
Abstract
Background and Purpose:
Safe intraluminal access to the ureter and kidney is essential for endourologic procedures. Pharmacologic manipulation of ureteral smooth muscle could conceivably ease access and decrease morbidity. To minimize systemic effects, local intraluminal administration would be optimal, but the urothelium presents a barrier to the passage of medications. We present a novel ex-vivo apparatus and technique to measure ureteral peristalsis and assess drug diffusion.
Materials and Methods:
Excised 3-cm pieces of porcine or human ureters were placed inside a specially designed apparatus that allows separate manipulation of the intra- and extraluminal environments while measuring peristalsis. Intraluminal antegrade perfusion was maintained by a reservoir. A pressure transducer was placed at the inflow end of each ureter segment. After equilibration, phenylephrine (10 μM) was then added extraluminally to induce peristalsis. Nifedipine was then added to the intraluminal reservoir or the external organ bath. The concentration of nifedipine needed to cause aperistalsis was measured.
Results:
In 12 trials, extraluminal nifedipine caused aperistalsis at a concentration of 1 ± 0.1 μM, while intraluminal nifedipine needed 10.2 ± 1.1 μM. Significantly higher concentrations of nifedipine were needed intraluminally to cause aperistalsis, (P < 0.0001).
Conclusions:
With our apparatus, we can control the intraluminal and extraluminal ureteral environments, and measure peristalsis before and after drug administration. This apparatus should help investigators who are interested in studying both the diffusion of a wide range of drugs, as well as the effects of those medications on ureteral physiology. In this study, the urothelium acted as a significant barrier to the diffusion of nifedipine.
Introduction
Accordingly, any pharmacologic manipulation of the ureter to relax it before surgery might prove beneficial by easing insertion of instruments, reducing surgical complications, and decreasing operative times.
At present, there is no medication approved by the Food and Drug Administration that is designed for ureteral relaxation and medical stone expulsion therapy. Clinically, tamsulosin and nifedipine both have been shown to improve stone expulsion rates by presumably relaxing the ureter. 1 Using medications to relax the ureteral smooth muscle before endourologic surgery could be of great future clinical importance, because it could allow the passage of larger instruments and sheaths, thereby facilitating the management of larger stones with ureteroscopy, and thus reducing the indications for the more morbid approach of percutaneous nephrolithotripsy.
Because all medications that are currently used to relax the ureter are also used as blood pressure medications and have unwanted systemic side effects, local intraluminal application of these medications would be ideal. The urothelial barrier, however, inhibits passage of medications from the lumen to the ureteral smooth muscle. In this regard, more scientific pharmacologic data are needed.
Currently, there is no ex-vivo method for the quantification of drug diffusion across the urothelium. To do this, precise control of both the intraluminal and extraluminal drug concentration is needed, in conjunction with the ability to measure ureteral contractile activity after drug administration. The effect of medications has been previously studied in an in vivo animal model, both via intravenous 2,3 and intraluminal 4 administration. Several groups have developed ways to measure the contraction of isolated rings 5 or strips of ureter, 6 –8 but to date, nobody has been using ≥2 cm lengths of intact ureter with isolation of the intraluminal surface from the extraluminal area of the ureter. We present a novel ex-vivo apparatus and technique to measure ureteral peristalsis and assess drug diffusion.
Materials and Methods
Complete intact porcine ureters and an intact segment of human ureter were obtained fresh from pigs and from discarded clinical material. All work was performed under Institutional Review Board (IRB) and Institutional Animal Care and Use Committee approved protocols. The ureters were cleaned of periureteral connective tissue and cut into 3 cm long segments perpendicular to the lumen. They were then placed in gassed Krebs bicarbonate solution at 37°C, pH 7.4. The Krebs solution is gassed with 95% O2 and 5% CO2, and contains (in mmol/L): 118 NaCl, 4.7 KCl, 1.64 MgSO4, 1.18 KH2PO4, 2.52 CaCl2, 24.9 NaHCO3, and 5.5 D-Glucose.
