
Abstract
Objectives:
The aim of this study was to investigate the current impact of dietary counseling on the risk for urolithiasis.
Methods:
A retrospective cohort study of the patients treated in our stone clinics from July 2007 to February 2009 was carried out. Patients' urinary risk factors for stone disease were evaluated with pre- and postintervention 24-hour urine collections. All patients received dietary recommendations from a registered dietician at each visit.
Results:
One hundred thirty-seven subjects were identified and managed initially with only dietary interventions to address their urinary stone risk parameters. Average follow-up for this group was 15.19 ± 13.7 months. Subjects showed significant changes in urine volume (71.1%, 1.68 ± 0.68 to 2.59 ± 0.80 L/day, p < 0.0001), urine sodium (58.1%, 229.68 ± 72.51 to 144.65 ± 52.70 mmol/day, p < 0.0001), urine calcium (43.8%, 314.33 ± 95.75 to 216.81 ± 80.90 mg/day, p < 0.0001), urinary uric acid (50%, 0.821 ± 0.210 to 0.622 ± 0.128 g/day, p < 0.0001), urinary citrate (50.7%, 583.19 ± 330.86 to 797.36 ± 412.31, p < 0.0001), and urine oxalate (55.5%, 46.28 ± 10.31 to 32.56 ± 9.02 mg/day, p < 0.0001). The supersaturation for calcium oxalate also decreased significantly from baseline (9.34–5.03, p < 0.0001).
Conclusion:
Urolithiasis is a multifactorial disease requiring a multidisciplinary approach. Our results support the use of dietary counseling by a registered dietician in the management of urolithiasis.
Introduction
Prior studies have focused on specific dietary modifications such as fluid intake, 2 –4 sodium and protein restriction, 5 and citrate supplementation. 6 –9 Finally, for hyperoxaluric patients, diet has been shown to contribute to as much as 80% of urine oxalate. 10,11
With this background, it is clear that, in a variety of study settings, controlled dietary changes can play an important role in urinary stone parameters and subsequent risk of urinary stone formation. Our goal in this study was to translate this knowledge to a clinical setting and investigate the effect of dietary counseling without additional measures on urine stone formation parameters.
Methods
After internal review board approval (University of Minnesota Internal Review Board protocol 0408M63354), a retrospective study of consecutive patients treated from July 2007 to February 2009 at our multidisciplinary stone clinic (n = 314) was performed. Inclusion criteria for this analysis included age (≥18 years), at least two 24-hour urine collections, and recurrent stone formation. Recurrent stone formers were defined as those with a history of multiple stone passages/interventions or multiple calculi on initial presenting computerized tomography. One hundred thirty-seven patients who were managed initially with dietary intervention alone or more were included in this study.
Subjects were evaluated using two sequential 24-hour urine collections at baseline (Litholink Laboratory Reporting System; Litholink Corporation, Chicago, IL) for high urine sodium (>150 mmol/day), hyperuricosuria (men, >800 mg/day; women, >750 mg/day), hypercalciuria (urinary calcium: male, >250 mg/day; female, >200 mg/day), hyperoxaluria (urinary oxalate excretion, >40 mg/day), low urine volume (<2.0 L/day), and hypocitraturia (men, <450 mg/day; women, <550 mg/day).
The first urine collection was performed with the patient following an unrestricted diet and prior to any dietary counseling. Following this, a registered dietician provided dietary recommendations to all patients, with specific recommendations based on the 24-hour urine results. Counseling included hydration to keep urine volume above 2 L/day, sodium restriction to <2400 mg/day, protein moderation 3–4 oz twice per day, and adequate calcium intake (1000–1200 mg/day with meals), with an emphasis of timing with meals. Also, citrate-containing juice, such as lemon juice, was advised. Unless drug therapy was refused by patients, subjects with urinary oxalate >50 mg/day, urinary calcium >300 mg/day without hypernatriuria, urinary citrate <200 mg/day, or hyperuricemia >10 mg/dL underwent immediate supplemental pharmacological intervention and as such were excluded from the study, which focused on dietary intervention as a single modality therapy. Each patient received standard follow-up with a clinic-based urologist. Follow-up Litholink 24-hour urine collections were performed at 3-month intervals until urinary parameters had normalized. Patients who failed dietary counseling were supplemented with pharmacological intervention as indicated and considered a treatment failure for dietary control.
The primary endpoint for the study was the impact of dietary intervention on urinary metabolites and electrolytes levels known as risk factors for stone disease. Secondary endpoints included the proportion of patients converting from abnormal to normal levels after dietary manipulation and the changes in relative urinary supersaturation for calcium oxalate. Statistical comparisons of the postintervention urine collections to baseline were performed using a paired t-test.
