
Abstract
Purpose:
To assess effectiveness of flexible ureteroscopy (fURS) in patients not with simple but with multiple unilateral renal stones.
Patients and Methods:
A database analysis was performed to identify patients with multiple unilateral intrarenal stones. Patients were treated using an 8.8F flexible ureteroscope. Patients were considered stone free if no residual stones were seen endoscopically and radiographically after the procedure. The efficiency and the safety of the procedures were analyzed.
Results:
Between 2006 and 2008, 1054 ureteroscopic procedures were performed in our department; 125 patients met the inclusion criteria. Holmium:yttrium-aluminum-garnet laser lithotripsy was necessary in 41 (32.8%) patients. The mean stone size was 11.93 ± 8.2 mm, with a mean stone burden of 83.7 ± 67.66 mm2. The mean number of stones was 3.59 ± 3.57. Twenty-six (20.8%) patients had a stone burden ≥100 mm2, and 99 (79.2%) a stone burden <100 mm2. The overall stone-free rate after a single procedure of fURS was 74.4%. In the remaining 32 patients with residual stones, the mean stone burden dropped from 123.24 ± 84.36 mm2 to 56.28 ± 52.53 mm2. The stone-free rate in patients with a stone burden ≥100 mm2 was 65.4% and 79.5% in patients with a stone burden <100 mm2, respectively. Complications have been recorded in seven (5.6%) patients, including urinary tract infection in four, ureteral perforation in one, and hematuria in two patients. No major complications occurred. All patients were treated conservatively.
Conclusions:
fURS is an effective treatment option in patients with multiple unilateral renal stones. Single procedure stone-free rates are high with a low rate of only minor complications.
Introduction
With the development of smaller caliber semirigid and flexible ureteroscopes, as well as the advances in the deflectable tip, visual quality, and durability, and the introduction of improved instrumentation, including the holmium:yttrium-aluminum-garnet (Ho:YAG) laser, flexible URS (fURS) has evolved into a safer and more efficacious modality for management of stones in all locations with increasing experience worldwide. This improvement in technology has expanded the potential indications of fURS to include intrarenal small and large stones (>25 mm), with stone-free rates up to 90%, besides SWL failure, infundibular stenosis, morbid obesity, renoureteral malformations, musculoskeletal deformities, and bleeding diathesis. Moreover, URS can be used to safely simultaneously manage bilateral ureteral stones in selected cases. 2,4 –9
Even though neither the EAU 1 nor the AUA 2 guidelines recommend URS as a treatment of choice for intrarenal stones, fURS with intracorporeal lithotripsy can be considered a first-line treatment for multiple intrarenal calculi in selected patients, with a high stone-free rate and low morbidity. 10 To reinforce this hypothesis, we investigated the use of fURS and intracorporeal lithotripsy specifically for the management of multiple intrarenal unilateral stones in our institution by evaluating the effectiveness of a single fURS procedure in patients with multiple unilateral renal stones.
Patients and Methods
Our database for urolithiasis was retrospectively reviewed regarding fURS for multiple unilateral renal stones. The indications for fURS were: Multiple intrarenal stones in patients in whom SWL, URS, or PCNL had failed; obesity; and patient preference (ie, the decline of SWL or PCNL) after a thorough explanation of the advantages and disadvantages of fURS (ie, high risk of stone-free failure). Contraindications for fURS included severe hydronephrosis with renal shrinkage and nondependently draining collecting system (ie, high insertion of the ureter, horseshoe kidney). Informed consent was obtained from all participants before treatment.
All patients underwent retrograde pyelography before ureteroscopy to define the collecting system anatomy and to ensure that the stones were not harbored within a diverticulum or the kidney parenchyma. The total stone burden was calculated (retrospectively measured as the cumulative surface of the intrarenal stones in mm2) with the Picture Archiving and Communications System. The fURS was performed with an 8.8F flexible ureteroscope (Viper, R. Wolf, Knittlingen, Germany). Antibiotic prophylaxis with a second-generation cephalosporin was administered intraoperatively. An ureteral access sheath catheter (9.5/11.5F) was placed to facilitate stone extraction when ≥3 ureteral passages with the ureteroscope were suspected.