Porcine ureteral pieces likely function best when used immediately after harvesting. We have noticed in additional trials (not reported here) that the ureter will still function after up to 24 hours of refrigeration; however, we have no data that compare contractile amplitude or frequency and would be concerned that the data would be inaccurate if the ureters are not used immediately. We attempted to obtain ureters from a local slaughterhouse. These ureters, which were approximately 3 days old, did not function at all, even though they had been refrigerated since the time of collection. All trials in these reported experiments were performed using freshly harvested ureters and were done within 1 hour of collecting, cleaning, and preparing the ureteral segment, on average within 30 minutes. Peristalsis will continue for up to 10 to 12 hours after introduction into the ureteral apparatus. After aperistalsis occurs, it takes approximately 1 hour for the nifedipine to wash out and peristalsis to restart.
Next, the prepared ureteral segments were placed horizontally in separate chambers of a double-walled polysterol organ bath with 50 mL of gassed Krebs bicarbonate solution. Each segment was cannulated by inserting polysterol tubing (internal and external tubing diameter of 2 and 3 mm, respectively) into the open luminal ends and securing the ureter ends with 4-0 silk suture. The ureter was cannulated so that the proximal end was the fluid inflow and the distal end was the outflow. A pressure transducer (TRN050, Kent Scientific, Torrington, CT) was calibrated with water pressure, ranging from 10 to 100 cm, and then placed in-series at the inflow end of each ureteral segment. Intraluminal antegrade perfusion was then maintained by a constant pressure, gravity fed reservoir containing Krebs solution (height 50 cm, volume 50 mL). The used solution drained by gravity to a waste receptacle. The pressure transducer produced a DC voltage output signal that was sampled at 100 Hz and processed using a Transbridge Amplifier (World Precision Instruments, Sarasota, FL), a PowerLab digitizer and LabChart software (both from ADInstruments, Inc, Colorado Springs, CO). Unpaired t tests with Welch correction were used to compare the data. Statistics and graphing were performed using GraphPad Prism (GraphPad Software, Inc, La Jolla, CA).
