
Abstract
Introduction:
The purpose of this study was to compare in a randomized fashion the clinical outcomes following standard laparoscopic and laparoendoscopic single-site (LESS) donor nephrectomies.
Materials and Methods:
Fifty voluntary renal donors who met the inclusion and exclusion criteria were randomized to standard laparoscopic (group A) and LESS (group B) donor nephrectomies. The primary end point of the study was patients' postoperative pain. The clinical outcomes, patient's quality of life, body image, and cosmetic scores on follow-up were also compared.
Results:
The operating times were similar in both groups (175.83 ± 47.57 vs. 172.20 ± 38.33 minutes, p = 0.38). The surgeon's difficulty as measured using a visual analog scale was significantly more in group B in 4 of 10 defined steps. The postoperative patient pain scores were similar till 48 hours following surgery (3.84 ± 1.68 vs. 3.68 ± 0.75, p = 0.33), but following which the patients in group B had improved pain scores (2.08 ± 0.91 vs. 1.24 ± 0.72, p = 0.0004). Analgesic requirements were similar in both groups (p = 0.47). The warm ischemia times in group B (5.11 ± 1.01 vs. 7.15 ± 1.84 minutes, p < 0.0001) were longer but the total ischemia times in both groups were similar (62.55 ± 9.46 vs. 62.71 ± 12.14 minutes, p = 0.48). All grafts had on-table urine output in the recipient. Intraoperative (8% vs. 16%, p = 0.2) and postoperative complications (20% vs. 16%, p = 0.99) in both groups were comparable. The patients in group B had shorter hospital stay (4.56 ± 0.82 vs. 3.92 ± 0.76 days, p = 0.003). There was no graft loss in either group except for one recipient in group A who sustained sudden cardiac death. The estimated glomerular filtration rates of recipients at 1 year were comparable for both groups (80.87 ± 22.12 vs. 81.51 ± 29.01 mL/minute, p = 0.46). The donor's quality of life, body image, and cosmetic scores were comparable for both groups.
Conclusion:
In this select group of donors, LESS donor nephrectomy, although challenging to the surgeon with longer warm ischemic times, gave early pain relief with shorter hospital stay and comparable graft function.
Introduction
Materials and Methods
This randomized comparative study was approved by our institutional review board. The study period was from January 2009 to February 2010. A total of 50 patients were recruited and randomized equally into groups A and B (Fig. 1). The patient demography in both groups is shown in Table 1. The primary outcome of the study was postoperative patient pain score documented using a visual analog scale (VAS). The secondary end points