
Abstract
Objective:
Single-incision surgery is by now practicable in many fields of surgery, including surgery of the adrenal gland. We report on first experience with laparoscopic transperitoneal and retroperitoneoscopic single-incision adrenalectomy.
Patients and Methods:
Between September 2009 and February 2010, eight patients underwent single-incision adrenalectomy. Four patients received single-incision retroperitoneoscopic adrenalectomy, and four patients transperitoneal single-incision laparoscopic adrenalectomy. Technical feasibility and perioperative data are presented.
Results:
All patients had benign adrenal tumors (Conn's adenoma, n = 7; pheochromocytoma, n = 1). Tumor size ranged between 1.2 and 2.4 cm. Mean operation time was 76 minutes for single-incision retroperitoneoscopic adrenalectomy and 82 minutes for single-incision laparoscopic adrenalectomy. Blood loss was irrelevant in both groups.
Conclusions:
Single-incision adrenalectomy is safe and feasible in appropriate operation time, both by the retroperitoneoscopic technique and by the laparoscopic technique. It is also associated with good cosmetic outcome.
Introduction
Patients and Methods
Between September 2009 and February 2010, single-incision adrenalectomy was applied in eight patients at the University Medical Center Regensburg. Four patients received SIRA, and four patients were operated by transperitoneal SILA in lateral flank position.
Only patients with a body mass index <35 kg/m2 and small adrenal tumors (<3 cm) were included in this study. Tumor localization was an important factor for choice of access. Since liver retraction is necessary during conventional right transperitoneal laparoscopic adrenalectomy, four or five ports are required in most cases. Therefore, only patients undergoing left transperitoneal laparoscopic adrenalectomy were included in the SILA group. All feasible tumors of the right adrenal gland were operated retroperitoneoscopically. Patient data are shown in Table 1. In addition, operating time, blood loss, and intra- and postoperative morbidity were documented. All patients with Conn's syndrome had been treated with spironolactone 100 to 200 mg daily during 6 weeks before surgery. Both patients with pheochromocytoma received alpha- and beta-adrenergic blockade 2 weeks before surgery.
SILA = single-incision laparoscopic adrenalectomy; SIRA = single-incision retroperitoneoscopic adrenalectomy.
Surgical technique
Single-incision right retroperitoneoscopic adrenalectomy
Surgery is performed in prone position. The procedure is started by a 2-cm incision below the 12th rib (Fig. 1a). Subsequently, fibers of the quadratus lumborum muscle are spread and the Gerota fascia is opened dorsally. After reaching the retroperitoneal space, this area is dilated with the forefinger as previously described. 10,12 The same instruments are used for laparoscopic and retroperitoneoscopic techniques (30°-Endoscope, Karl Storz, Tuttlingen, Germany; Harmonic scalpel 5 mm, Ethicon Endosurgery, Hamburg, Germany; 5 mm-roticulating-graspers, Covidian, Neustadt, Germany; and recovery bag, Applied Medical, Rancho Santa Margarita, CA). Afterward, a multilumen system that permits the application of a 10-mm port for the camera is placed. Operation starts with retroperitoneoscopic exploration and insertion of two 5-mm ports through the multilumen system in which a roticulating instrument or the Harmonic scalpel is introduced (Fig. 1b).

Operative steps of a single-incision retroperitoneoscopic adrenalectomy (SIRA). (
After blunt preparation of the retroperitoneal space, the operation is continued by dissection of the retrorenal fat tissue from the renal capsule at the upper renal pole. After observation of the vena cava, the adrenal vein is identified, closed with 5-mm titanium clips and transected. Subsequently, dorsal, lateral, and cranial mobilization of the tumor is performed. Thereby, it is recommended to carry out preparation of the upper part of the adrenal gland as the last step to avoid elevation of the tumor. To remove the specimen, one 5-mm port is removed, and a 10-mm retrieval bag is introduced into the retroperitoneal space through the other 5-mm port (Fig. 1b). The flexibility of the multiport system permits placement of 10-mm instruments through the small aperture. Drainage placement was not necessary in any case. Finally, the fascia at the single incision and the skin are closed (Fig. 1d).