In the absence of peristalsis, Krebs solution flowed through the ureter at a pressure of approximately 4 mm Hg with a flow rate of 1 to 4 mL/min. During peristalsis, flow was blocked and the pressure increased. A slotted optical switch flow transducer with a drop counter phototransistor (Optek Technology, Carrollton, TX), was used to control the flow. The complete apparatus is seen in Figure 1. It can be used to test up to four segments of ureter simultaneously.
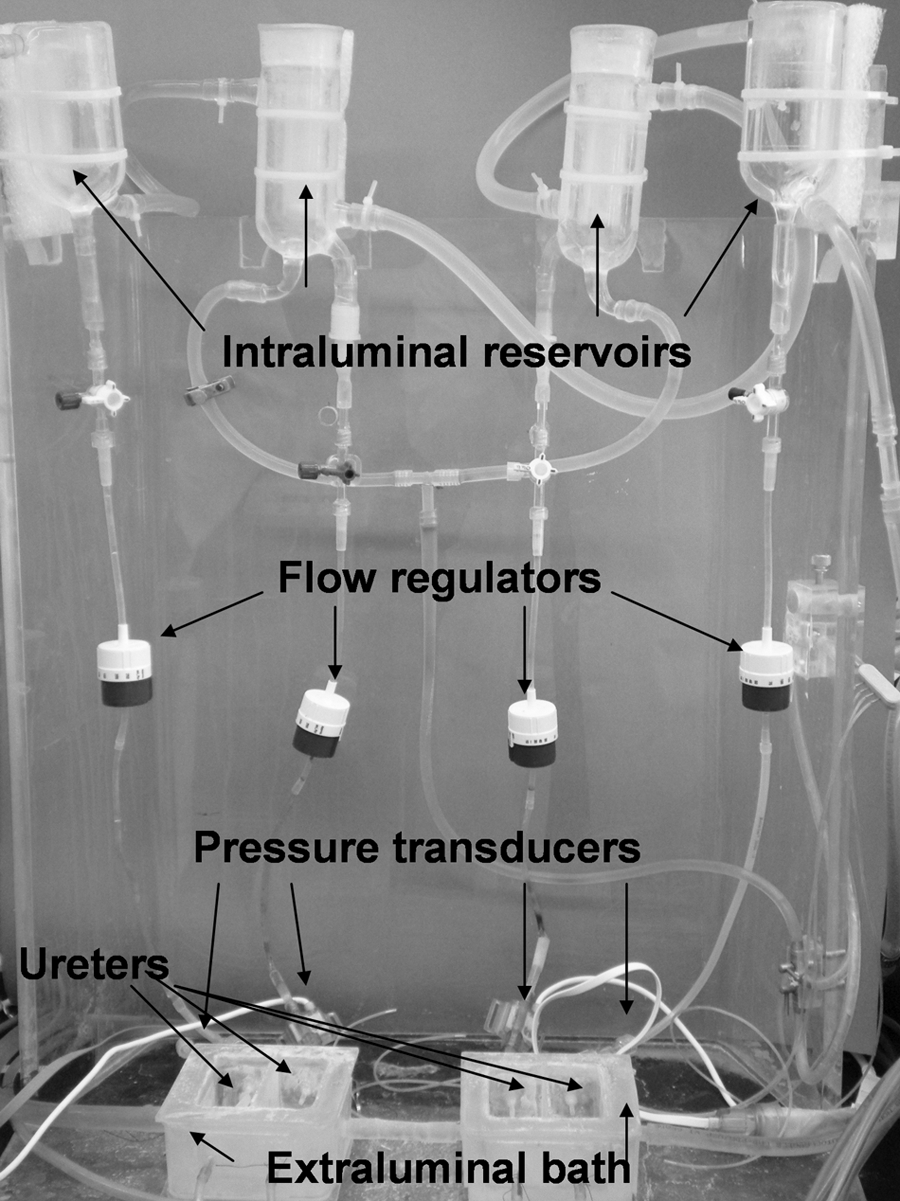
The novel ex-vivo ureteral apparatus developed in our laboratory that can test four ureteral segments at one time.
Prior to administration of pharmacologic agents, the ureter was maintained for 1 hour in the organ bath at a constant intraluminal flow (1 mL/min) of Krebs solution. This served to equilibrate the ureter after the shock and trauma of surgical removal and periureteral connective tissue cleaning. In addition, the flow of Krebs acted to relax the ureter, increasing the baseline intraluminal diameter from 1 mm to 3 to 8 mm, and occasionally evoked spontaneous peristalsis. Extraluminal administration of medication was performed by adding substances directly to the organ bath. For intraluminal drug administration, the medication was added to the elevated reservoir. The flow transducer (Fig. 1), which regulated intraluminal flow, could be bypassed if desired, to allow a rapid delivery of medication.
To quickly and reliably induce and enhance peristalsis, phenylephrine (Sigma-Aldrich St. Louis, MO) at a concentration of 10 μM was added to the external bath and intraluminal reservoir of all preparations. Phenylephrine is given therapeutically at many different doses; this dose was chosen because it has been shown to cause changes in Ca2+ concentrations and thus changes in tone in isolated canine pulmonary artery smooth muscle cells. 9 The effect of phenylephrine was rapid and durable, developing within 1 minute and lasting more than 1 hour. Test agents to induce relaxation or aperistalsis were added to either the extraluminal or intraluminal environments.
