
Abstract
Purpose:
To directly compare the outcome of laparoscopic radical prostatectomy (LRP) with robot-assisted laparoscopic prostatectomy (RALP) performed by a single laparoscopic surgeon with intermediate experience—one who is between a novice and an expert.
Patients and Methods:
Consecutive 106 patients with prostate cancer who were treated with radical prostatectomy (62 with LRP and 44 with RALP) were included. The preoperative characteristics, the perioperative surgical outcomes, and the functional outcomes were compared between the two groups.
Results:
The mean operative time was longer in the RALP group (371 min vs 308 min, P = 0.00), conceivably because of more nerve-sparing procedures (84% vs 57%). The other perioperative parameters, including the surgical margin, were comparable, except for two major complications (rectourethral fistula and ureteral injury) in the LRP group. The RALP group recovered continence faster than those in the LRP, but the eventual continence rate at 12 months was similar (95% for LRP vs 94.4% for RALP, P = 1.00). The potency rate ≥ 6 months postsurgery was 47.6% in the LRP group and 54.5% in the RALP group (P = 0.65).
Conclusions:
RALP was beneficial for the earlier recovery of continence, although LRP and RALP had comparable safety and efficacy as minimally invasive surgery for prostate cancer when performed by a laparoscopic surgeon with intermediate experience. Long-term follow-up data are needed for further evaluation of oncologic and functional outcomes for both techniques.
Introduction
Robot-assisted laparoscopic radical prostatectomy (RALP) using the da Vinci® Surgical System (Intuitive Surgical, Sunnyvale, CA) was introduced less than a decade ago. 6 The technical advantages associated with this new and popular system include magnified three-dimensional vision, improved dexterity, and improved ergonomics, resulting in a shorter learning curve and theoretically precise dissection of the periprostatic neurovascular structures.
Many studies on either LRP or RALP or comparing both techniques have been published. There are, however, few direct comparisons of LRP with RALP from a single surgeon's experience. We assessed the operative, pathologic, and functional outcomes of LRP and RALP performed during the same period by a single surgeon with intermediate laparoscopic surgical experience. We regarded the laparoscopic surgeon with intermediate experience as one who is between a novice and an expert in laparoscopic surgery.
Patients and Methods
A total of 62 patients with prostate cancer underwent a transperitoneal LRP between October 2007 and March 2009 by a single surgeon (SIS). From January 2008 to March 2009, a total of 44 patients were treated with a transperitoneal RALP by the same surgeon using the da Vinci Surgical System. The LRP was performed in all patients before launching the da Vinci system at our institution. Since its introduction, the RALP has been preferred as the latest technologic advancement in this procedure. The medical expense of the RALP was five to six times higher than the LRP, however, because our national health insurance system does not cover the RALP. Therefore, patients themselves made the final decision of surgical method. The main reason for choosing LRP for patients was medical expenses.
We retrospectively reviewed the medical records with regard to patient history and clinical characteristics of the tumors. The perioperative parameters, including operative time, estimated blood loss (EBL), transfusion, neurovascular bundle preservation, and lymph node dissection, were recorded, and the postoperative factors, including pathologic stage and positive surgical margin (PSM) rate, were considered in the analysis. The postoperative functional outcomes were also assessed in patients who were followed for 6 months or more after surgery.
All patients underwent clinical staging before surgery with a digital rectal examination, prostate MRI, and whole body bone scan by our institution's protocol. The MRI was performed on a 3.0 Tesla unit (Integra Achieva 3.0T, Philips Medical System, Best, The Netherlands) with a phased array coil (6 channels) using T2-weighted imaging, T1-weighted imaging, dynamic contrast-enhanced imaging, and diffusion-weighted imaging.