If lithotripsy was necessary, we performed it with a Ho:YAG laser (Sphinx, LisaLaser, Katlenburg, Germany) in combination with a 272 μm laser fiber (FlexiFib, LisaLaser, Katlenburg, Germany). For stone retrieval, 1.5 or 2.2F tipless nitinol baskets (NCircle/Ngage, Cook Medical, Limerick, Ireland) were used. Postoperatively, a Double-J stent was placed based on surgeon decision.
At the end of the operation the stone-free status was defined with the absence of any stone fragments right after an ureteroscopic visualization. In addition, transoperative retrograde pyelography was performed to identify residual stones and to exclude any lesion of the ureter or renal pelvis. All patients underwent renal ultrasonography as a routine study the day after URS to ensure the absence of hydronephrosis and a radiographic study in the case of ureteral stent control and/or residual stone.
Statistical analysis was performed by using the calculating program SPSS (SPSS, Inc., Chicago, IL, version 11.5.1) for Windows. The data were expressed as the mean ± standard deviation.
Results
Between January 2006 and December 2008, 1054 ureteroscopic procedures were performed at our department; 125 patients were treated with fURS for multiple renal stones and met the selection criteria. Ho:YAG laser lithotripsy was performed in 41 of 125 patients (32.8%). Mean age at ureteroscopy was 51.31 ± 15.6 years (range 11–85 y). There were 73 males and 52 females (Table 1). Twenty-five (20%) patients had previously received one session of SWL, URS was previously performed in four (3.2%) patients at another institution, and fURS was performed in 10 (8%) patients after a PCNL procedure. Ninety-six (76.8%) patients had a Double-J stent placed before the procedure. A postoperative Double-J stent was placed in 54 (43.2%) patients for 2 to 4 weeks.
Data presented as number of patients, mean ± standard deviation.
BMI = body mass index; DJ = Double-J; SWL = shockwave lithotripsy; URS = ureteroscopy; PCNL = percutaneous nephrolithotomy.
The patient stone demographics are shown in Table 2. The mean stone size was 11.93 ± 8.2 mm (range 2–50 mm), with a mean stone burden of 83.7 ± 67.66 mm2 (range 5.03–348.40 mm2). Twenty-six (20.8%) patients had a stone burden ≥100 mm2, and 99 (79.2%) patients had a stone burden <100 mm2. The mean stone number per patient was 3.59 ± 3.57 (2–33). The mean operative time per patient was 65.15 ± 36.26 minutes (range 17–199 min). The operative time was calculated from the time of cystoscope insertion to the completion of the procedure.
Data indicated as mean values ± standard deviation.
OR = operating room.
The overall stone-free rate after a single procedure of fURS was 74.4%. Of the 32 patients with residual stones after one fURS procedure, the mean stone burden, however, dropped down from 123.24 ± 84.36 mm2 (range 42.64–305.73 mm2) to 56.28 ± 52.53 mm2 (range 14.19–178.6 mm2); 12 patients underwent a second URS procedure, 5 were treated with PCNL (4–8 weeks later), and the remaining 15 patients had spontaneous passage. In addition, the stone-free rate in patients with a stone burden ≥100mm2 was 65.4% and 79.5% in patients with a stone burden <100mm2 after one procedure, respectively.
Complications were recorded in seven (5.6%) patients, including urinary tract infection in four, ureteral perforation in one, and hematuria in two patients, respectively. No major complications occurred. All patients were treated conservatively with antibiotics and/or prolonged Double-J stent placement in the ureter of up to 4 weeks. The postoperative course was uneventful in these patients. Follow-up intravenous urography (IVU) 1 month after Double-J stent removal documented resolution of extravasation.
Discussion
Although technologic advances in fURS make most areas of the kidney accessible, indications for ureteroscopic management of renal calculi remain debated. Because of the small number of prospective comparative study publications, neither the EAU 1 nor the AUA 2 guidelines recommend ureteroscopy as a first-line treatment of choice for single or multiple unilateral renal stones.