Two experiments were performed to evaluate the ureteral apparatus. In the first, to test the effects of intraluminal vs extraluminal nifedipine administration, twelve 3 cm porcine ureteral segments were obtained and cleaned, cannulated, and introduced into the ureteral apparatus. To induce peristalsis, 10 μM phenylephrine was added. In six trials, nifedipine (Sigma-Aldrich St. Louis, MO) was administered to the extraluminal bath, and in another six trials, it was added intraluminally to the reservoir. In both trials, the drug was administered in escalating doses until aperistalsis was seen. These doses were 0.1 μM, 0.25 μM, 0.5 μM, 0.8 μM, 1.0 μM, 1.2 μM, 1.4 μM, 2.5 μM, 5.0 μM, 7 μM, 8 μM, 9 μM, 10 μM, 11 μM, 12 μM, 15 μM, and 25 μM. The initial dose was chosen based on the effective human concentration of nifedipine, which is 47 ng/mL or 0.135 μM. 10 To reach the next dose, the difference in concentration of pure nifedipine was added to the bath or reservoir.
Each dose was allowed 30 minutes to have an effect before the next higher dose was given. The minimal concentration of antagonist needed to block the effect of phenylephrine was measured.
In the second experiment, we attempted to see if human ureter behaved similarly to porcine ureter. A single 3 cm segment of human ureter was obtained from a nephrectomy specimen and cleaned, cannulated, and introduced into the ureteral apparatus. Flow was started, and spontaneous ureteral peristalsis without any pharmacologic intervention was assessed. Pressure and flow tracings were recorded.
