithiasis between 20% and 60%. The role of shock wave lithotripsy (SWL) in patients with HSK remains poorly studied.
Methods:
Data from all patients treated since January 1994 with a known HSK was reviewed. Analysis was restricted to all patients with a minimum follow-up of 2 weeks after SWL. Success was defined as patients who were stone-free or had asymptomatic, clinically insignificant residual fragments ≤4 mm.
Results:
Data from 41 patients with HSK were analyzed (61 calculi). Mean stone size was 91.3 ± 71.6 mm2; mean body mass index was 27.1 ± 5.3 kg/m2. At 3 months, the single-treatment success and stone-free rates were 25.0% and 9.1%, respectively. The overall treatment success rate at 3 months was 63.6%, and the stone-free rate was 39.1%. Little incremental benefit was found for more than two SWL treatments per stone. The auxiliary treatment rate was 72.7%, with an efficiency quotient of 10.5%. On multivariate analysis, stone burden (p = 0.074), other calyceal location (p = 0.026), and body mass index (p = 0.013) were found to be prognostic for SWL success.
Conclusions:
Patients with HSK appear to have lower success and stone-free rates after SWL than patients with normal kidneys. This likely has to do with factors such as greater skin-to-stone distance (particularly for calyceal stones) and restricted urinary drainage. SWL may be offered to patients with a HSK once limitations in stone clearance have been considered.
Introduction
For patients with congenital anomalies of the urinary tract, including HSK, treatment of urolithiasis poses a particular challenge. Extracorporeal shock wave lithotripsy (SWL) is considered the first-line treatment for the majority of patients with urolithiasis; however, success rates in patients with HSKs remain poorly studied. Our goal was to determine the clinical success and stone-free rates for patients with HSK treated with SWL as well as to examine patient and stone-related factors contributing to success in this group of patients.
Materials and Methods
We performed a retrospective review of all patients with HSK treated and followed at the Kidney Stone Centre at St. Michael's Hospital, University of Toronto, since January 1994. All patients with previously untreated radio-opaque stones within the kidney who underwent SWL were included in the analysis. We excluded patients unable to return for a minimum 2-week follow-up. In all cases, the diagnosis of HSK was confirmed by the presence of one or more of computed tomography (CT), intravenous urogram, or ultrasonography. In total, 64 patients with 103 calculi were treated at our centre over a 15-year period. Two-week follow-up data were available for 41 patients (with 61 stones) and 3-month follow-up data were available for 29 patients (with 44 stones). Individual treatment data were available for each stone, and thus each stone was considered separately in the univariate and multivariate analyses. The study was approved by our institutional ethics review board.
Treatment
Before January 2001, the Dornier MFL-5000™ lithotriptor (Dornier Medical Systems Inc., Atlanta, Ga) was used. From January 2001 forward, Philips LithoTron™ lithotriptor (HealthTronics, Marietta, GA) was used. All patients were treated on an outpatient basis with neuroleptic anaesthesia that usually consisted of propofol, fentanyl, and midazolam. During treatment, all patients were placed in the supine position. For the Dornier MFL-5000, shock wave intensity was started at 14 kV and gradually increased to 23 kV. For the Philips LithoTron, shock wave intensity was started at 14 kV and gradually increased to 23 kV. Biplanar fluoroscopy was used for stone localization, and was employed every 100 to 200 shocks and as necessary to ensure the stone was within the focal zone. At our institution, renal calculi routinely receive 3000 shocks per treatment at a rate of 120 shocks/second unless the stone appears to be completely fragmented.
Primary follow-up of patients at our institution is carried out 2 weeks after treatment. At this visit, patients are either referred for additional SWL treatments or auxiliary treatments as needed, or scheduled for an additional follow-up appointment at 3 months if stone-free or if adequate stone fragmentation is noted on imaging. The primary outcome of interest was the single-treatment success rate, determined at 2 weeks and 3 months after SWL. Success was defined as an asymptomatic patient who was either stone-free or had a fragment ≤4 mm on the kidneys, ureter, and bladder (KUB), and who did not require any additional treatment for the treated stone. The single-treatment stone-free rate on KUB was also determined at both 2 weeks and 3 months after SWL. Primary outcome assessment was conducted by a urologist who reviewed all imaging and supervised follow-up visits.