were clinical parameters including operating times, requirement of analgesics, hospital stay, quality of life scores, body image scores, cosmesis scores, and recipient graft function. Twenty-five donors had to be included in each arm to establish a significant mean pain score difference of 1 with a standard deviation of 1.5, a power of 0.9, and an α of 0.05. The sample size was calculated using Power and Sample size calculation version 3.0. After prior informed consent, 50 voluntary related renal donors who have been completely worked up and cleared for laparoscopic donor nephrectomy were randomized by chit method with block randomization. 10
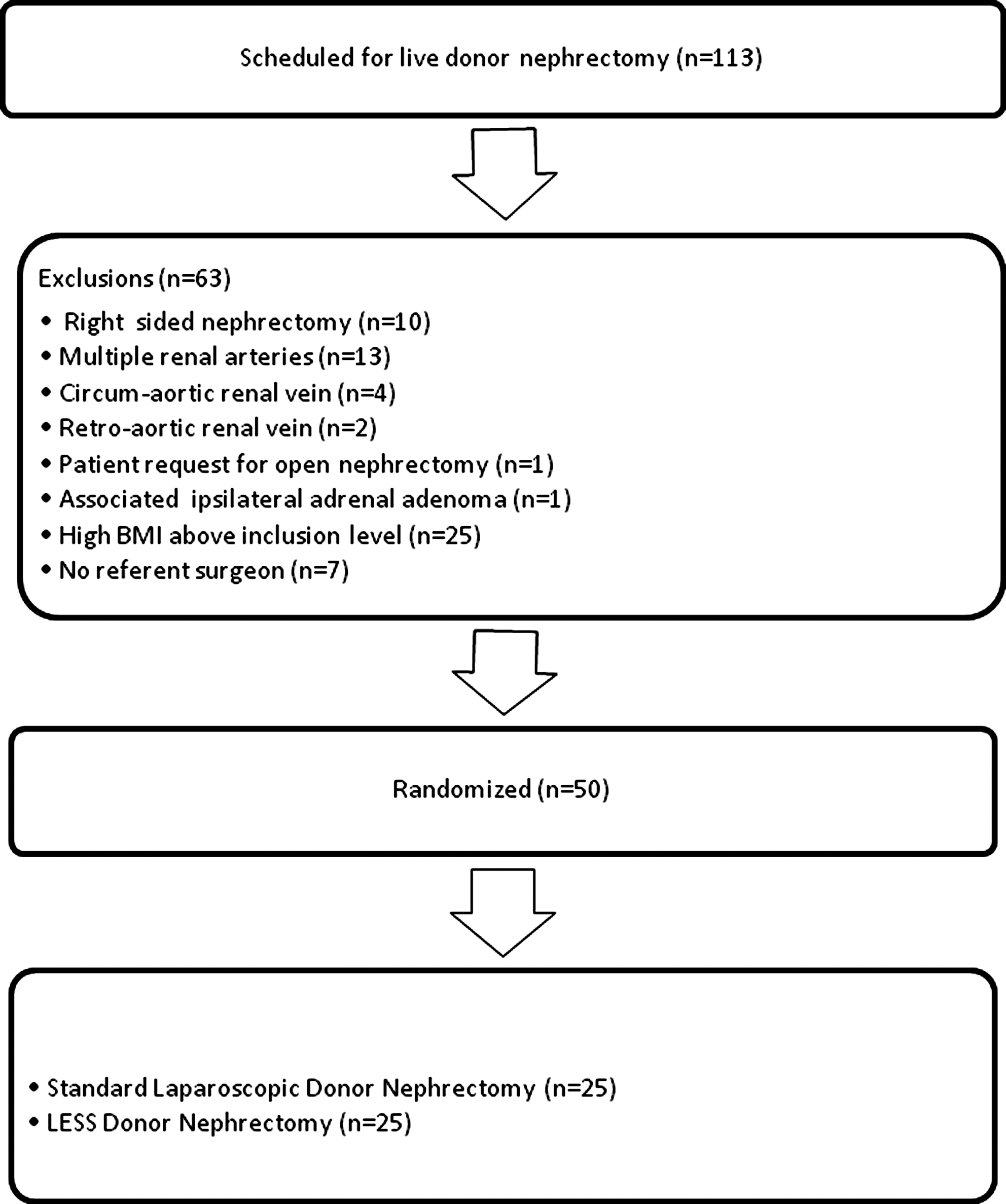
Flowchart showing patients recruitment. BMI = body mass index; LESS = laparoendoscopic single-site.
SF 36v2 Health Survey, taken 1 month prior to nephrectomy.
BMI = body mass index; LESS = laparoendoscopic single-site.
The exclusion criteria for the study were right-side nephrectomy and any abnormal renal vascular anomaly. Patients with a body mass index of >25 kg/m2 were also excluded from the study in the first 30 patients. The cutoff body mass index was later extended to 27 kg/m2 for the later 20 patients.
The LESS donor nephrectomies were performed by the same surgeon (M.D.). The standard laparoscopic donor nephrectomies were performed by multiple surgeons, all under the supervision of M.D. The operating room team was same in both groups. In group A, access was achieved through three to four standard ports placed after creating pneumoperitoneum. The access was achieved using an R-port (TriPort or QuadPort) (Advanced Surgical Concepts) placed through an umbilical incision in group B. After incising the skin in a zigzag fashion, the sheath and peritoneum were incised vertically in the midline and the R-port was inserted. A standard 10-mm telescope was used in group A, whereas a 5-mm, 30-degree telescope with coaxial light cable was used (EndoEye) in group B. A 5-mm telescope with a flexible, actively deflectable tip was used in two cases in group B intermittently (EndoEye). An accessory 3-mm port was inserted if required by the surgeon to introduce a 3-mm forceps to help in retraction. Following port insertion, the surgical steps were same in both groups and consisted of colonic reflection, mobilization of the ureter–gonadal packet, adrenal vein division, upper pole separation, lumbar vein division, dissection of the renal pedicle, division of gonadal vein and ureter, division of the renal artery and vein, and graft retrieval. The difficulty level of each step was recorded by the surgical team in a VAS (1 to 10).