Results
Our primary end point measure was the concentration needed to stop peristalsis. For the 12 porcine ureteral segments, the amount of nifedipine needed to cause aperistalsis was 0.8, 0.8, 1.0, 1.0, 1.2, and 1.4 μM extraluminally, and 7, 8, 10, 10, 11, and 15 μM intraluminally. A sample tracing, using extraluminal nifedipine to stop peristalsis, is seen in Figure 2. In 12 trials, extraluminal nifedipine caused aperistalsis at a concentration of 1 ± 0.1 μM, while intraluminal nifedipine required 10.2 ± 1.1 μM (P < 0.0001) (Fig. 3).
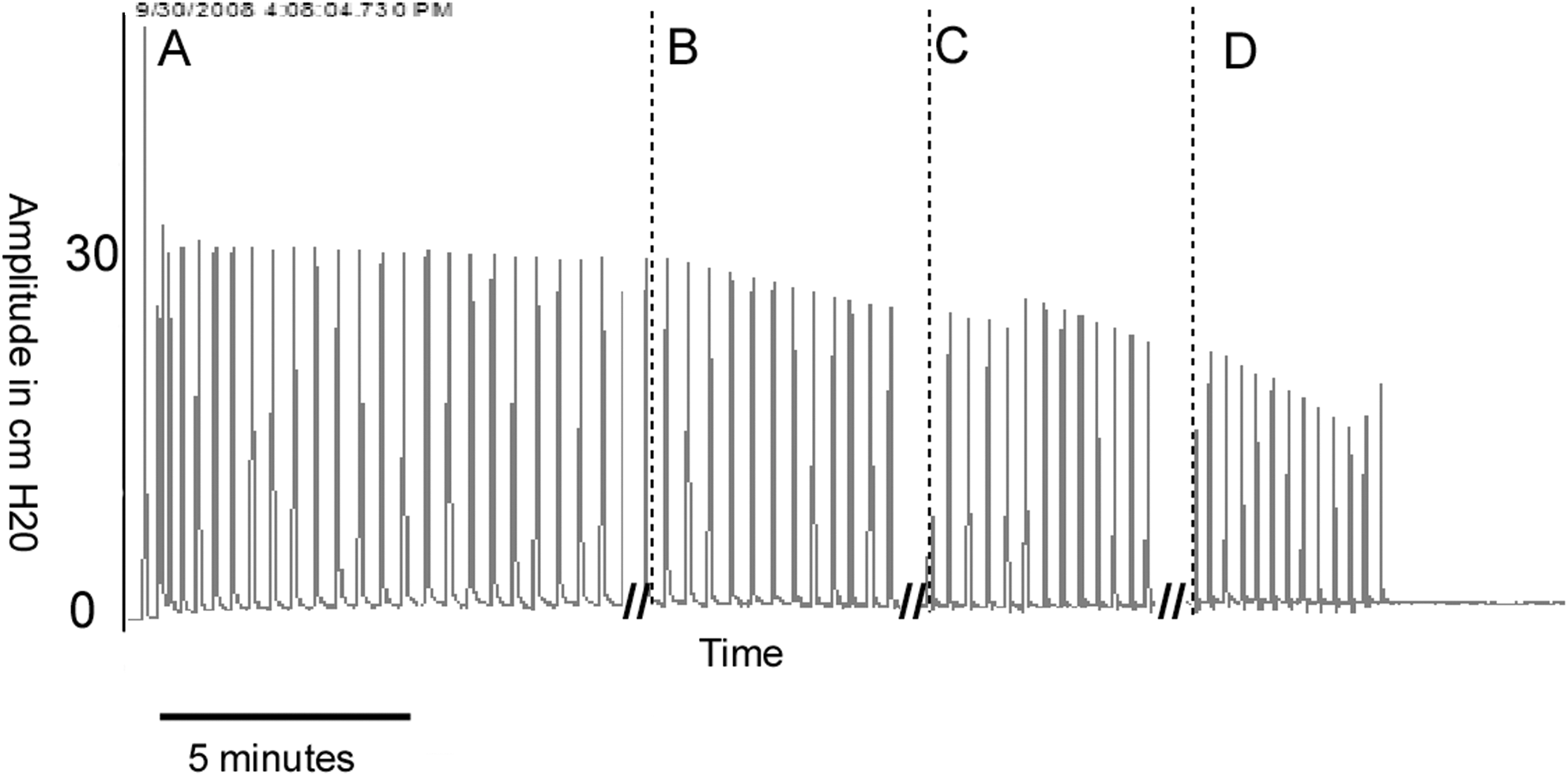
Sample tracing that shows
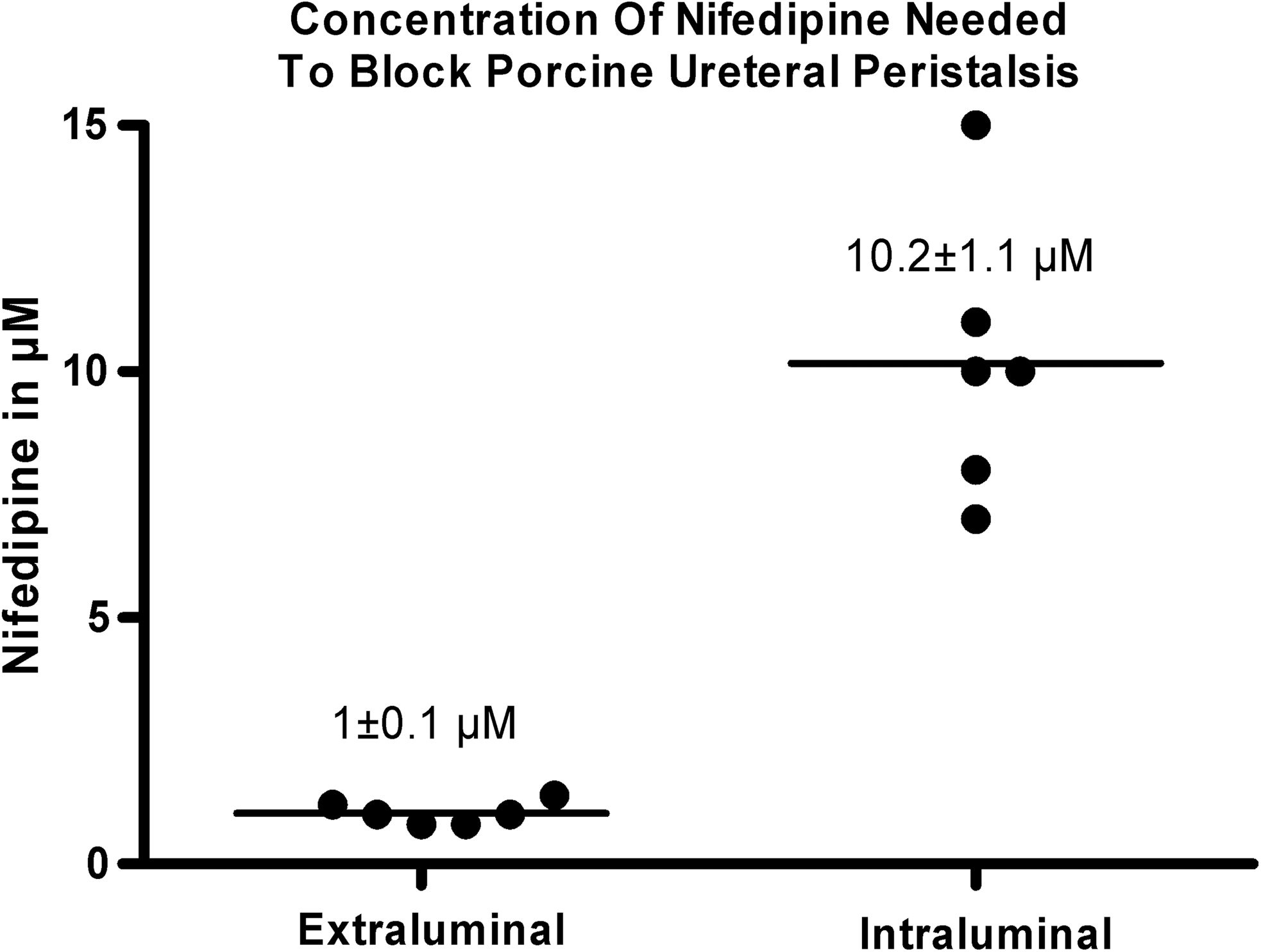
Comparison of extraluminal vs intraluminal nifedipine concentration needed to block porcine ureteral peristalsis.
In the single human ureter trial, we showed that the ureteral apparatus will measure peristalsis in the human ureter and that the human ureter will exhibit spontaneous peristalsis. Peristalsis was measured by increases in pressure as determined by the pressure transducer and reductions in flow as calculated by the flow transducer (Fig. 4). The frequency of spontaneous peristalsis in this trial was approximately 0.011 to 0.0167 Hz (one contraction every 60–90 s), and the pressure of the contraction was greater than 30 cm H2O.

Pressure
Discussion
Except for actively transported substances, the urothelium is essentially impermeable to all substances present in the urine and blood. 11 The luminal surface of the urothelium is covered by glycosaminoglycans (GAGs) adhering to proteins. The role of GAGs in the upper tract is not completely known, but they are likely involved in reducing the formation of renal calculi. 12 In the bladder, GAGs on the luminal epithelial surface are thought to be important in maintaining bladder impermeability. 13 Therefore, movement across the urothelium must pass this GAG layer first and then occur via either a transcellular (across the urothelial cell membrane) or a paracellular (through the spaces between cells and across the tight junctions) pathway. 11
Because of this impermeability, ex-vivo studies need to separately control the intraluminal and extraluminal environments if data are to be used to predict in vivo studies. Most in vivo ureteral pharmacologic studies administer the test drug via an intravenous route, which can experimentally make it difficult to separate the local from the systemic effect. It is, of course, possible to add medications directly into the lumen of the ureter in an in-vivo animal model, 4 but this can be difficult and time consuming. Also, it is often difficult to obtain IRB approval to test oral medications in a human model. 14 Our ex vivo method allows for the rapid testing of myriad drugs in either human or porcine tissue that would otherwise be discarded.