Statistical analysis
Logistic regression was used to test the importance of both stone and demographic factors on success rates. Change in stone area after treatment was compared using analysis of covariance. Parametric parameters were compared with the Student t-test. Nonparametric parameters were compared using the Chi-squared and the Mantel–Haenszel statistic or the Mann–Whitney test where appropriate. Statistically significant differences were considered at two-sided, p < 0.05 using the SPSS 16.0 statistical package.
To facilitate comparison between machines, efficiency quotients were calculated using the following formula:
Results
Commencing January 1994, 64 patients with HSK (103 stones) underwent SWL at our center. Follow-up was available for 61 stones at 2 weeks and 44 stones 3 months after treatment. Follow-up for the remaining patients was conducted by the referring urologist. Baseline characteristics are presented in Table 1. Although two lithotriptors were used over a 15-year period, patients were similar in terms of sex, body mass index (BMI), side of treatment, initial stone area, presence of a ureteral stent at the time of SWL, and stone location.
Data are reported as mean ± standard deviation or n (%) where appropriate.
BMI = body mass index; RP = renal pelvis; LC = lower calyx; UPJ = ureteropelvic junction; AP = apatite; COM = calcium oxalate monohydrate; COD = calcium oxalate dihydrate.
Apart from the lithotriptor used, treatment did not differ between groups. The mean number of shocks per stone on the Dornier MFL-5000 lithotriptor was 2956.1 ± 215.7 and on the Philips Lithotron was 2982.1 ± 463.9 (p = 0.536). The mean amount of fluoroscopy time used was 2.89 ± 1.5 minutes on the Dornier MFL-5000 and 2.86 ± 1.3 minutes on the Philips Lithotron (0.932).
Overall, the single-treatment success rate at 2 weeks after SWL was 44.3% and the stone-free rate was 26.2% (Fig. 1). Using the Dornier MFL-5000 lithotriptor, the success rate was 60.0% and the stone-free rate was 30.0%. Using the Philips Lithotron, the success rate was 36.6% and the stone-free rate was 24.4%. There was no difference in overall success (p = 0.084) or stone-free rate (p = 0.640) when comparing results for both lithotriptors. At 3-months, overall single-treatment success and stone-free rates decreased to 25.0% and 9.1%, respectively. Using the Dornier MFL-5000 lithotriptor, the single-treatment success rate was 41.7% and the stone-free rate was 16.7%. Using the Philips Lithotron, the single-treatment success rate was 18.8% and the stone-free rate was 6.2%. Again, no differences were detected in the clinical success (p = 0.118) and stone-free rates (p = 0.284) when the different lithotriptors were compared. At 3 months, 72.7% of stones needed auxiliary treatments (repeat SWL, percutaneous nephrolithotomy [PCNL], or ureterorenoscopy). For the Dornier MFL-5000, the auxiliary procedure rate was 58.3% compared with 78.1% for the Philips Lithotron (p = 0.189). Three patients underwent PCNL, whereas 29 required at least one additional SWL treatment.