Results
One hundred thirty-seven patients met the inclusion criteria. There were 70 men and 67 women for a male-to-female ratio of 1.04. Mean age was 47.2 ± 14.9 years and the average follow-up for this group was 15.19 ± 13.7 months. Additional patient characteristics can be found in Table 1. The distribution of urinary abnormalities included high urinary sodium (85.4%), uric acid (33.6%), calcium (35%), and oxalate (32.8%) and/or low urinary volume (98.5%) or citrate (51.8%).
Subjects showed significant changes in urine sodium (58.1%, 229.68 ± 72.51 to 144.65 ± 52.70 mmol/day, p < 0.0001), urine calcium (43.8%, 314.33 ± 95.75 to 216.81 ± 80.90 mg/day, p < 0.0001) (Fig. 1), urinary uric acid (50%, 0.821 ± 0.210 to 0.622 ± 0.128 g/day, p < 0.0001), and urinary citrate (52.1%, 583.19 ± 330.86 to 797.36 ± 412.31 mg/day, p < 0.0001) (Fig. 2), urine oxalate (55.6%, 46.28 ± 10.31 to 32.56 ± 9.02 mg/day, p < 0.0001) (Fig. 3), and urine volume (71.1%, 1.68 ± 0.68 to 2.59 ± 0.80 L/day, p < 0.0001) (Fig. 4). The supersaturation for calcium oxalate also showed important change from baseline (9.34–5.03, p < 0.0001) (Fig. 5). However, the majority of patients did not completely normalize their urinary parameters as demonstrated in Figure 6. Patients with persistent hyperoxaluria (44.4%), hypercalciuria (56.2%), hyperuricosuria (50%), and hypocitraturia (49.2%) were advised to receive supplemental pharmacological therapy with pyridoxine, indapamide, allopurinol, or potassium citrate, respectively.
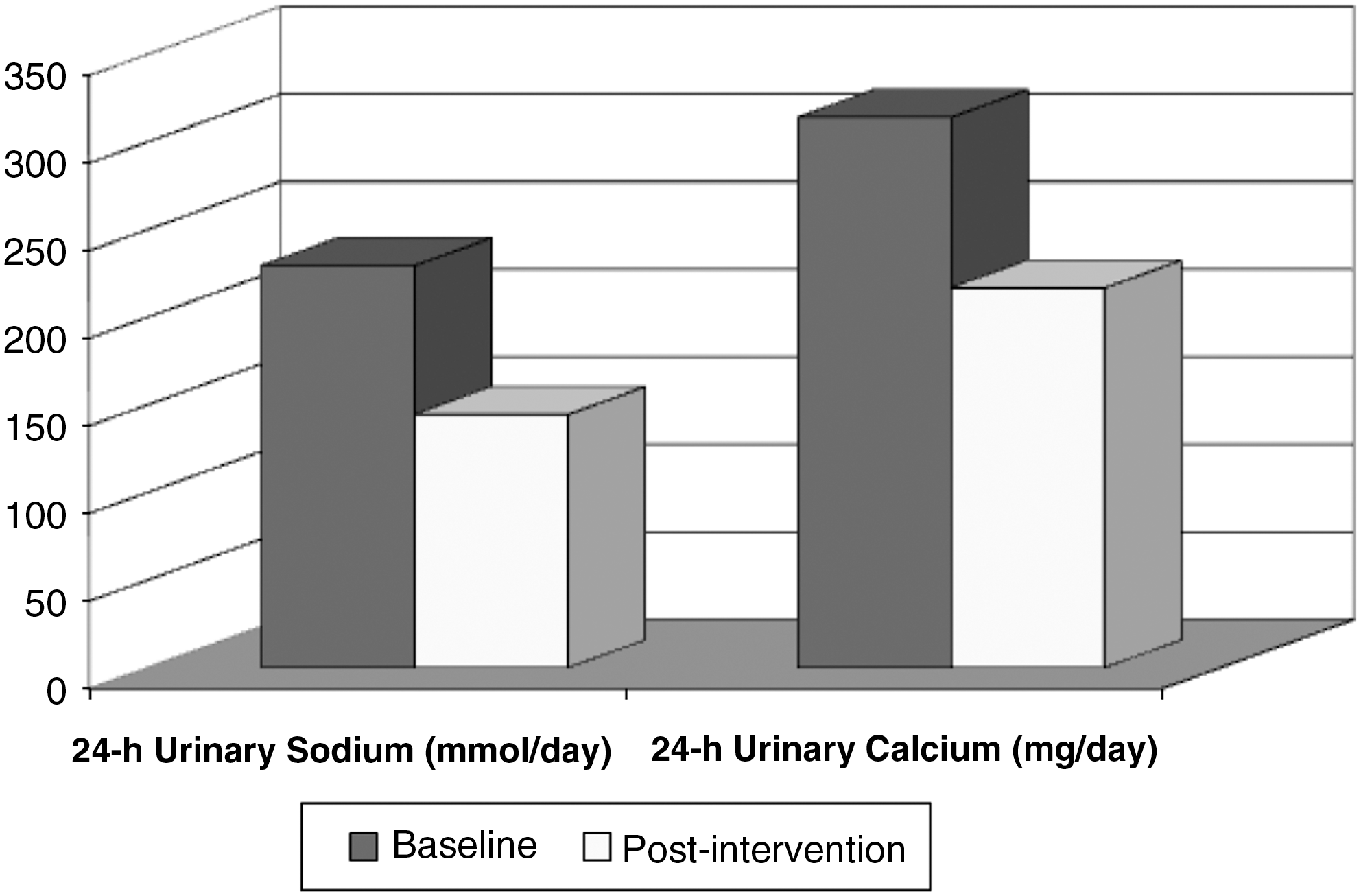
Twenty-four hour urinary sodium (mmol/day) and calcium (mg/day) excretion.
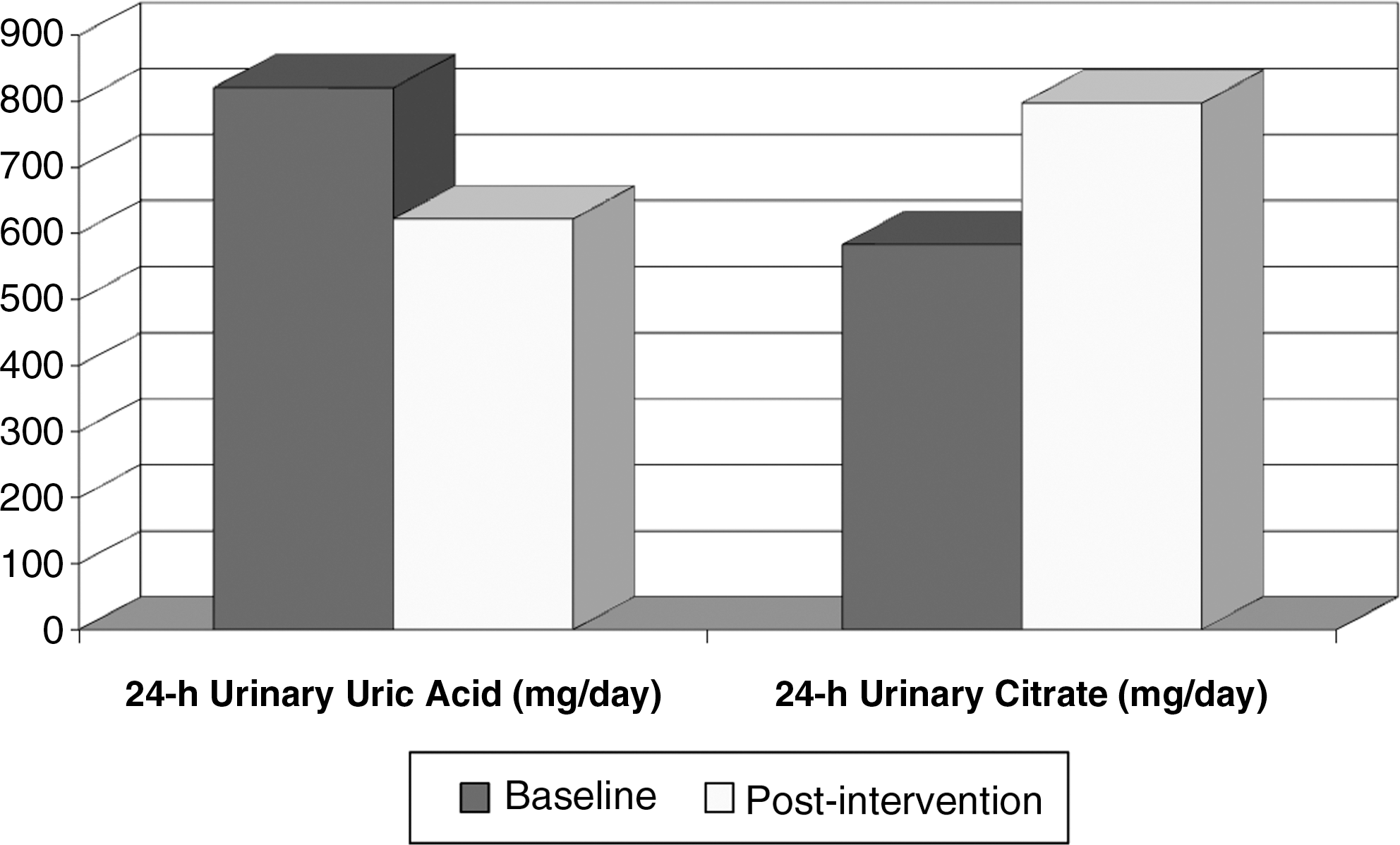
Twenty-four hour urinary uric acid (mg/day) and citrate (mg/day) excretion.