SWL has traditionally constituted the favored approach for small to moderate size intrarenal calculi (<20 mm), although ureteroscopy has assumed an increasing role in recent years. The highest stone-free rates (80%–88%) were achieved with SWL to calculi in the renal pelvis. Success rates are lower in the upper pole (73%), midpolar (69%), and lower (63%) pole calices. 3,9,11 –15 When multiple intrarenal stones are managed with SWL, however, the stone-free rate drops down to 50% to 55%. 1 –3,16
Possible advantages of SWL in the management of renal stones are patient acceptance, short convalescence, and the lack of a requirement of anesthesia during the procedure. 3,12 The outcome, however, is influenced by patient characteristics, such as body mass index, pelvicaliceal anatomy, and stone number, composition (ie, cystine and calcium oxalate monohydrate), and location (ie, lower pole). 17,18 Besides, SWL is contraindicated in pregnancy and in patients with bleeding disorders, and should not exceed 3 to 5 sessions, 1 which sometimes are necessary in patients with multiple stones or stones in multiple locations.
PCNL, on the other hand, has a significantly higher stone-free rate than SWL (86%–100%) and is the standard of care for single, complex (>20 mm), or >10 mm lower-pole stones as well as for multiple intrarenal stones. It is associated, however, with greater morbidity than either SWL or URS, 3,19 –21 which has been reported in up to 83% of cases. 22 Complications arise mainly from the percutaneous puncture, associated with bleeding secondary to renal parenchymal damage, and adjacent structures injuries, such as colon (0.8%) and pleura (3.1%) causing septicemia (4.7%). 22 Even when up to 95% of stones can be removed with a single procedure, 23 multiple caliceal stones may necessitate multiple access tracts, which increase the risk of complications and discomfort. 24
Advances in flexible ureteroscopes, allowing detailed caliceal examination, and the introduction of Ho:YAG laser lithotripsy, allowing fragmentation of all stone types, even in dustlike particles, as well as the improvement in ureteroendoscopic instrumentation, such as nitinol stone baskets without interfering with the scope deflection grade, 25 have made ureteroscopy an alternative to SWL and PCNL for managing renal calculi. 3 Besides, fURS is useful in the management of stones in a caliceal diverticulum or in a horseshoe kidney, where stone-free rates with SWL are typically low because of poor fragment clearance.
URS offers the low morbidity of SWL but the potential stone-free rates approaching those of PCNL for small to moderate size renal calculi. Fabrizio and associates 13 reported a 77% stone-free rate for renal stones <10 mm and 50% for >16 mm stones with a complication rate of 3%. Breda and colleagues 6 reported a stone-free rate of 93.3% after an average of 2.4 procedures for single renal stones larger to 20 mm without major complications. Riley and coworkers 4 reported after an average of 1.8 procedures a 90.9% stone-free rate for single intrarenal mean stone size of 30 mm. The authors have found that significant lower pole stone burden is a limiting factor for success. The lower pole is the most difficult part to access; even with the new flexible ureteroscopes, the lower pole calices can be accessed only in 93% of cases. 7
There are only a few published reports on ureteroscopic management of multiple unilateral intrarenal stones. 7,9,10,13,19 Breda and colleagues 10 reported results of 51 patients with overall stone-free rates after one and two procedures of 64.7% and 92.2%, respectively, for multiple unilateral intrarenal stones: 85.1% for a stone burden >20 mm and 100% for a stone burden <20 mm with a complication rate of 13.6%.
In our study, we decided to measure the stone burden by a cumulative two-dimensional stone surface area (mm2) 26 in addition to the typical stone length (mm). We believe that this fashion is more representative of stone volume compared with stone length; either the stones were all located in the lower pole or distributed within the pelvicaliceal system (Fig. 1).