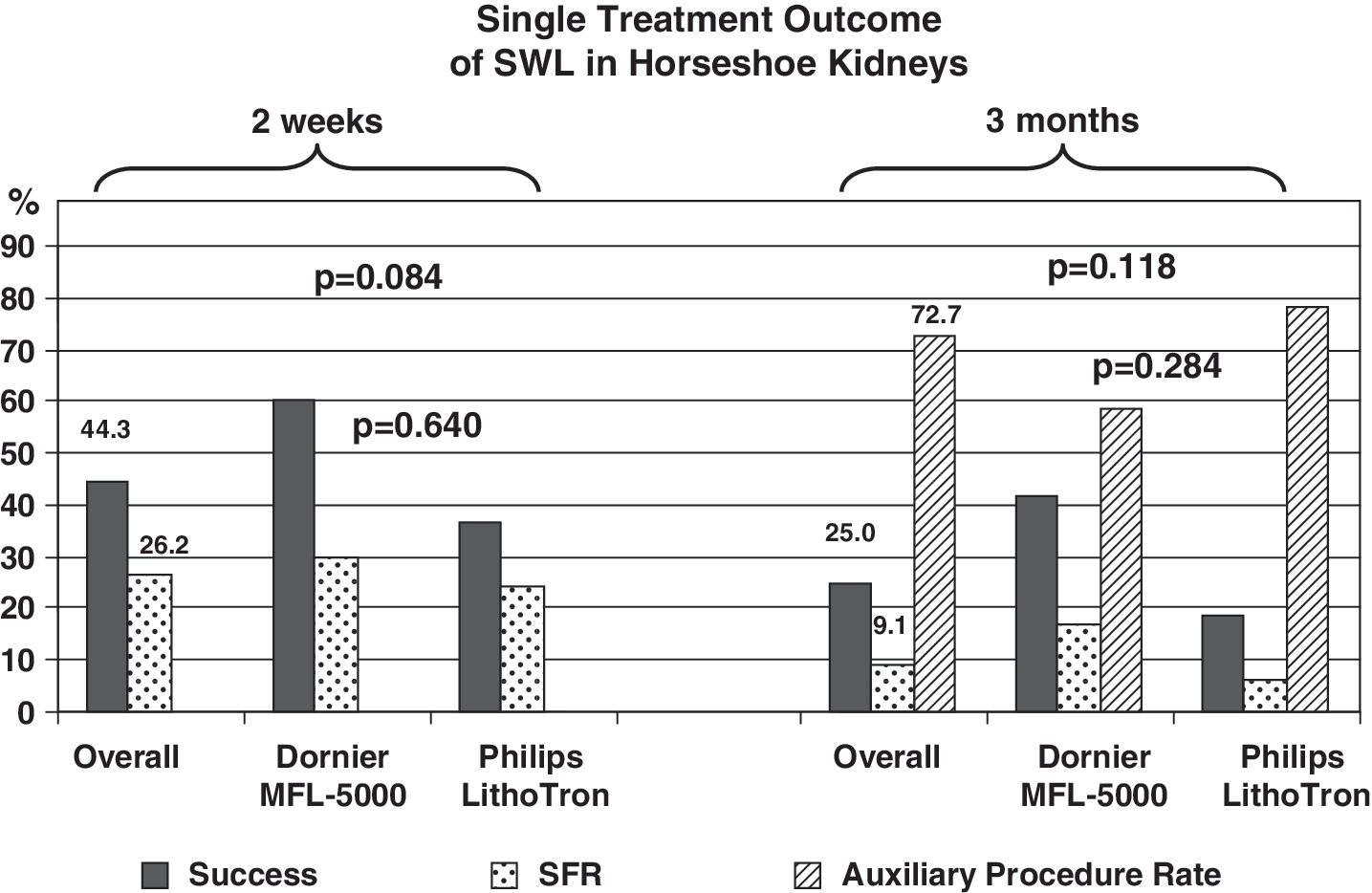
Single-treatment outcome of shock wave lithotripsy (SWL) in patients with horseshoe kidney. Both 2-week and 3-month follow-up data are shown. SFR = stone free rate.