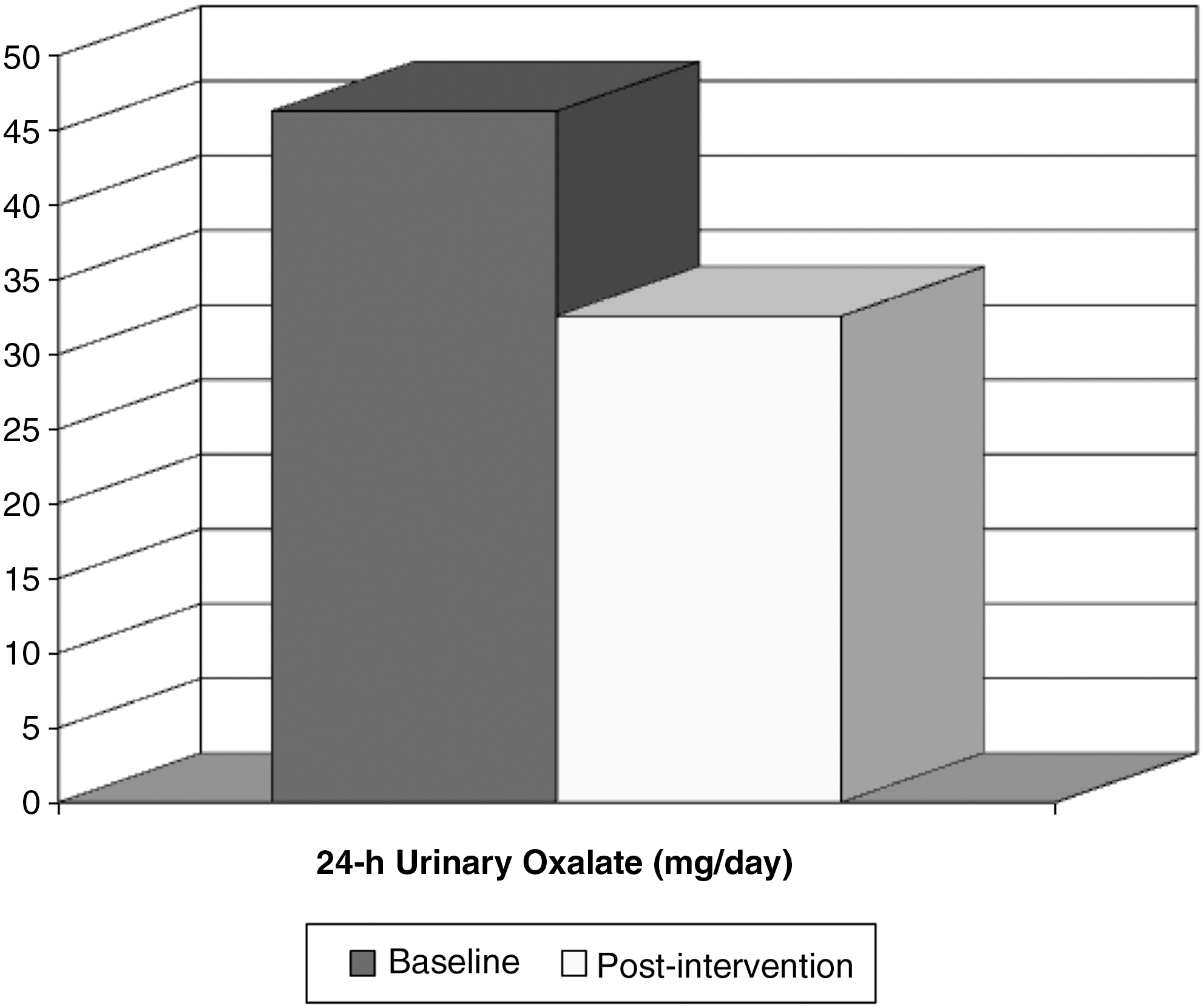
Twenty-four hour urinary oxalate (mg/day) excretion.