Transperitoneal SILA
Surgical steps of the transperitoneal laparoscopic technique were previously described. 12 Patients are placed in a 45°–60° right lateral flank position. A 2-cm incision is performed 3 cm below the left costal arch in the anterior medioclavicular line (Fig. 2a). After division of fat tissue and fascia, muscle fibers are spread and the peritoneum is opened. The multilumen system is placed. The intraabdominal pressure is kept at 12 mm Hg. The left colonic flexure is mobilized along the Gerota fascia. The avascular plain between pancreatic tail and kidney was dissected through, and the spleen and the pancreatic tail are moved medially, which results in an open-book view. Subsequently, fat tissue at the upper part of renal capsule is mobilized (Fig. 2b).

Operative steps of a single-incision laparoscopic adrenalectomy (SILA). (
The fat tissue surrounding the adrenal gland is left in place to avoid tumor manipulation. Afterward, the adrenal vein is identified and transected between clips in all cases. Dorsal mobilization of the tumor is performed, followed by lateral and cranial mobilization. The adrenal gland and the surrounding fat tissue are removed en bloc with a retrieval bag through the multilumen system. The fascia and skin are closed (Fig. 2c).
Results
Seven patients presented with Conn's syndrome, and one with pheochromocytoma. All patients were symptomatic and all required antihypertensive treatment. Patients with Conn's adenoma had an average serum potassium level of 2.4 mmol/L (1.7–3.2 mmol/L) and all had a pathological aldosterone/renin ratio (A/R R) of median 54 (41–103). Bilateral tumors were found in one case. Adrenal venous sampling revealed an A/R R of 69 on the left side and 4.2 on the right side, leading to one-sided operation via left laparoscopic adrenalectomy in this particular patient.
There was no significant difference regarding operating time between both groups. Duration of surgery could be reduced from 102 to 45 minutes in SIRA and from 110 to 56 minutes in SILA. The blood loss was irrelevant (Table 2).
There were no intra- or postoperative complications and no conversions. All patients were discharged from hospital with a good cosmetic result. Patient data, results of imaging studies, and postoperative specimens are demonstrated in Table 1 and Figures 3 and 4.

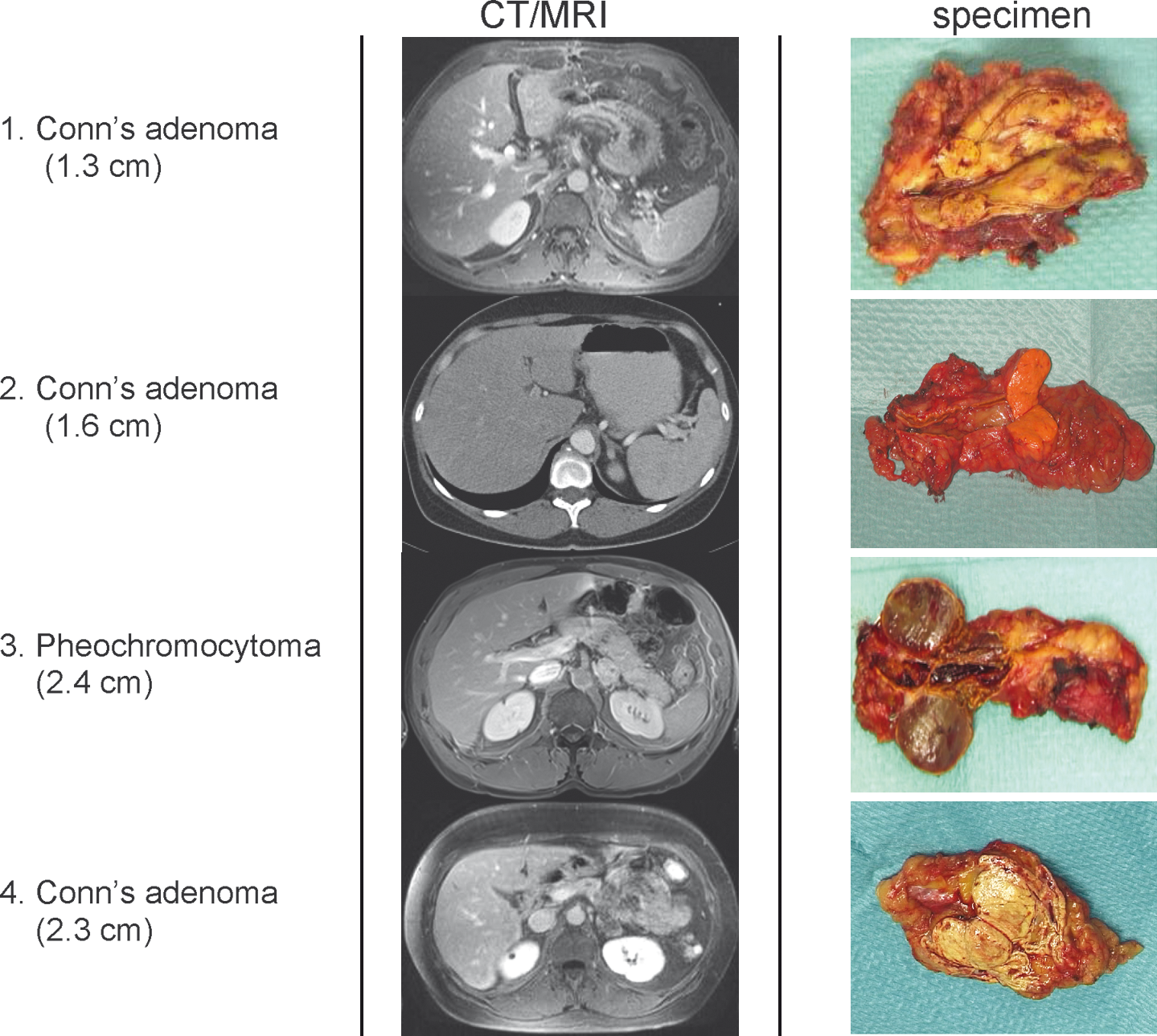
Preoperative imaging studies and postoperative specimens of four patients undergoing SIRA.
