
Abstract
Purpose:
To report our experience with robot-assisted partial nephrectomy (RAPN) in obese patients compared with a contemporary cohort of nonobese patients.
Patients and Methods:
We defined obesity as a body mass index (BMI) ≥30 kg/m2. From June 2004 to September 2009, 97 patients underwent RAPN at our institution, of whom 49 were obese (group 1) and 48 were nonobese (group 2, BMI <30 kg/m2). We compared demographics, operative data, complications, and pathological outcomes between these two groups.
Results:
The average BMI for the obese group was 36.2 kg/m2 (range 30.3–49) compared with 25.7 kg/m2 (range 20.5–29.7) for the nonobese group. Median tumor size was 2.5 versus 2.3 cm for obese and nonobese groups, respectively. Obese patients had a larger median estimated blood loss (150 vs.100 mL, p = 0.027) and a trend toward a longer median operative time (265 vs. 242.5 minutes, p = 0.085) and median warm ischemia time (26.5 vs. 22.5 minutes, p = 0.074), but this did not achieve statistical significance. An intraoperative complication occurred in one patient in each group. The postoperative complication rate was not statistically significant between the two groups (8.3% vs. 4.3%, p = 0.377). The median hospital stay was 2 days for both groups.
Conclusions:
RAPN is safe and feasible in obese patients. Obese patients had a higher estimated blood loss and a trend toward greater operative time and warm ischemia time, which did not achieve statistical significance.
Introduction
Nephron-sparing surgery has emerged as the preferred option for managing small renal tumors, comparing favorably with radical nephrectomy from the standpoint of long-term oncological control with the advantage of preservation of renal function. 5
Robot-assisted partial nephrectomy (RAPN) is an alternative to laparoscopic partial nephrectomy (LPN) with a number of studies demonstrating its feasibility and safety for renal tumors. 6 –9 Although the feasibility of LPN in obese patients has been described, 10,11 to the best of our knowledge, no studies to date evaluate RAPN in obese patients. The objective of this study was to report our experience with RAPN in obese patients and compare surgical, functional, and short-term oncologic outcomes with a cohort of nonobese patients.
Patients and Methods
From June 2004 to September 2009, 97 patients underwent RAPN at our institution. Patients were grouped into two cohorts, obese (body mass index [BMI] ≥30 kg/m2) and nonobese (BMI <30 kg/m2). Data were reviewed from a prospectively maintained, institutional review board-approved, computerized database. Demographic and perioperative variables were compared between groups.
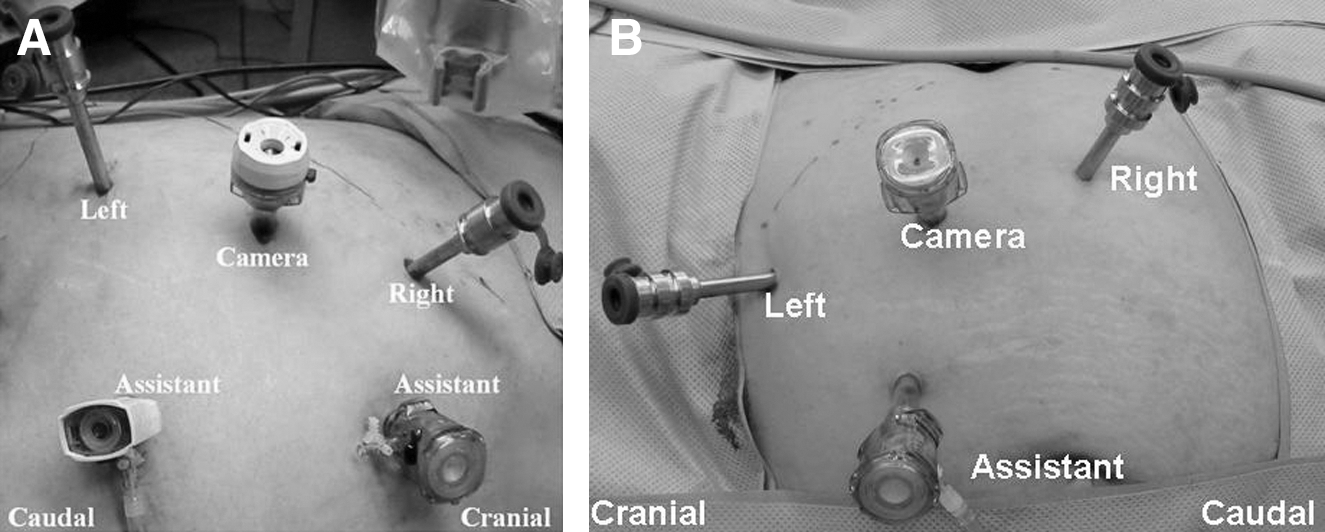
Our RAPN technique has been previously described 12 –14 and a detailed description of technique is beyond the scope of this report. Briefly, patients are placed in flank position, and ports are placed as demonstrated in Figure 1A and B with the pannus over the edge of the table. An extra-long 12-mm port is placed laterally for the robotic camera. The entire port template is shifted laterally compared with nonobese patients. In morbidly obese patients, extra-long robotic trocars may be used.