Twenty-four hour urine volume (L).
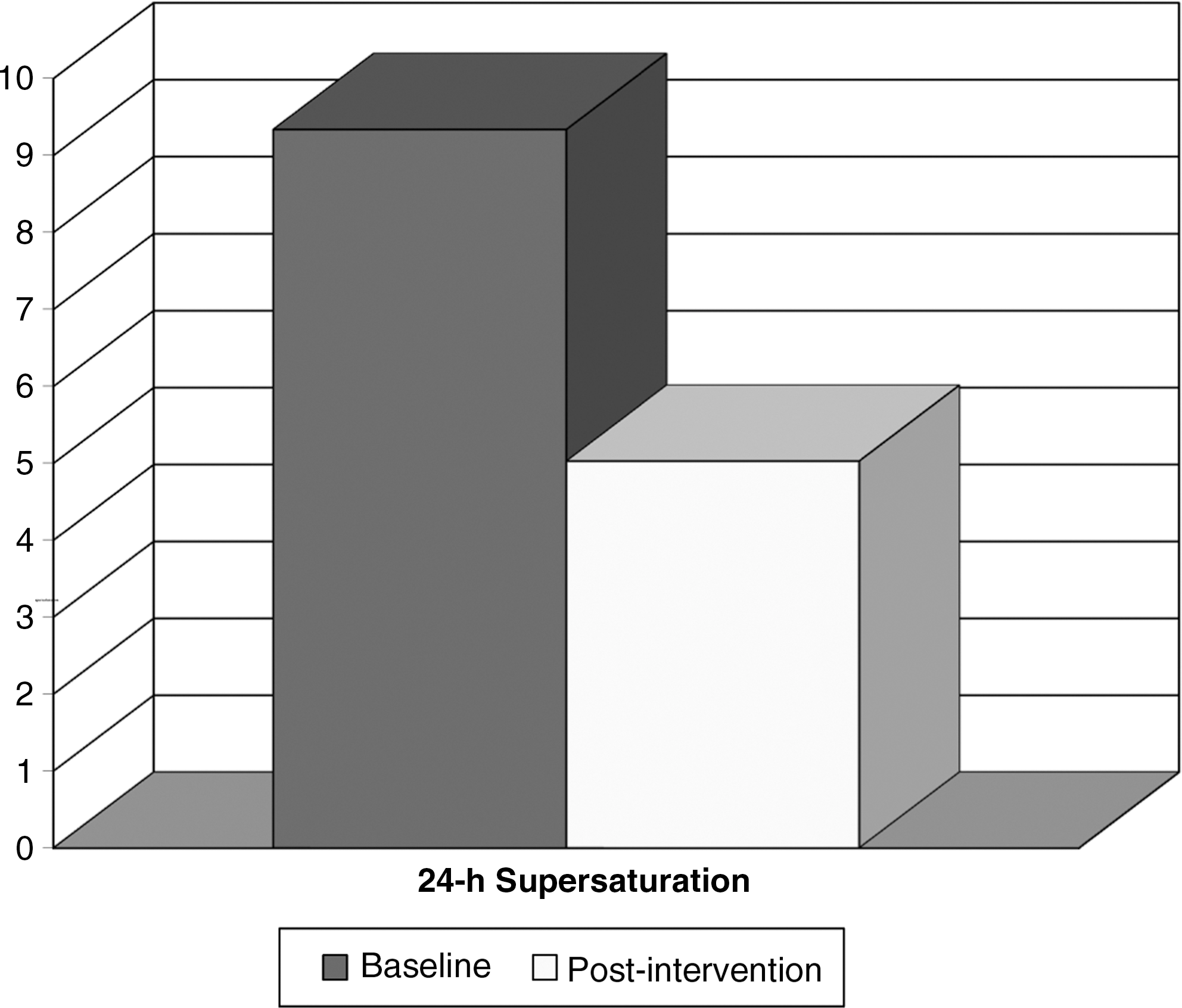
Twenty-four hour urinary calcium oxalate supersaturation.