Preoperative imaging studies and postoperative specimens of four patients undergoing SILA.
Discussion
During the last decade, single-incision laparoscopic surgery was used in patients undergoing cholecystectomy, urologic, and bariatric surgery. 3 –5 To date, only case reports and small series on single-incision adrenalectomy have been published. 6,7,13 –15 To our knowledge, this study is the first published series about laparoscopic and retroperitoneoscopic single-incision adrenalectomy.
Our study shows that small hormone-active tumors are particularly eligible for single-incision adrenalectomy. Patients with Conn's adenoma are especially suitable candidates for SILA/SIRA because an overwhelming majority of these tumors are small and benign. In our study, the largest Conn's adenoma measured 2.5 cm.
Obesity is associated with serious difficulties in performing retroperitoneoscopic adrenalectomy, because the retroperitoneal space is compromised by redundant fat tissue. Probably, with increased experience, single-incision adrenalectomy will be possible even in patients with a higher body mass index by transperitoneal laparoscopic route. All four right adrenal tumors have been operated by retroperitoneoscopic technique (SIRA), since transperitoneal technique (SILA) would require an additional port for retraction of the liver.
Our study shows the technical feasibility of both surgical procedures. More than 300 retroperitoneoscopic and transperitoneal adrenalectomies have been performed at our center during the last decade. Our preliminary experience shows that both SIRA and SILA reveal significant technical similarities to conventional multiple-trocar procedures, leading to a short learning curve in experienced adrenal surgeons.
The main advantage of the single-incision surgery is its cosmetic result. However, published data show broad variations regarding the length of incision. Hirano et al 14 described in 2005 an extirpation of a 2.6-cm adrenal tumor through a single incision of 4.5 cm. This surgery was performed retroperitoneoscopically in the lateral flank position with the aid of a proctoscope without CO2 insufflation. Even an incision of 9 cm was reported by Kageyama et al. 15 Length of incision never exceeded 2 cm in our study.
There are numerous technical challenges when performing single-incision laparoscopic surgery: limited mobility of laparoscopic instruments, use of multiple trocars, and complexity of orientation. 16 In our opinion, the camera should be placed through the lower aperture of the multiple port system to avoid interference of instruments, thus reducing loss of the intraabdominal/retroperitoneal pressure. We cannot confirm the experience of Castellucci et al, 13 who described limited observation and safety of vessel control in SILA.
We were able to reduce surgery time from 102 to 45 minutes for SIRA and from 110 to 56 minutes for SILA. Longer operation time for single-incision procedures than that for multiple incision laparoscopic techniques seems to be acceptable. Operation time ranged from 120 to 240 minutes in published cases. 7,13 However, Walz and Alesina 6 reported on five cases of retroperitoneoscopic adrenalectomies performed by the technique similar to ours conducted in 35 to 70 minutes.
Conclusion
Single-incision transperitoneal and retroperitoneoscopic adrenalectomy can be performed with same safety as conventional endoscopic procedures. Improved cosmetic results can be achieved by these techniques. Expectedly, larger tumors and obese patients will qualify for SILA/SIRA with growing experience.
Disclosure Statement
The authors have no conflicts of interest or financial ties to disclose.