The LRP and RALP procedures were performed using essentially the same technique: (1) Patients were positioned supine with a Trendelenburg tilt (25 degrees); (2) five ports (two working ports, one camera port, two assistant ports) were needed for LRP and six ports for RALP (three robotic arm ports, one robotic camera port, two assistant ports); (3) development of the prevesical space and incision of the endopelvic fascia; (4) ligation of the dorsal vein complex; (5) division of the bladder neck with the lateral to medial approach 7 ; (6) dissection of the seminal vesicles; (7) incision of the Denonvillier fascia and control of the lateral pedicles with antegrade neurovascular bundle dissection; (8) apical dissection and division of the dorsal vein and the urethra; (9) urethrovesical anastomosis; (10) and pelvic lymph node dissection (PLND). The PLND was routinely performed to a limited extent in patients with Gleason score ≥7 or with a prostate-specific antigen (PSA) level ≥10 ng/mL.
Nerve-sparing procedures were performed for preoperatively potent patients (International Index of Erectile Function-5 score ≥17), except in patients with a strong suspicion of extracapsular extension at MRI finding or a PSA level >10 ng/mL. The total operative time was defined from the first periumbilical incision to complete closure of the trocar sites or skin to skin. The surgical specimens were evaluated for the Gleason score, the location and volume of tumor, ECE, seminal vesicular invasion, surgical margin status, and lymph node involvement. The 2002 Tumor-Node-Metastasis staging system was used for the clinical and pathologic staging.
In some initial cases of LRP, cystography was routinely performed 5 days after surgery, and the Foley catheter was removed when no urine leakage was confirmed. Thereafter, postoperative cystography was performed only if leakage was noted in the filling bladder after urethrovesical anastomosis during surgery. Otherwise, the catheter was removed between 7 to 10 days after surgery without cystography in both groups. If a cystogram showed leakage at the vesicourethral anastomosis site, the catheter was kept in place for another 2 weeks before radiologic reassessment.
Urinary continence was defined as use of no or one security liner a day. It was evaluated at 1, 3, 6, and 12 months after surgery by patient interview. Potency was defined as the presence of spontaneous or phosphodiesterase-5 (PDE-5) inhibitor assisted erections sufficient for vaginal penetration; this was assessed by patient interview among those who had nerve-sparing surgery and were followed for more than 6 months.
Statistical analysis was performed with the Student t test and Mann-Whitney U test for comparison of the numerical variables and the chi-square test and Fisher exact test for comparison of the categorical variables, using SPSS 15.0 (SPSS Inc., Chicago, IL). A P value <0.05 was considered statistically significant.
Results
Patient demographics showed that the RALP cohort was younger, had a higher body mass index (BMI), and lower PSA levels than the LRP cohort. There was no significant difference, however, in the calculated prostate volume and the distribution of Gleason scores between the two groups. The clinical stages of the two groups were also similar (Table 1).
BMI = body mass index; PSA = prostate-specific antigen; LRP = laparoscopic radical prostatectomy; RALP = robot-assisted laparoscopic radical prostatectomy.
The mean operative time, defined as “skin to skin,” was significantly shorter in the LRP cohort than in the RALP cohort (308 min vs 371 min, P = 0.00). In terms of a learning curve, the operative time gradually decreased in both cohorts; it decreased faster and appeared constant after the 15th case in the RALP cohort, whereas a gradual decrement but steeper curve was found in the LRP cohort (Fig. 1). When the two groups were divided as earlier and later halves, by chronologic order, the LRP cohort also showed a shorter operative time than the RALP cohort.