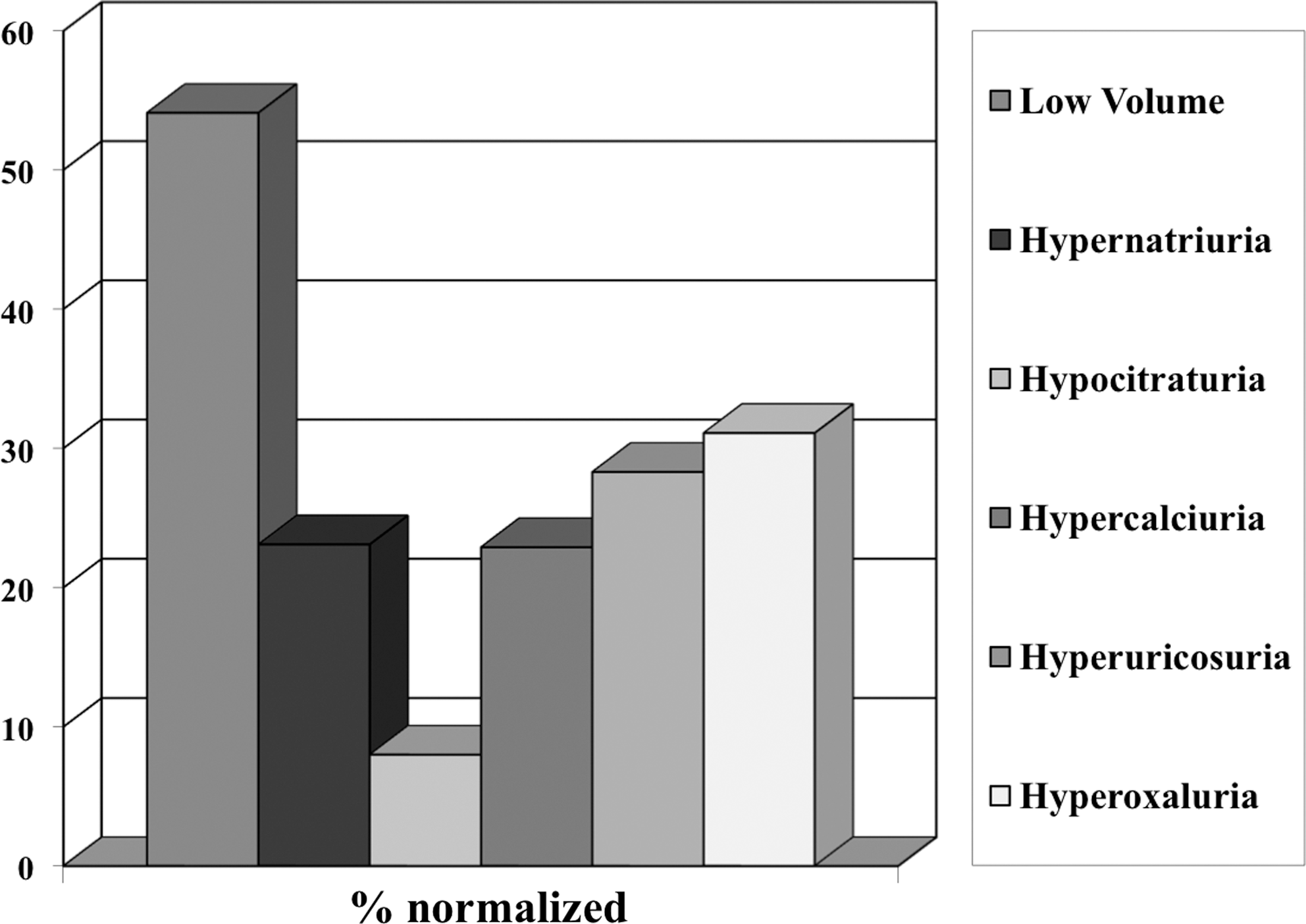
Percentage of patients with normalized urine parameters after dietary management.
Discussion
Previous studies have provided evidence of the important role of diet in the management of urolithiasis. Urolithiasis is a multietiologic disease process with diet management playing a central role in both prevention and long-term management.
Increased fluid intake has been recognized as one of the main approaches to decrease urine supersaturation. Increasing the urine volume results in a decrease in stone prevalence. 12 Borghi et al 4 followed prospectively patients with calcium stone for 5 years randomized to a high water intake protocol to achieve a urine volume of 2 L/day. During 5 years follow-up, patients in the high water intake group had fewer recurrences (12% vs. 27%, p = 0.008) and the time for recurrence was significantly longer (38.7 ± 13.2 vs. 25.1 ± 16.4 months, p = 0.016) compared with the group on regular amounts of fluid intake. 4
To determine the efficacy and safety of diet, fluids, and supplement intervention for secondary prevention of nephrolithiasis, Fink et al 13 conducted a meta-analysis on reported randomized trials and found that increased water intake to >2 L/day or enough fluid intake to keep the urine output to more 2.5 L/day decreased stone recurrence (relative risk: 0.39, 95% confidence interval: 0.19–0.80). Indeed, the inhibitory activity of Tamm-Horsfall protein over the aggregation of calcium oxalate monohydrate crystals has been found to increase with urine dilution. 14 In our patient population we observed a 71.1% response rate to increased fluid intake to keep urine volume above 2 L/day with a significant decrease in urine supersaturation of calcium oxalate from 9.34 to 5.03 (p < 0.0001).
