
Abstract
Double-J stents that are inserted to span the ureterovesical anastomosis at ureteoneocystostomy may be associated with problems such as coiling or migration. An unusual occurrence of retroperitoneal migration of a Double-J stent after bilateral open ureteroneocystostomy is reported. The migrated stents were retrieved laparoscopically with construction of a laparoscopic ureteroneocystostomy.
Introduction
Case Report
A 32-year-old woman was referred to our clinic for management of a migrated DJ stent. On inquiry, a history of laparoscopic hysterectomy that was performed 2 months earlier was elicited. At 4 hours after the procedure, she experienced anuria and exploration was performed. Bilateral lower ureteral injuries were identified, and bilateral refluxing ureteroneocystostomies were created with insertion of 6F DJ stents bilaterally. Detailed operative records were unavailable. No skiagrams were evaluated after the reimplantation procedure.
At 6 weeks postsurgery, the patient was scheduled for stent removal. Operative records narrated removal of the left DJ stent through cystoscopy. The right-side DJ stent could not be visualized at this cystoscopy, and the patient was referred for expert treatment.
At presentation to our center, she was normothermic, and vital signs were normal. Abdominal examination revealed previous surgical scars. Blood parameters, including renal function, were normal. The skiagram (Fig. 1) revealed two DJ stents on the right side. CT urography was ordered to identify the exact pathology. CT revealed (Fig. 2) a dilated right pelvicaliceal system with two DJ stents on the right side. Both stents appeared extravesical. The primary treating physician could not be reached for communication, and no explanation regarding this finding was obtained.
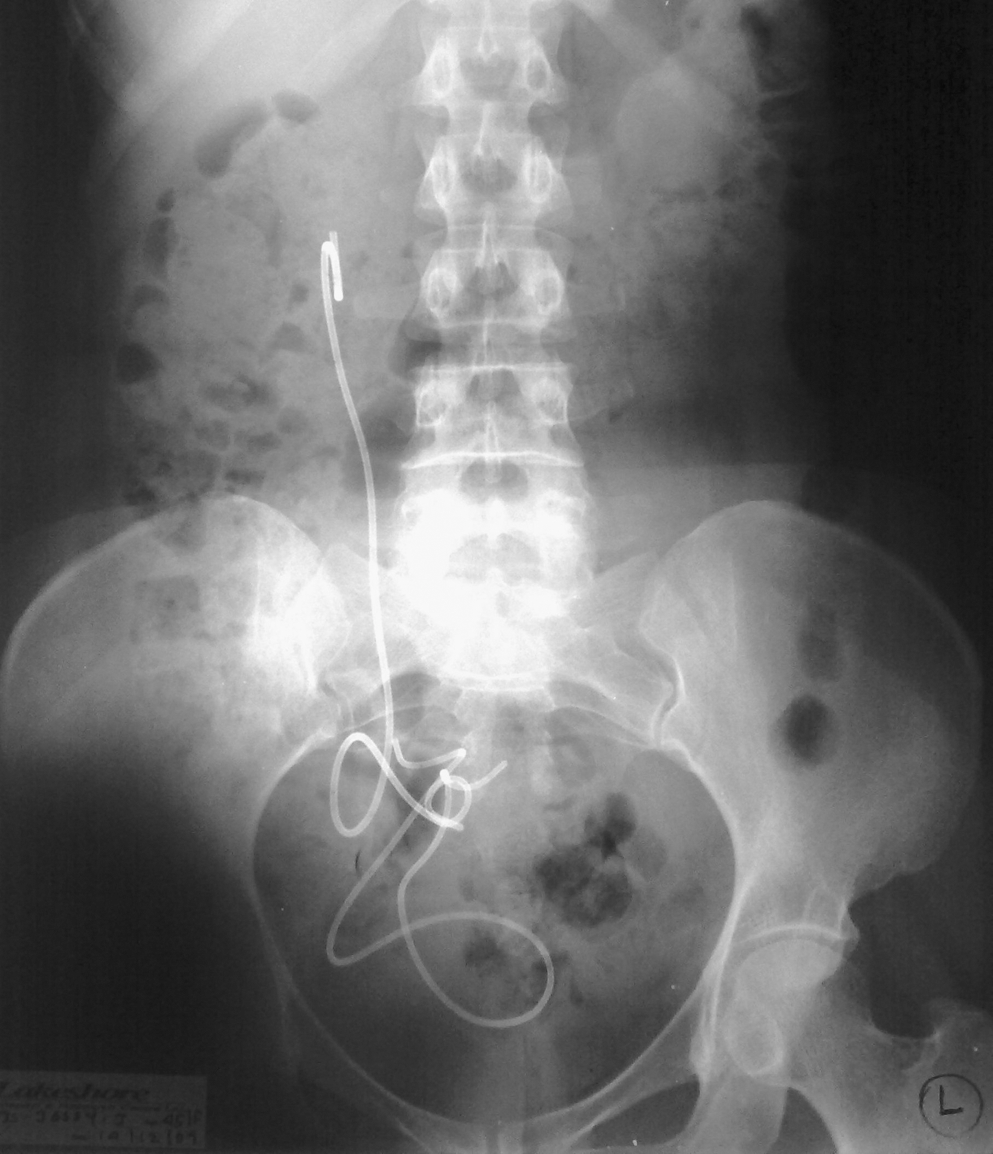
Skiagram of the kidneys, ureters, and bladder at presentation.