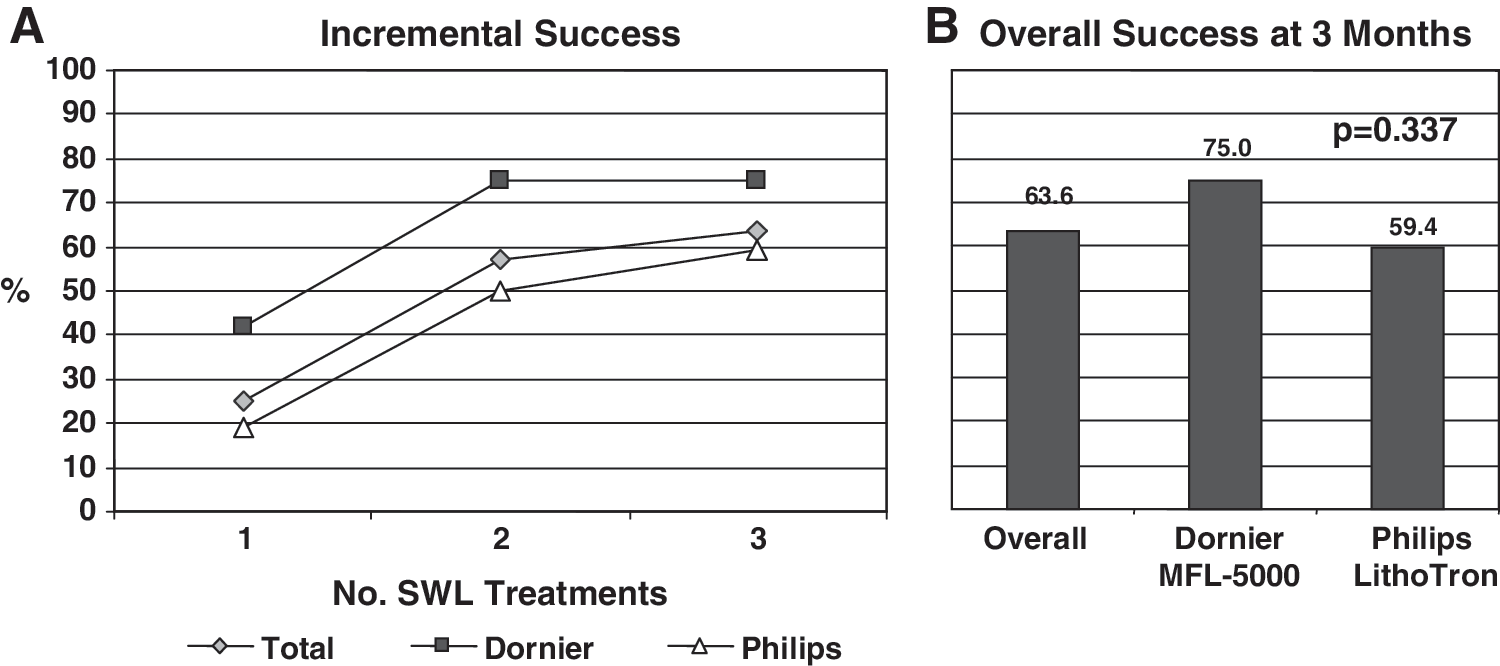
The overall SWL treatment success rate (after more than one SWL treatment for the same stone) was 63.6% at 3 months and the overall stone-free rate was 39.1%. For the Dornier MFL-5000 lithotriptor, the overall success rate was 75.0%, whereas for the Philips Lithotron it was 59.4%. No difference was detected in the overall success rate using either lithotriptor (p = 0.337). On average, a treated stone required 1.71 SWL treatments for fragmentation (Fig. 2). Little incremental benefit was seen beyond two SWL treatments. No patient in our series underwent more than three SWL treatments for the same stone.
Stone composition was analyzed for 31 patients. The primary stone composition was calcium oxalate monohydrate (83.9%), followed by dihydrate (12.9%) and calcium phosphate (3.2%) (Table 1). There were no struvite calculi. Stone composition was not significantly different for either lithotripter (p = 0.153). Similarly, at the 2-week and 3-month follow-up appointments, no difference was observed when the stone composition was considered based on lithotripter used (p = 0.390 and p = 0.301, respectively).
Univariate analysis was performed to investigate the relative impact of individual prognostic factors on single-treatment SWL outcome in this patient population. At follow-up 2 weeks after treatment, factors found to impact clinical success included BMI ≥30 kg/m2 (p = 0.005) and stone area (p = 0.014) (Table 2). Three additional factors that approached statistical significance but may also play a role included stone burden ≥100 mm2 (p = 0.058), the presence of a preoperative ureteral stent (p = 0.052), and the lithotriptor used (p = 0.084). Univariate analysis of 3-month outcomes demonstrated no significant factors to be predictive of single-treatment SWL outcomes (p > 0.1 for all, Table 3). On multivariate analysis, BMI (p = 0.013) and upper calyceal location (p = 0.026) were both found to be important predictors of SWL success. Stone burden approached but did not reach statistical significance (p = 0.074).