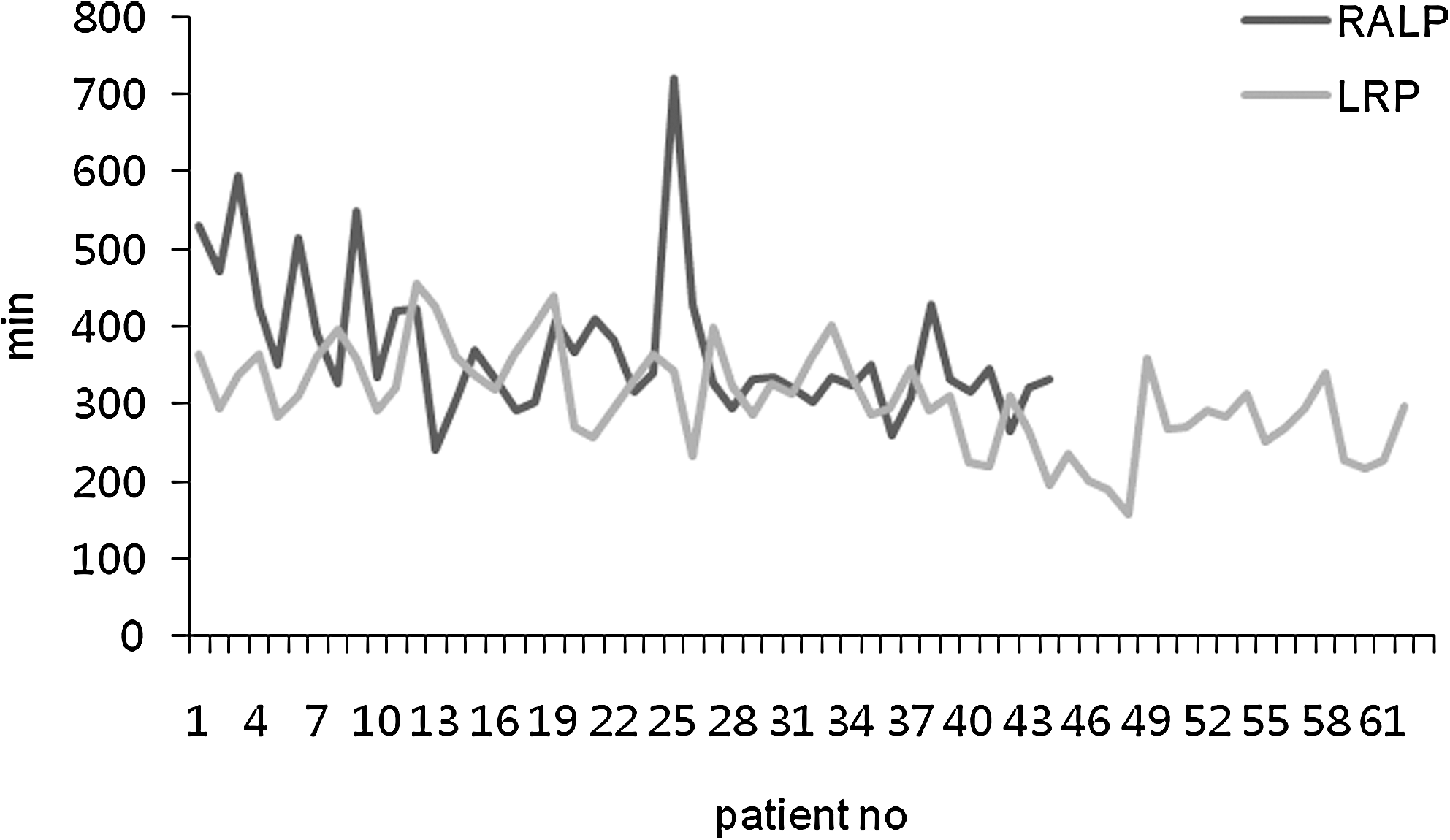
The learning curve (operation time) of laparoscopic radical prostatectomy and robot-assisted laparoscopic prostatectomy. LRP = laparoscopic radical prostatectomy; RALP = robot-assisted laparoscopic prostatectomy.
The mean EBL was similar in both cohorts (220 mL for RALP vs 214 mL for LRP, P = 0.83). No blood transfusion was given during the operation, although one patient, in the RALP group, received 2 units of red blood cells after the surgery. The hematocrit (Hct) decreased more in the RALP group on the first postoperative day (−6.5% vs −1.7%, P = 0.44); this was not a statistically significant difference. By the fifth postoperative day, however, the Hct was similar in the two groups (−6.9% vs −7.4%, P = 0.63).
More nerve-sparing procedures were performed in the RALP group (84.1% vs 56.5%, P = 0.01). There were no differences in the number of PLND procedures and in the number of obtained lymph nodes between both groups. No significant difference was found in the length of hospital stay and the duration of indwelling Foley catheters between the two groups (Table 2). There was no open conversion or robotic to conventional laparoscopic conversion.
EBL = estimated blood loss; Hct = hematocrit; PLND = pelvic lymph node dissection.