Regarding dietary salt content, observational studies suggested a strong relation between sodium consumption and hypercalciuria, but new evidence has challenged this. High sodium intake is known to reduce renal tubular reabsorption of calcium, thereby increasing the amount of calcium excreted in the urine. 15 Also, a high-sodium diet is known to increase urine pH and has been proposed to reduce urine citrate. 16 Wasserstein et al 17 showed a positive association between urinary sodium and calcium excretion and postulated that stone formers may be more sensitive to the calciuric effect of sodium. Nouvenne et al 18 found that when idiopathic calcium stone patients were treated with sodium restriction (60 mmol/day) and high fluid intake, a reduction of 100 mmol of urinary sodium was accompanied by a reduction of 64 mg/day in urinary calcium, with 30% of patients achieving normal urine calcium. We found a 58.1% response rate to sodium restriction, with 23% of patients treated achieving normal urine sodium.
In contrast, new data specifically in patients with hypocitraturia (not hypercalciuria) demonstrated that dietary sodium supplementation resulted in increased voided volume and decreased calcium oxalate supersaturation. 19 This has to be carefully examined because these patients were followed for only a short period of time and they were already using pharmacological interventions for stone disease. Although results have been conflicting, 2,3 reduced dietary sodium is a general recommendation given to most patients with urolithiasis, and our study supports its effectiveness specifically in patients with hypercalciuria.
Uric acid solubility in the urine largely depends on the urine pH; as such, strategies to manage the urine pH should be addressed with dietary interventions if appropriate. 20 Manipulation of urine pH is a complex task because it will be affected not only by diet and hydration status but also by weight and body mass index (BMI). A negative correlation between urine pH and BMI has been found, with higher BMI associated with lower urine pH. 21,22 Including a weight reduction goal when appropriate may benefit stone patients with uric acid stones or low urine pH; however, this long-term component of dietary counseling and weight reduction was not evaluated in our study. Our specific recommendation regarding protein moderation (3–4 oz/day) led to a 50% response rate for lowered urinary uric acid.
The excretion of urine uric acid, calcium, and citrate is linked to the acid load of the diet. 23 It has been suggested that the increase of intake of fruits, vegetables, and alkali-rich low-phosphate beverages by recurrent stone formers to neutralize the acid load of food ingestion seems wise. 23,24 If urine pH is acidic, we recommend to increase the intake of potassium-containing foods (banana, dairy products, oranges, potatoes, salmon), increase citrate fruits and vegetables, and avoid acidic foods such as asparagus, cranberries, and plums. Alternatively, if the urine is alkaline, instructions can be given to increase the amount of acidic foods such as asparagus, cranberries, corn, meat, fish, poultry, vinegar, plums, and soft water. 25 –27
Citrate is an accepted inhibitor of the aggregation and growth of calcium oxalate and calcium phosphate crystals. 28 Citrate complexes with calcium ions and enhances the inhibitory activity of Tamm-Horsfall glycoprotiens toward calcium oxalate crystal aggregation. 29 In the past, dietary interventions to increase citrate have included lemonade and orange juice intake. 7,30 The results with lemonade consumption are conflicting, with one study showing an increase in urine volume but not in urine citrate. 8 Nevertheless, our results showed that 50.7% of the patients responded to dietary supplementation of citrate-containing juice for management of low urine citrate, but only 8.5% reached normal urine citrate levels with this approach.
Hyperoxaluria is a metabolic risk factor for stone disease. Dietary oxalate may contribute as much as 80% of the urine oxalate. 10,11 Krishnamurthy et al 31 demonstrated that recurrent stone formers with mild hyperoxaluria have an exaggerated response to a dietary oxalate load compared with stone formers with normal oxalate excretion. As such, a low-oxalate diet may provide benefit for patients with hyperoxaluria.