Discussion
Treatment of stones in patients with congenital renal anomalies, and HSK in particular, poses a clinical challenge. In part, this is caused by the ectopic location and malrotation associated with the anomaly. The unusual course of the upper ureter, over the isthmus, is often associated with impaired renal pelvic drainage, ureteropelvic junction obstruction, and hydronephrosis. 1 As with normal kidneys, three main treatment options exist. There is considerable published data regarding the efficacy of PCNL in these patients, and its role in patients with large stones is undisputed. However, for patients with a smaller stone burden, less invasive options are desirable, providing that acceptable success rates can be achieved with minimal morbidity. Published data for ureteroscopy are limited to just two reports with a total of seven patients. 2,3 The slow uptake of the technique may be due in part to the inability of currently available flexible endoscopes to access stones in many of these patients. Consequently, achieving stone-free status is problematic, and the recognition that auxiliary procedures are often necessary has likely prevented any group from developing a large experience.
In contrast, SWL is easily administered and well tolerated by the majority of patients. 4 Several groups have recently begun to describe their experience (Table 4). Jenkins et al 5 and Tolon et al were among the first to report the use of SWL in this patient group, but provided no description of their patients or outcome data. 6 The generalizability of other early reports has been limited by their small size and the inclusion of patients with other congenital renal anomalies. In one of the largest series published to date, Demirkesen et al 7 reported data on SWL in patients with upper urinary tract anomalies, including 31 patients with HSK. The majority of patients were either stone-free (45%) or had the so-called clinically insignificant fragments ≤4 mm (48%) after a follow-up of 10 to 12 weeks. However, patients required an average of three treatments to achieve these results. As above, their data were limited by the lack of information specific to patients with HSK as data from 21 additional abnormal kidneys were included in the analysis. Kirkali et al 8 reviewed their series of SWL performed in 18 patients with HSK. The clinical success rate was 78% for fragmentation ≤4 mm, but the stone-free rate was just 28% after a mean follow-up of 6 months. Further, prone positioning was required for targeting in eight patients. Vandeursen et al 9 treated 33 calculi in 11 patients with HSK over a 4-year period. The success rate was 83% and the stone-free rate was 55% after a mean of 3.8 treatments. They found that 18 of 21 (86%) stones located in the lower pole cleared completely.
Where possible, stone-free rate is reported at 3 months.
Although Lampel et al. treated 50 renal units, follow-up data were available for only 29 patients.
In their analysis, Demirkeson et al. included data from 21 patients with congenital anomalies in addition to 31 patients with horseshoe kidney.
n/a = not available.
Two groups with sizeable series have reported SWL results that are comparable to normal kidneys. In 49 patients with HSK treated with two second-generation lithotriptors, Sheir et al 10 reported an overall stone-free rate of 71.4% with an efficiency quotient of 0.42. Prone positioning was adopted in 19 patients. Only the presence of hydronephrosis was found to adversely affect the stone-free rate on univariate analysis. Unfortunately, this group provided no data on treatment parameters or fragmentation rates. 10 In another series, Lampel et al 11 reported on 37 patients; however, follow-up was only available for 29. Their stone-free rate was 76.9% at 3 months, with an overall success rate of 100%. Any patient with HSK and hydronephrosis or delayed drainage on a diuretic renal scan was excluded from SWL and underwent open pyelolithotomy and pyeloplasty, suggesting that results comparable to normal kidneys may be achievable in the absence of these factors. 11
To our knowledge, we report the largest series published to date of SWL in patients with HSK. Overall single-treatment success and stone-free rates 3 months after SWL were 25.0% and 9.1%, respectively. Consequently, 15 patients (51.7%) required at least one additional treatment. However, little incremental benefit was found beyond two treatments in our series (Fig. 2), calling into question the practice of repeated SWL treatments. The overall treatment success rate after a 3-month follow-up was 63.6%, indicating that satisfactory fragmentation does occur with SWL. In contrast, the overall stone-free rate was 39.1% after 3 months. This illustrates the difficulty in treating this patient population. Although satisfactory fragmentation occurs, stone clearance is impaired. This may be because of several factors. Concomitant UPJO occurs in up to one-third of patients with HSK, 1 and hydronephrosis has been shown to adversely affect stone-free rates in these patients. 10,12 Notably, both single-treatment success and stone-free rates dropped between the 2-week and 3-month follow-up appointments in our series. This is because our primary outcome measure was the single-treatment success rate. Our rigorous definition required that any patient experiencing symptoms or who underwent a second SWL procedure was considered as a treatment failure.