The pathologic stage was comparable in the two groups, with a median Gleason score of 7. The overall PSM rate was similar: 21% in the LRP group and 20% in the RALP group (P = 0.95). The site of the PSM showed a relatively even distribution in the apex, lateral margin, and bladder neck in the two groups (Table 2). Perioperative and postoperative complications developed among 11.3% (7 of 62) of the LRP patients and 11.4% (5 of 44) of the RALP patients.
Postoperative urinary continence recovered gradually. The continence rates at 1, 3, 6, and 12 months were 24.6%, 55.8%, 76.3%, and 95% in the LRP group and 66.7%, 88.6%, 93.5%, and 94.4% in the RALP group, respectively (Fig. 2). Erection sufficient for vaginal penetration with or without an oral PDE-5 inhibitor was present in 12 of 22 (54.5%) patients in the RALP group and in 10 of 21 (47.6%) patients in the LRP group who were followed for more than 6 months after a unilateral or a bilateral nerve-sparing procedure (P = 0.65).
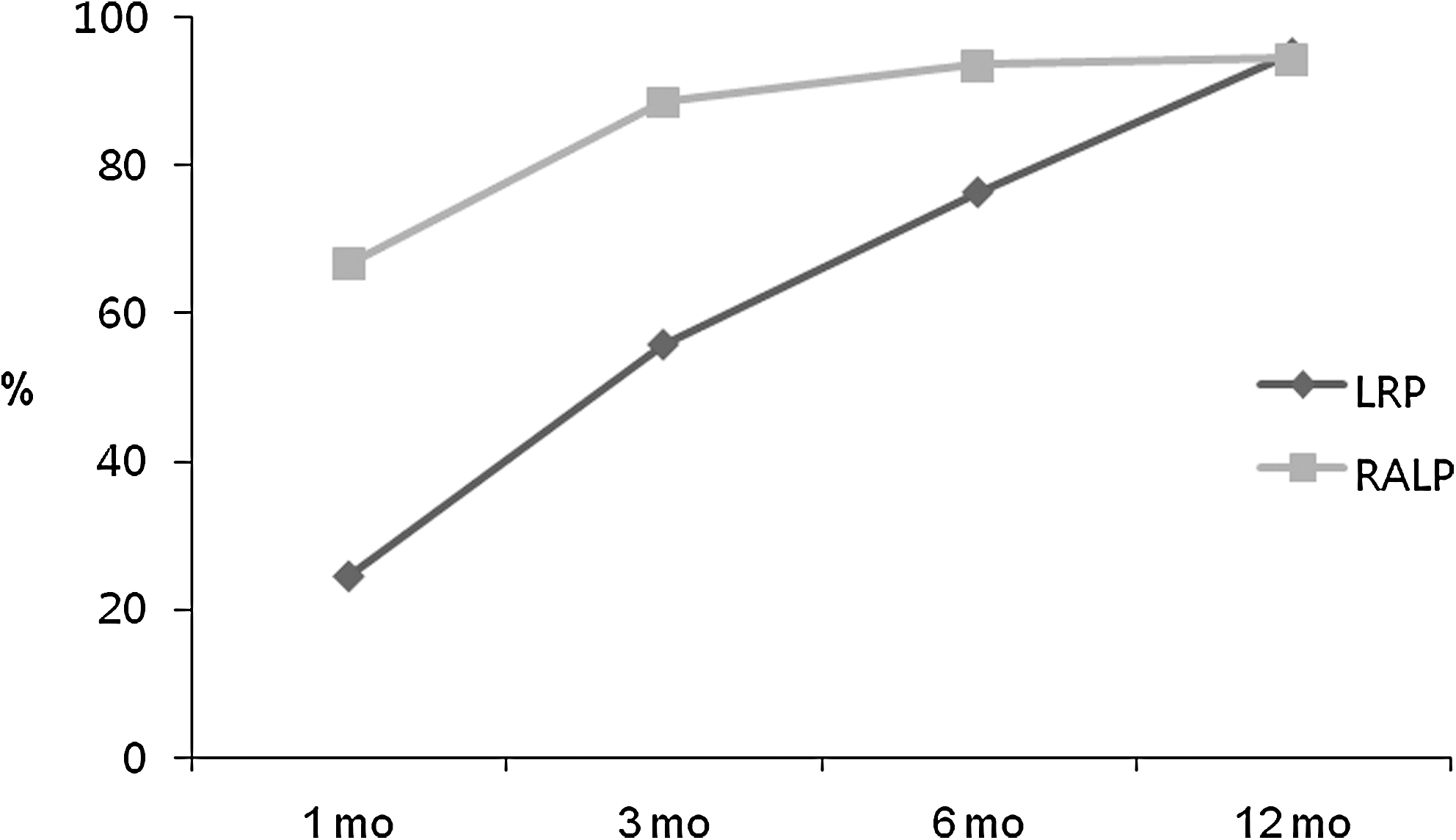
The recovery rates of continence after laparoscopic radical prostatectomy and robot-assisted laparoscopic prostatectomy. LRP = laparoscopic radical prostatectomy; RALP = robot-assisted laparoscopic prostatectomy.