Adequate dietary calcium content to minimize intestinal oxalate absorption has been the subject of numerous studies. Borghi et al 5 in a randomized trial in men with recurrent calcium oxalate stones achieved a significant reduction in oxalate excretion and incidence for recurrent stones for patients on a normal-calcium (1200 mg/day), low-animal-protein, low-salt diet compared with a low-calcium diet (400 mg/day). Similarly, our patients received dietary recommendations to target calcium intake with meals and to keep calcium intake between 900 and 1200 mg/day. In addition, specific dietary instructions about foods high in bioavailable oxalates were given (see Appendix). We found that with this intervention, half of the patients had a decrease in urine oxalate and almost a third had normalization of urine oxalate (28.9%).
The dynamic multifactorial interplay of genetics and environment that results in urolithiasis warrants a holistic approach that includes dietary intervention, weight management, and lifestyle changes. The evaluation with a licensed dietitian is critical to identify risk factors according to sex and age and to tailor follow-up. 32 As one of the problems with conservative management of stone disease is compliance, follow-up measurements are extremely important. Further, biomarkers such as urinary potassium have been studied to follow the diet quality of patients on nutritional treatment for stones. 33 With an estimated $2.1 billion annual cost for urinary stones treatment in 2000 and with the cost-effectiveness of preventive care well established in first-time stone formers, the role for dietary therapy for stone disease is critical. 34,35
Conclusion
Dietary intervention is an integral component of prevention of kidney stones. These data support the efficacy of dietary counseling by a registered dietician and the compliance with recommendations received in a multidisciplinary stone clinic in selected patients with mild-moderate metabolic abnormalities. Our study utilized urinary stone risk parameters as a surrogate outcome measure for the efficacy of dietary intervention. Long-term studies evaluating the impact on stone recurrence rates are warranted.
Footnotes
Disclosure Statement
No competing financial interests exist.
Abbreviation Used
Appendix
Dietary Recommendations for Patients with High Urine Oxalate
Drink more than 8 cups of fluid per day
Limit salt (sodium) in your diet
Limit oxalate to 50 mg/day or as instructed by your physician
Use the information below as a guide
Fruits—green gooseberries, lemon/lime/orange peel, rhubarb
Vegetables—amaranth, beets, cassava root, Swiss chard, collards, leeks, okra, parsley, spinach
Grains/starches—wheat germ, soybean crackers
Nuts and seeds—almonds, peanuts, pecans, cashews, hazelnuts, peanut butter, sunflower seeds, poppy seeds
Miscellaneous—chocolate, dry cocoa, fig Newton, pepper (>1 tsp/day)
Fruits—blackberries, blueberries, cranberries, dewberries, strawberries, raspberries, red currants, caned fruit cocktail, concord grapes, damson plums, tangerines
Vegetables—boiled raw green, wax, dry beans, and beans in tomato sauce; celery, chicory, eggplant, escarole, kale, parsnips, green pepper, chilies, pokeweed, sweet potatoes, rutabagas, summer squash, watercress, mustard greens
Grains/starches—graham crackers, popcorn, grits, white corn, whole-wheat flour
Miscellaneous—fruitcake, vegetables/tomato soup, tomato sauce, tofu, pepper (more than 1 tsp/day)
Beverages—draft beer, juices that contain high oxalate fruit, Ovaltine, and other similar beverage mixes, tea, cocoa
Fruits—apples, oranges, pineapple, Italian prunes, black currants, cherries (red sour), apricots, peaches, pears
Vegetables—asparagus, broccoli, carrots, cucumber, iceberg lettuce, lima beans, tomatoes, turnips
Grains/starches—yellow corn, cornbread
Meats/poultry/seafood—sardines
Beverages—coffee (8 oz), grape juice, orange juice, tomato juice
Miscellaneous—sponge cake
Fruit—avocado, apples (peeled), grapefruit, mangoes, melons/cantaloupe, honeydew, watermelon, cassava, nectarines, bing cherries, bananas, grapes, peaches, plums, raisins
Vegetables—alfalfa, sprouts, acorn squash, brussel sprouts, cauliflower, cabbage, mushrooms, onions, peas, potatoes, radishes, chives, red peppers, squash
Grain/starches—corn flakes, noodles, rice, white bread, oatmeal
Meat/poultry/seafood—eggs lean lamb, beef, pork, bacon, poultry, seafood
Beverages—apple juice, grape juice, lemonade, pineapple juice, soda (12 oz/day)
Dairy—low-fat or skim milk, low-fat or fat-free yogurt, buttermilk, cheese
Miscellaneous—jelly (made with allowed fruit), lemon or limejuice, sugar, soup (with allowed ingredients), salad dressing