Before dividing the vessels, the ureter and gonadal vein are divided. Mannitol is given intravenously and a brisk urine output is observed from the divided ureter before proceeding to divide the vessels. After dividing the renal vessels, the freed graft was retrieved by hand, inserted through a preplaced pfannenstiel incision after incising the peritoneum. In group B, the graft was retrieved through the umbilical incision after removing the R-port. The rectus sheath and peritoneum may be further incised to facilitate easy retrieval. The supple skin is stretched to accommodate the outcoming kidney, but sometimes may require minimal extension of the incision. The entire hand need not be inserted and the kidney in its long axis can be maneuvered out gently with fingers. In the last three cases, we modified the retrieval by placing the graft in a retrieval bag (ENDO CATCH II 15-mm Specimen pouch, Covidien/Autosuture; Hamilton HM FX). The surgical wound was not infiltrated with local anesthetic. Patient demography and operative details were recorded for both groups. The operating time, blood loss, intraoperative complications, and conversions were noted. In the postoperative ward, patients received analgesics (tramadol) on demand. Pain scores were recorded using a VAS (1 to 10). Pain scores were documented at 12, 24, 36, 48, 60, 72, and 96 hours following surgery. The VAS pain score was recorded by the postoperative transplant recovery room nursing staff. Postoperative complications were recorded and classified according to the Clavien and Dindo system. 11,12 Patients were usually discharged once they were on normal diet and are ambulant and comfortable. The estimated glomerular filtration rate calculated using the four-variable Modification of Diet in Renal Disease equation was recorded for the recipients on follow-up. 13,14 The quality of life was assessed in both the groups by the SF 36v2 Health survey preoperatively and postoperatively at 6 and 9 months. All patients were contacted at once and asked to fill out the Body Image questionnaire evaluating body image and cosmesis. 15 The questionnaire consists of five questions that measure patients' perceptions and satisfaction with their own body and their attitude toward their bodily appearance (body image) (score 5–20) and three questions that assess satisfaction with the appearance of scar (cosmesis) (score 3–24). Higher scores on both scales indicate greater satisfaction. The SF 36v2 Health survey and body image questionnaire were filled up by our trained transplant social worker who was blinded to the mode of nephrectomy.
Statistical analysis was carried out using SPSS version 15.0. We used the chi-square test and Student's t-test to compare categorical and continuous variables, respectively.
Results
The difficulty level for the surgical team was similar on all steps in both groups except in port insertion, upper pole separation, division of renal vessels, and graft retrieval, with significantly higher scores in group B (Table 2). The clinical outcomes in the donor and recipient are outlined in Table 3. All patients in group B required insertion of an accessory 3-mm port for inserting an instrument for retraction. The accessory port was inserted during the step of adrenal vein division, upper pole separation, and renal pedicle dissection in 40%, 52%, and 8% of the cases. None of the patients required open conversion. Two patients (8%) in group B required more than one accessory port and thus were labeled as conversion to multiple ports donor nephrectomy.
LDN = laparoscopic donor nephrectomy; eGFR = estimated glomerular filtration rate.
Patients in both groups had similar pain scores in the immediate postoperative period. Significant improvement in pain scores were documented in group B after 48 hours following surgery (Table 4). The quality of life scores, body image scores, and cosmesis scores were comparable in both groups. The incidence of intra and postoperative complications was comparable in both groups. The intraoperative complications in either group did not require open conversion and were managed immediately without any postoperative sequel. In the postoperative period, the rate of complications recorded was comparable in both groups and there were no grade 3, 4, or 5 complications. One recipient in group B had a sudden cardiac death in the follow-up period, resulting in graft loss. There was no other graft loss in either group. Good graft functions were documented in both groups.
In group A (standard laparoscopic donor nephrectomy), two patients had fever, which necessitated antipyretics. Two patients had minimal purulent discharge from the surgical incision, which necessitated regular wound dressings but not removal of stitch or antibiotics. One patient was readmitted with subacute intestinal obstruction, which was managed conservatively and did not necessitate any surgical intervention. In group B (LESS donor nephrectomy), two patients had fever, necessitating antipyretics, and two patients had minimal purulent discharge from the umbilical wound, which necessitated only regular wound dressings but not antibiotics, stitch removal, or any untoward cosmetic sequel.
Discussion
The donor is not a patient with an existing pathology that needs laparoscopic removal or correction. The intent of the donor is to save the recipient's life. A donor would prefer minimally invasive donor nephrectomy because of the shorter convalescence and decreased pain. 16 Minimally invasive surgical techniques would enhance the willingness of family and friends to donate. Live donor nephrectomy rates have significantly increased with the advent of laparoscopic donor nephrectomy. 17 It is understandable that a significant population may come forward to donate if the morbidity associated with living donor nephrectomy is further reduced. Considering that the donors in our population is young and mainly women, cosmesis will also be in their minds. LESS donor nephrectomy with lesser pain, faster recovery, promises of better cosmesis, and equivalent graft outcomes will bring forward more donors. In donor nephrectomy, the safety of the donor and retrieving the graft in perfect condition are of paramount importance. Care should be taken while introducing any new technique to make sure that the comfort zone of the surgeon and patient safety are optimal. Keeping this in mind, many patients were excluded as per the exclusion criteria, from randomization. So we do admit that the patient population in this study was highly selected.