Importantly, we have also been able to identify several factors that influence success and stone-free rates before treatment. On multivariate analysis, upper calyceal location and BMI were both associated with failure in patients with HSK. Additionally, stone burden approached, but did not reach, statistical significance. It is possible that any calyceal location will negatively impact stone clearance, a finding that has been seen with SWL in normal kidneys. 13,14 We further hypothesize that BMI may be a surrogate for skin-to-stone distance, a known predictor of SWL success. 15,16 Owing to the ectopic location of HSKs, the renal pelvis is often medially displaced over the lumbar spine. This can have the dual effect of further increasing the skin-to-stone distance 8,10,17 as well as making fluoroscopic targeting more difficult, 8,10 particularly when patients are positioned supine.
In early reports, the etiology of stones in patients with HSK was thought to be secondary to obstruction and infection. 18 In contrast, the primary stone composition in our patients was found to be primarily calcium oxalate monohydrate (83.9%), followed by dihydrate (12.9%) and calcium phosphate (3.2%); none had struvite stones. These analyses mimic the stone composition that we have found in normal kidneys, a finding that has been made by others. However, part of this difference may be caused by case selection as patients with HSK and staghorn calculi were more likely to undergo PCNL rather than SWL. In a study of eight patients with HSK and urolithiasis, two patients had struvite calculi. 19 These authors noted that abnormalities of calcium and urate metabolism occurred in 75% of evaluated patients. In a prospective series, Raj et al 20 found that in 11 patients with a complete metabolic work-up, at least one abnormality was noted in all patients, and a there were an average of 2.7 abnormalities per patient in total. 20 On the basis of these results, it has been recommended that a metabolic evaluation to be undertaken in all HSKs with urolithiasis.
There are several unanswered questions regarding the use of SWL in patients with HSK. Included among these are recommendations for optimal patient positioning and targeting during the procedure. The role for percussion, diuresis and inversion therapy, adjuvant α-blockers, and, perhaps most important in this population, the role for alternate therapies in patients with small-stone burden and hydronephrosis also remain to be determined.
On a final note, although no complications were noted in our series, care must be taken during the use of SWL in these patients. The relationship of other organs to the ectopic kidney may yield unexpected results. Smith et al 17 reported a possible case of focal ischemic colitis or hematoma of the bowel wall secondary to the presence of colon within the focal zone of the lithotriptor.
There are several limitations to our data that deserve mention. First, as this retrospective study included patients from 1994 to present, preoperative axial CT scans were not available for the majority of patients, preventing us from commenting on either the exact nature of the fusion anomaly present, or the presence of concomitant renal anomalies known to coexist with HSK (e.g., ureteral duplication). Thus, the relative importance of these conditions on SWL efficacy remains unknown. Second, as SWL in our unit is limited to patients with radio-opaque stones, the routine follow-up of patients is with KUB. Our data point out that SWL has lower success and stone-free rates in patients with HSKs compared with normal subjects. However, follow-up with CT would be likely to show tiny fragments not seen on KUB, making stone-free rates lower still. We also acknowledge that defining stones ≤4 mm on KUB as clinically insignificant is controversial; however, this is a commonly used definition of SWL success. 28,29 Third, as we lack information regarding treatments received before referral, the importance of prior treatment failure cannot be accounted for in our dataset. We attempted to limit this bias by excluding any patients who had previously received another treatment for their stone in our department. Finally, as a provincial referral center, patients often travel great distances for SWL treatment, and will prefer follow-up with their local urologist. As a result, our follow-up data are incomplete. As we are more likely to have follow-up data on patients who return after an unsuccessful treatment, our results may be negatively biased. However, this bias may have been at least partially mitigated by patients who were referred back to their own urologist because of awareness of the lack of efficacy of a second SWL treatment.
Conclusion
Patients with HSK appear to have lower single-treatment success and stone-free rates after SWL than patients with normal kidneys. Although stone clearance is impaired, treatment is successful with good fragmentation rates and symptom relief in the majority of patients. SWL should be offered to patients with HSK and small renal calculi once limitations in stone clearance have been considered.
Footnotes
Disclosure Statement
No competing financial interests exist.