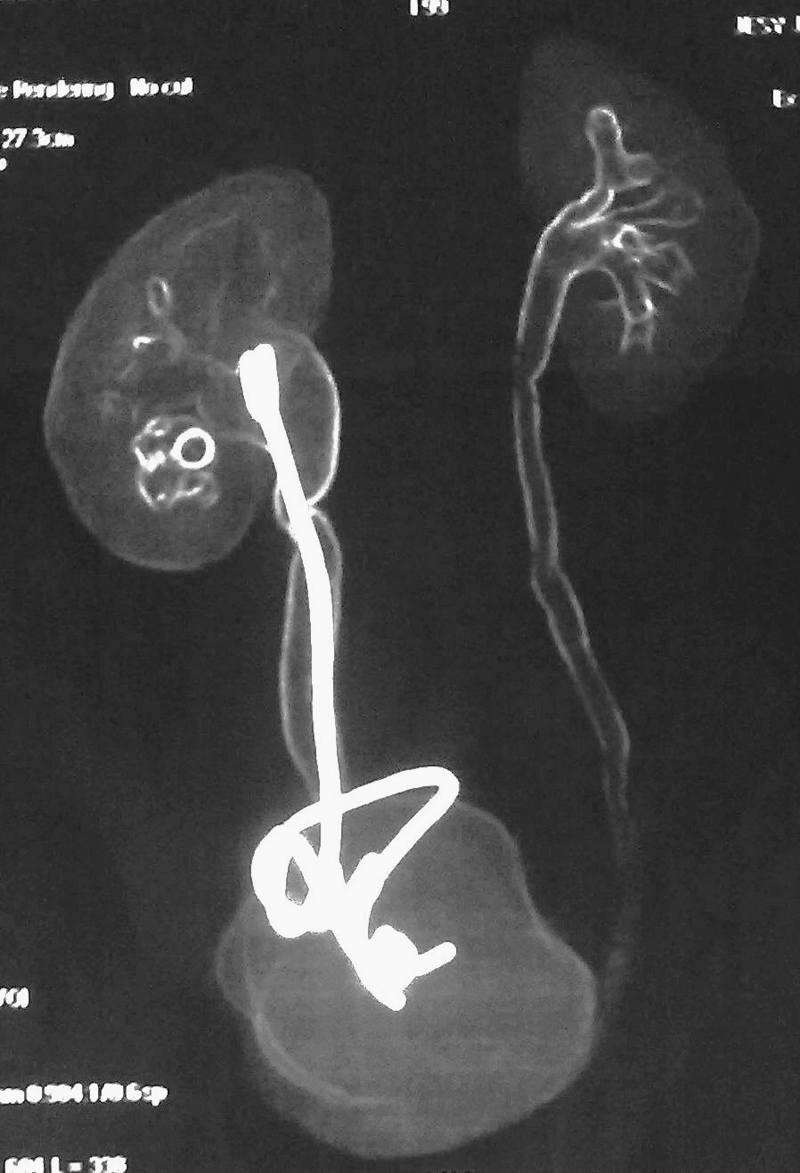
CT urogram showing two right-sided Double-J stents.
Cystoscopy followed by laparoscopy was planned for the patient to identify the location of the stents and subsequent retrieval. Cystoscopy revealed a normal appearing left neoureteral orifice and fibrosed right neoureteral orifice. No intravesical stent was visible. At laparoscopy, one stent (Fig. 3) was discernible extraperitoneally on the right side, extending toward the midline. The lower end of the other stent (Fig. 3) was projecting outside the right lower ureter with surrounding adhesions. Both stents were retrieved.