Discussion
Radical prostatectomy remains the gold standard for treatment of patients with localized prostate cancer. Laparoscopic procedures were first introduced by an American group in the early 1990s. 1 They found that it was a feasible surgical approach; however, they also noted that the procedure had limitations and was not as effective as open prostatectomy with regard to outcomes and available instruments. In the United States, the steep learning curve for the LRP hindered its expansion into mainstream urologic practice. 8,9 In 1999, Guillonneau and Vallancien 10 reported their pioneering results of 65 cases of LRP, suggesting that it could become a routine urologic procedure. Since then, the LRP has gained interest worldwide and is becoming a standard procedure in many institutions, mainly in the European countries.
The use of robotic technology for a radical prostatectomy offers many theoretical advantages over conventional LRP, including three-dimensional visualization, magnification, increased seven degrees of freedom, absence of the fulcrum effect, and robotic-wrist instrumentation so that one can overcome the technical difficulties associated with the LRP. These advantages have led to the rapid use of the robotic system throughout the world.
For the laparoscopically naïve surgeon, the learning curve necessitates as many as 50 to 100 LRPs. 11 –14 All of the aforementioned advantages of RALP contribute to successfully reducing the learning curve that is associated with LRP. Although there is no accepted standard for either procedure for the definition or measurement of the learning curve, it usually is the self-declared point at which a surgeon becomes comfortable performing the procedure. Thus, the learning curve could vary considerably, depending on the surgeon's direct or indirect experience or results with alternative surgical approaches.
Several studies that compared the surgical and oncologic results of LRP and RALP have been published. Most of these reports, however, were either from a multi-institutional and/or multisurgeon perspective or involved the comparison of a highly experienced laparoscopic surgeon's LRP series with an initial RALP series. The present study is a direct comparison of the early results of a single surgeon, who had some laparoscopic ablative and reconstructive surgical experience but was on the learning curve for LRP and RALP.
In terms of mean operative time, our results were longer compared with previous reports, conceivably because of the learning curve. The operative time for the RALP cohort was longer than for the LRP cohort (371 min vs 308 min). This was likely because of the greater number of nerve-sparing procedures (84% vs 57%) and higher BMI in the RALP group, as previously reported by Poulakis and associates. 5 In the non–nerve-spared subgroups of both techniques, there was no significant difference in the operative time.
We did not find significant differences in other intraoperative or perioperative factors between the LRP and the RALP groups, including EBL, postoperative decrease of Hct, PLND dissection rate, number of obtained lymph nodes, length of hospital stay, and bladder catheterization days. The mean EBL of our result was 214 mL in the LRP patients and 220 mL in the RALP patients; only one RALP patient needed a transfusion after surgery.
When compared with the other results in the literature, our blood loss was significantly less than 813 to 1550 mL in the RRP series, 2,15 less than the 380 to 800 mL for LRP, 2,16 and similar to the 206 to 256 mL for RALP. 17,18 Because the blood loss reported is for our early series, hopefully further reduction of blood loss will occur with experience. Not all the intermediate- or high- risk patients underwent PLND because of low yield of positive nodes in those patients from our institution's prostatectomy database and technical difficulty in early cases of our series.