The daVinci surgical system (Intuitive Surgical, Sunnyvale CA) was used in all cases. For select large or challenging tumors, a four-arm approach was used for kidney retraction and positioning. Bowel mobilization and kidney exposure are performed with complete robotic assistance. The renal hilum is dissected and the perinephric fat is reflected to expose the tumor. Laparoscopic ultrasonography is used to confirm tumor location and delineate margins of resection. Hilar occlusion is performed in the majority of cases using either laparoscopic bulldog clamps or a Satinsky clamp. For larger or more endophytic or central tumors, we generally clamp both the artery and vein. For smaller more peripheral tumors, we clamp just the artery. Tumor excision is performed sharply with robotic scissors ensuring adequate surgical margins. Large vessels and collecting system defects in the resection bed are suture ligated. The renal capsule is closed using 0 polyglactin sutures anchored with hemolock clips and tightened using the sliding hemolock clip technique. 15 Bolsters and thrombogenic agents were used for larger defects. A drain was routinely placed that was removed before discharge if the drain creatinine was normal.
Perioperative factors analyzed included total operating room time, warm ischemia time, hilar clamping technique, estimated blood loss, and length of hospital stay. Complications were recorded using the Clavien classification system. 16 Change in estimated glomerular filtration rate (eGFR) was recorded from baseline to follow-up 1 to 3 months postoperatively using the Modification of Diet in Renal Disease equation. 17 Pathological factors analyzed included pathologic tumor size, histology, pathologic stage (2002 AJCC staging criteria), Fuhrman grade, and margin status. Preoperative and perioperative results, as well as pathological and functional outcomes data, were retrospectively analyzed and compared between groups. The assumption of normality was tested for the entire distribution using the Kolmogorov–Smirnov test, the Shapiro–Wilk test, and graphical design. The obese and the nonobese cohorts were then tested separately using the same methods. Of all the variables in the analysis, tumor size, American Society of Anesthesiologists (ASA) score, operative time, warm ischemia time, estimated blood loss, length of stay, and pathologic size were non-normally distributed. The Mann–Whitney U-test was used to compare the median values of these variables. The independent samples t-test and Pearson Chi-squared test were used as appropriate. For homogeneity of variances the Levene's test was used; the Welch's t-test was used instead of the independent samples t-test if nonhomogeneity was confirmed. All tests were two-tailed with the significance set at 0.05. All statistical analyses were performed using PASW software (PASW 17; IBM, Chicago, IL).
Results
Of the 97 patients who underwent RAPN at our institution during the study period, a total of 49 (50.5%) were considered obese (BMI ≥30 kg/m2). Baseline demographics and radiographic tumor characteristics are summarized in Table 1. The mean BMI in group 1 was 36.2 (30.3–49) and in group 2 was 25.7 (20.5–29.7). There were no significant differences in baseline characteristics between groups except that obese patients had a higher rate of hypertension (75.5% vs. 54.1%, p = 0.027) and a trend toward a higher rate of diabetes mellitus (28.6% vs. 14.6%, p = 0.092). Median radiographic tumor size was 2.5 cm (0.7–5.8) and 2.3 cm (0.7–7.9) for groups 1 and 2, respectively (p = 0.152). The number of clinical T1b tumors was 11 (22.5%) in the obese group and 5 (10.4%) in the nonobese group.
BMI = body mass index; ASA = American Society of Anesthesiologists.
Perioperative outcomes for obese versus nonobese patients are listed in Table 2. Obese patients had a larger median estimated blood loss (150 vs. 100 mL, p = 0.027) and a trend toward a longer median operative time (265 vs. 242.5 minutes, p = 0.085) and median warm ischemia time (26.5 vs. 22.5 minutes, p = 0.074). The majority of cases were performed under warm ischemia with hilar clamping in both groups (67.4% vs. 75%, p = 0.537). Estimated eGFR was lower preoperatively in the obese group (67.7 vs. 77.3 mL/minute, p = 0.018). Despite the trend to longer warm ischemia times in the obese group, the mean decrease in 1 to 3 months eGFR from baseline was similar in both groups.
eGFR = estimated glomerular filtration rate (mL/min/1.73 m2); IQR = interquartile range.
A comparison of intraoperative and postoperative complications is summarized in Table 3. There was one intraoperative complication in the obese group in which an enterotomy was made during lysis of adhesions in a patient with prior abdominal surgery, which was repaired robotically without sequelae. One patient in the nonobese group was converted to a radical nephrectomy because of bleeding. Four patients in the obese group had postoperative complications versus two patients in the nonobese group.
Converted to radical nephrectomy because of bleeding.