Pharmacologic manipulation of the ureter has proven difficult to measure in an ex-vivo model. Several groups have developed ways to measure the contraction of isolated rings 5 or strips of ureter. 6 –8 In most studies, the ring or strip is placed directly into an organ bath, where it is attached to a force transducer. While this method is effective for understanding the ureteral smooth muscle's response to medication, it cannot measure the urothelial barrier because the intraluminal and extraluminal surfaces are equally bathed. More importantly, a ureteral ring or strip cannot allow us to study ways to overcome the urothelial barrier. Furthermore, a ring or strip of ureter is not truly representative of the intact ureter in segment form over which a peristaltic wave can properly propagate as it would in vivo.
Tsuchiya and Takei 15 evaluated the response of the ureter to electrical stimulation by measuring intraluminal pressure changes in a standing column of fluid. In their apparatus, a 3 to 5 cm segment of ureter was cannulated and attached to a pressure transducer, then submerged in an organ bath. After stimulation with an electrical impulse, they could measure the force of peristalsis using the pressure transducer. Our method builds on similar principles of apparatus design. We used phenylephrine and Krebs fluid flowing through the cannulated ureter to reliably cause peristalsis. In agreement with the work of Tsuchiya and Takei, 15 with only fluid flowing through the ureter, spontaneous, rhythmic (every 45–60 s) peristalsis was observed in some preparations. Spontaneous peristalsis after being placed in Krebs solution was often dependent on the medical history of the ureter (human specimen) or the length of the previous surgical procedure (porcine specimens). Because we could not rely only on spontaneous peristalsis, we elected to use phenylephrine to reliably induce peristalsis. In this regard, we used a near maximal dose of phenylephrine that would reliably cause peristalsis.
Of note, phenylephrine is a selective α1 α-adrenergic receptor agonist, but does have some affinity for α2 alpha adrenergic receptors 10 In research into calcium channels of rat prostatic neuroendocrine cells, Kim and colleagues 16 showed that α1 α-adrenergic receptor agonists open calcium channels and that α2 alpha adrenergic receptor agonists close these same calcium channels. Accordingly, we are currently comparing phenylephrine with electrical stimulation to see if there is any difference in the ureter's response.
We have also found that two animals of the same species can have ureters that behave radically different. While we have not seen a significant difference in proximal vs distal portions of the ureter in the same animal, the variability of the degree of ureteral cleaning at the beginning of the experiment may damage the ureter by removing periureteral nerve tissue and may furthermore result in variations in the extraluminal rate of diffusion based on the degree of gross stripping of periureteral fat. We would not expect to see this on the intraluminal surface, because this is not harmed during processing of the ureteral segment.
Finally, the concentration response curve is typically done by adding the drug (in this case, nifedipine) and allowing the response to come to a new equilibrium before adding the next concentration. In these experiments, a standard time interval (30 minutes) was used. Thus, equilibrium may not have been reached. As a consequence, the reported concentrations, 1 and 10.2 uM, could possibly be overestimates of the true maximal inhibitory concentrations of nifedipine.
Conclusions
With the aforedescribed unique apparatus, we are able to rapidly test medications for ureteral relaxation properties before use in in-vivo animal experiments. This allows us to quickly and inexpensively test a large number of substances to best choose those that might prove most favorable in the animal model. The apparatus we have developed also allows one the ability to selectively test medications intraluminally at a specific concentration and a specific flow; accordingly, the pharmacologic properties of the urothelial barrier can be characterized.
Footnotes
Acknowledgments
This work was supported in part by generous funding from the Omeros Corporation in Seattle, WA. The authors wish to thank Scott M. Summers, Jeffrey M. Herz, Clark E. Tedford, and Geoffrey N. Box for their contributions to the work.
Disclosure Statement
No competing financial interests exist.