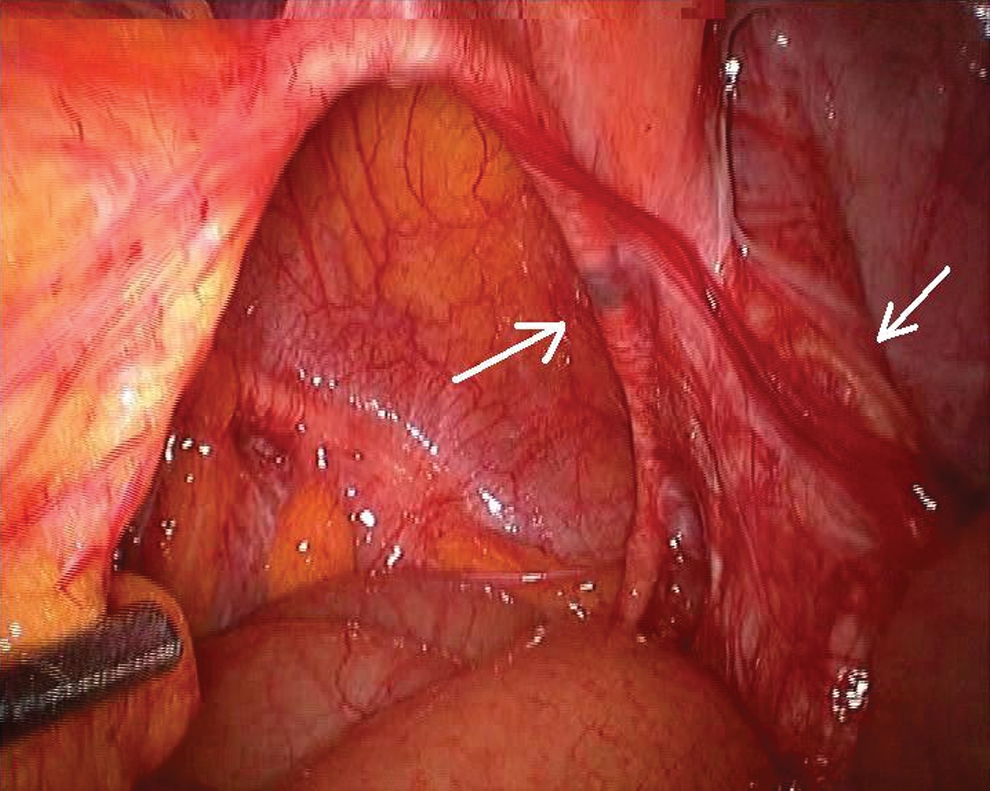
Intraoperative image at laparoscopy—two Double-J stents in the retroperitoneum.
Both the stents were 6F in diameter and 26 cm in length. The right lower ureter stricture segment was excised, and a fresh ureteroneocystostomy with psoas hitch was constructed laparoscopically. A new 6F DJ stent was placed across the anastomosis. (Fig. 4) The patient tolerated oral intake on the evening of the same day. The drain was removed on the following day. The patient was discharged with a right DJ stent. The stent was removed at 6 weeks. Cystoscopy at the time of stent removal confirmed a healthy right neoureteral orifice. The patient remains well at follow-up. Follow-up CT urography at 3 months postoperatively showed resolution of the pelvicaliceal dilatation with a satisfactory drainage pattern.

New Double-J stent inserted during laparoscopic ureteroneocystostomy.
Discussion
Ureteroneocystostomy is a well-recognized technique for reconstruction of lower segment ureteral loss that is sustained at laparoscopic hysterectomy. 1 During this procedure, a DJ stent is placed to span the ureterovesical anastomosis; the stent is removed 3 to 6 weeks after the procedure. 2 The DJ stent is often inserted without fluoroscopy assistance and, thus, the possibility of complications such as coiling or intraureteral migration exist. 3
The upper end of the DJ stent should always be guided under C-arm control. An operating table that is compatible with the use of intraoperative fluoroscopy is essential. The lower end of the stent should be placed under direct vision. The location of the lower end of the stent may be further confirmed by cystoscopy. Migration into the retroperitoneum has been a hitherto unreported occurrence.
A postoperative skiagram can confirm the location of stents in case of nonusage of fluoroscopy intraoperatively, and any abnormality can be immediately corrected. The omission of both these doctrines possibly contributed to the unfortunate happening in our case scenario.
After retrieval of the stents, a laproscopic ureteroneocystostomy with psoas hitch was performed. A psoas hitch renders additional anchorage and restricts tension at the suture line. This operative exercise was technically demanding in view of dense adhesions that were attributable to the previous two surgeries. The presence of a bladder with good capacity negated the need for flap reconstruction.
Footnotes
Disclosure Statement
No competing financial interests exist.