Both patients in the obese group stabilized after bedrest and transfusion. One patient in the nonobese group with platelet dysfunction was reexplored because of bleeding from a subcapsular hepatic hematoma.
Patient with solitary kidney required one treatment of dialysis postoperatively for acute renal failure.
Comparisons of pathologic variables are shown in Table 4. Final pathology revealed malignant tumors in 81.6% and 66.7% of patients in groups 1 and 2, respectively. Median pathologic tumor size was 2.4 cm (IQR, 1.9–3.7) versus 2 cm (IQR, 1.5–3.5) in groups 1 and 2, respectively (p = 0.251). One patient in each group had a positive surgical margin. Both patients had stage T1a chromophobe RCC with a focal microscopic positive margin and are undergoing close observation with no evidence of local recurrence at 12-month follow-up.
AML = angiomyolipoma.
Discussion
Obesity has been confirmed as a risk factor for RCC. 4 Donat et al 17 retrospectively evaluated BMI data in 1137 patients who underwent nephrectomy for RCC. The study found significant increases in blood loss and operative time with increasing BMI. Although BMI ≥30 kg/m2 was associated with a higher proportion of clear cell histology, comorbidity, and surgical morbidity, it did not adversely impact overall or progression-free survival. In our study, a greater percentage of patients in the obese group had clear cell RCC, but this difference was not statistically significant. In addition, no difference in pathological stage was noted in our results.
Columbo et al 10 reported on their experience with LPN in 140 obese patients compared with a cohort of 238 nonobese patients. Obese patients did not have a statistically significant difference in mean estimated blood loss (310 vs. 249 mL), operating time (3.4 hours), or warm ischemia time (31 vs. 32 minutes). Intraoperative and postoperative complication rates were also similar between obese and nonobese groups (5.7% vs. 8%, and 13% vs. 9%). The mean hospital stay was 2.8 days for the obese group and 3.5 days for the nonobese group. Romero et al 11 compared perioperative outcomes of laparoscopic and open partial nephrectomy in obese and nonobese patients. There were 56 obese and 56 nonobese patients who underwent LPN. There were similar perioperative outcomes for the obese and nonobese cohorts undergoing LPN, except that obese patients had a higher median blood loss (300 vs. 200 mL). Lifshitz et al 18 evaluated patient and tumor characteristics that might predict prolonged warm ischemia time during LPN. On multivariate linear regression analysis, tumor size, BMI, and central tumor location were independent predictors of longer warm ischemia time. The group concluded that patients with 2 or more of certain risk factors, including BMI ≥30 kg/m2, tumor >4 cm, and a centrally located tumor, were five times more likely to have warm ischemia time >30 minutes than patients without the risk factors (p = 0.002). In our study, the warm ischemia time was slightly higher in the obese group, but this difference was not statistically significant.
Although these studies demonstrate the feasibility of LPN in obese patients, our study is the first to evaluate RAPN with a special focus on obese patients. In the present study, obese patients had a greater blood loss and a nonsignificant trend toward greater operative time and warm ischemia time. Of note, our warm ischemia times were shorter than comparable laparoscopic series in obese patients (Table 5). Postoperative complications were also similar between the two groups.
Forty-five patients through retroperitoneal access.
Mean.
Median.
NA = not available.
Limitations of our study include the retrospective nature of our analysis and single-center experience. Only early oncological and functional outcomes are available at this time, and further studies with longer follow-up are needed. Our assessment of GFR at 1 to 3 months provides only a single assessment of postoperative renal function. However, we feel that evaluation of renal function at this time point does provide a meaningful assessment. Medical factors such as hypertension, diabetes mellitus, and chronic kidney disease are more common in obese patients and may cause worsening of renal function over time. By assessing GFR at 1 to 3 months, it allows time for recovery of renal function while minimizing confounding medical factors that may worsen renal function over time. Our total operative time was longer than the corresponding laparoscopic studies in Table 5, although our warm ischemia time was lower. This may be, in part, because of the time for robotic setup. Another potential factor is that we are a training institution and residents and fellows may be involved in portions of the cases before and after the duration of hilar clamping, which adds to operative time. When we divided our cases into quartiles (25, 24, 23, and 25), there was a trend toward lower operating room time in the later quartiles that did not reach statistical significance. This may have been caused by the more challenging nature of the tumors operated on as our experience grew. The last-quartile patients were older and had a higher BMI, median ASA score, median tumor size, and endophytic component of the tumor (data not shown).
We conclude that RAPN in obese patients is safe and feasible, showing comparable outcomes to nonobese patients. We do not necessarily advocate robotic assistance for all obese patients undergoing partial nephrectomy, but robotic assistance may help some obese patients to achieve the convalescence benefits of minimally invasive partial nephrectomy. Robotic assistance may also help overcome technical challenges of LPN in obese patients. Future studies with extended follow-up are necessary to further evaluate the long-term efficacy of RAPN in obese patients.
Footnotes
Disclosure Statement
No competing financial interests exist.