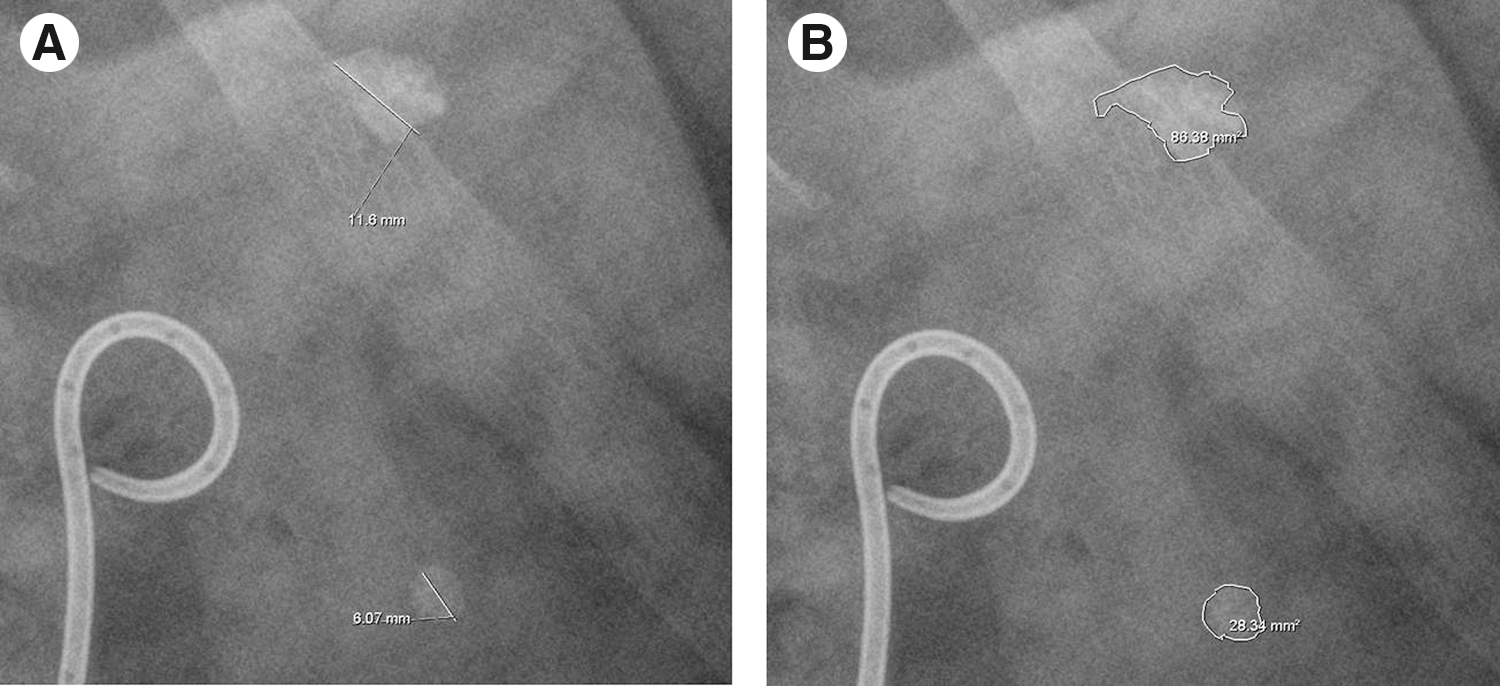
Cumulative stone length vs stone surface. (
So far, this is the largest series reported for multiple renal stones managed with furs. Our results are comparable to those previously published, with an overall stone-free rate after a single procedure of 74.4%. The combination of current generation flexible ureteroscopes and the Ho:YAG laser allows for excellent fragmentation rates in an outpatient procedure, with low postoperative complications. 27 We have used the Ho:YAG laser for stone fragmentation in 41 (32.8%) patients. Our study supports the usefulness of nitinol tipless stone baskets and ureteral access sheath to manage stones throughout the renal collecting system with a high success rate. 10,13,28,29 Recent reports indicate that the overall complication rates of URS are between 6% and 16%. 13,30 Our overall complication rate was 5.6% (seven patients), counting only minor complications: four patients with urinary tract infection who were treated with intravenous antibiotics; one patient who presented extravasation of contrast material and was treated with prolonged Double-J stent placement (up to 4 weeks) and IVU 1 month later without further alterations; and two patients with moderate hematuria that led to the procedure being aborted.
Conclusions
This is the largest series data reported, and our results suggest that fURS is an effective treatment option in patients with multiple unilateral renal stones; it has shown a high success rate with only a few minor complications. Given its safety and efficiency, we believe fURS can become a first-line option of treatment for these patients.
Footnotes
Disclosure Statement
No competing financial interests exist.