Because the foremost goal of less invasive surgery is to achieve oncologic outcomes equivalent to those of open surgery while reducing the inherent morbidity that is associated with the conventional open counterpart, the pathologic results are one of the most important aspects to consider. PSMs are unique predictors of tumor progression and decreased cancer-specific and overall survival. 19 In our series, the pathologic stages were comparable between the two groups, and the PSM rates also showed no significant difference between the groups (21% in LRP vs 20% in RALP). These results were generally comparable to those of previous reports: 18.9% to 28.7% for RRP, 2,15,20 16.7% to 36.7% for LRP, 2,16,20 and 10.5% to 35.5% for RALP. 9,14,17,18 Interestingly, RALP had a higher PSM rate than LRP with pT2 stage disease, and LRP had a higher PSM than RALP with pT3 stage disease; however, these differences were not statistically significant. Salomon and coworkers 20 reported a specific high-risk location for PSM by the surgical approach; they reported that the posterolateral margin was specific for the laparoscopic approach; however, the location of the PSM was evenly distributed among the apex, bladder neck, and lateral margins in our study.
We did not investigate the biochemical failure rate in this study because of the relatively short follow-up duration. Long-term biochemical failure rates and disease-specific survival rates of both techniques are to be investigated later to compare oncologic outcomes.
Our complication rate was 11.3% and 11.4% for LRP and RALP, respectively. Among the seven complications in the LRP group, two cases (one ureteral injury and one rectourethral fistula) were classified as major complications whereas all of the five complications in the RALP cohort were minor and could be managed conservatively. Previous reports that have directly compared LRP with RALP reported an overall higher complication rate either for LRP 21,22 or RALP. 23 These results, however, were based on comparisons between experts performing LRP and the initial results of RALP; therefore, the surgeon's experience affected the outcome.
Continence, after a radical prostatectomy, is difficult to compare among studies because the definition varies among investigators. Furthermore, former studies usually involved multiple surgeons at different levels of training and laparoscopic surgical experience. All of these factors limit the direct comparison of continence outcome for LRP and RALP. Our continence rates showed a more rapid recovery in the RALP group until 3 months after surgery; the results were similar in both groups from 6 months after surgery. This was comparable to another report of a single-surgeon experience performing LRP and RALP. 22 The advantages of the RALP such as improved surgical vision and improved ergonomics enabled meticulous apical dissection, providing the patient with sufficient length of urethral stump, which in turn was thought to affect early recovery of continence.
Potency is another factor that affects the quality of life of patients after a radical prostatectomy. Progressive improvement of potency was observed during follow-up. Potency at 12 months after nerve-sparing RALP has ranged from 20% to 97%. 24,25 In our series, albeit the follow-up duration was not sufficient to draw a significant conclusion, the potency rates of the two cohorts were comparable at 6 months after nerve-sparing surgery; therefore, LRP was not inferior to RALP with regard to the preservation of potency. Long-term follow-up is necessary, because recovery of potency can occur up to 18 months after surgery.
Limitations of the present study include the following: Relatively small size of the cohorts, relatively short follow-up, some differences in the patient demographics, and nonrandomization of the subjects. Thus, different age, PSA, and BMI of both groups might be a potential source of bias. The goal of the current study was to compare the results of LRP and RALP, with regard to the possible influence of a surgeon's previous laparoscopic surgical experience on the results. There were no significant differences in surgical and functional outcomes between the two procedures, although the surgeon was on the learning curve of both procedures. Further study is needed to assess long-term oncologic and functional outcomes for both techniques. This is the first study from an Asian country that directly compared the results of LRP and RALP performed by a single surgeon.
Conclusions
In this direct comparison of the early results of LRP and RALP, performed by a single surgeon with intermediate laparoscopic surgical experience, the findings showed that RALP was beneficial for the earlier recovery of continence, although both techniques had comparable safety and efficacy as minimally invasive surgery for prostate cancer. Longer follow-up data are needed to further assess whether one technique is superior to the other after completion of the learning curve.
Footnotes
Disclosure Statement
No competing financial interests exist.