The primary objective of this study was to compare the patient pain scores in each group. The pain scores were assessed for 96 hours following surgery. The rapidly declining pain scores in patients undergoing LESS donor nephrectomy through a nonmuscle cutting umbilical incision in the study probably suggest that the speed of pain relief is directly proportional to the length of incision. So it may appear that decreasing the length of skin incision decreases the postoperative pain. It is known in the scenario of tumor nephrectomy that reducing the extraction site incision by morcellation of the specimen results in reduced pain to the patient. 18,19
LESS nephrectomy is technically more challenging. Lack of triangulation and clashing of instruments both inside and outside the peritoneal cavity are the common problems. The skills are developed with practice in the dry lab and in animal models. Use of long and bent instruments along with standard instruments can reduce clashing. R-port comes in two varieties. The QuadPort with four ports, a larger working window, wider ports (15-mm instruments can be passed with ease), and wider distance between ports was used in 20 cases. The TriPort was used in five cases. Flexible tip laparoscopes can be valuable in observing the posterior aspect of the renal pedicle. Clashing of instruments gets worse during upper pole dissection in left donor nephrectomy. This can be solved by swapping the port sites of the working and retraction instruments. Graft extraction is more challenging when compared with the standard laparoscopic donor nephrectomy. In the last three cases, graft extraction was done using a specimen retrieval bag. The freed graft should be aligned in its longitudinal axis so that it comes out with ease through the smaller opening. The zigzag incision also helps in adequate skin retraction during graft extraction while keeping the scar confined to the area of umbilicus.
Warm ischemia time in our study was defined as the time taken from clipping of the renal artery to clear efflux seen following cold perfusion of the retrieved graft. The warm ischemia times were clearly longer in the LESS group and are of great concern. The graft retrieval technique evolved during the period of the study. Initially, the graft was retrieved in the long axis of the kidney by three to four fingers inserted through the wound. The sheath incision was extended without usually extending the skin incision to accommodate the breadth of the kidney including the perinephric fat. This technique has been now refined by placing the graft in a retrieval bag and retrieving it in the long axis. In comparison, the graft retrieval in the standard group has been standardized and perfected over the years by a simple act of inserting the hand through a preplaced pfannenstiel incision and removing the graft. In the last three patients in whom we modified our technique with the help of a retrieval bag, the mean warm ischemia time was 5.5 ± 2.17 minutes. So we are hopeful that the warm ischemia times will be comparable with more experience in the near future. Even though the warm ischemia times are significantly different, we were not able to document a difference in estimated glomerular filtration rates, acute rejection episodes, acute tubular necrosis, ureteral complications, or graft loss between the groups on follow-up of the recipients up to 1 year (Table 3).
In the donors' opinion, in our study, there were no difference in the quality of life, body image, and cosmesis following either standard or LESS donor nephrectomy. A larger sample size is probably required for a more definitive conclusion for this secondary outcome. Nevertheless, it suggests that an altruistic donor is probably not concerned about cosmesis. The quality of life scores can be also partly influenced by graft outcomes because of their great concern for the welfare of the recipients. In a study by Kok et al 5 comparing mini-incision open (n = 50) and laparoscopic (n = 50) donor nephrectomies, the quality of life scores were significantly better in the laparoscopic group. In a retrospective study by Lind et al, 20 the body image and cosmesis scores were comparable in both laparoscopic and open donor nephrectomy groups. Although we agree that the donor is more concerned about the recipient's wellbeing, more donors will come forward once we assure a less-disfiguring and less-painful surgery.
It is evident from this study that LESS donor nephrectomy is technically more demanding even for an expert in various steps of the surgery and is not without complications. It should be attempted only by surgeons with adequate experience in standard laparoscopic surgery and other LESS urological procedures.
Conclusion
In this study on select group of donors, we have found that even though LESS donor nephrectomy is technically more demanding for the surgical team with longer warm ischemic times, the patients had early relief of pain with shorter hospital stay with similar complication rates and equivalent graft outcome when compared with standard laparoscopic donor nephrectomy.
Footnotes
Acknowledgment
The authors thank Mr. Shashikant Chinchole for helping with the statistical analysis.
Disclosure Statement
No competing financial interests exist.