
Abstract
Urine leakage is an uncommon complication after renal cyst decortication that typically resolves with adequate drainage. With prolonged large volume urine leakage from a perinephric drain, however, consideration for open surgical repair must be taken into account. We present the successful management of persistent urine leakage after laparoscopic cyst decortication with endoscopic retrograde fibrin glue injection and ureteral stent placement.
Introduction
The following case describes the first reported use of retrograde endoscopic injection of fibrin glue to successfully manage a urine leak after a laparoscopic cyst decortication.
Case Report
A 46-year-old woman was transferred from an outside facility for further evaluation of a large symptomatic renal cyst. Physical examination revealed a large palpable mass in the right upper quadrant. Urinalysis and urine culture had negative findings, creatinine level was 0.8 mg/dL, and the white blood cell count was 10.5 with no bandemia. Abdominal CT was notable for a 13 × 9 cm simple cyst that extended along the posterior-lateral aspect of the right kidney with a density of 15 to 25 Hounsfield units (Fig. 1). The patient underwent a laparoscopic cyst decortication after failure of conservative management.
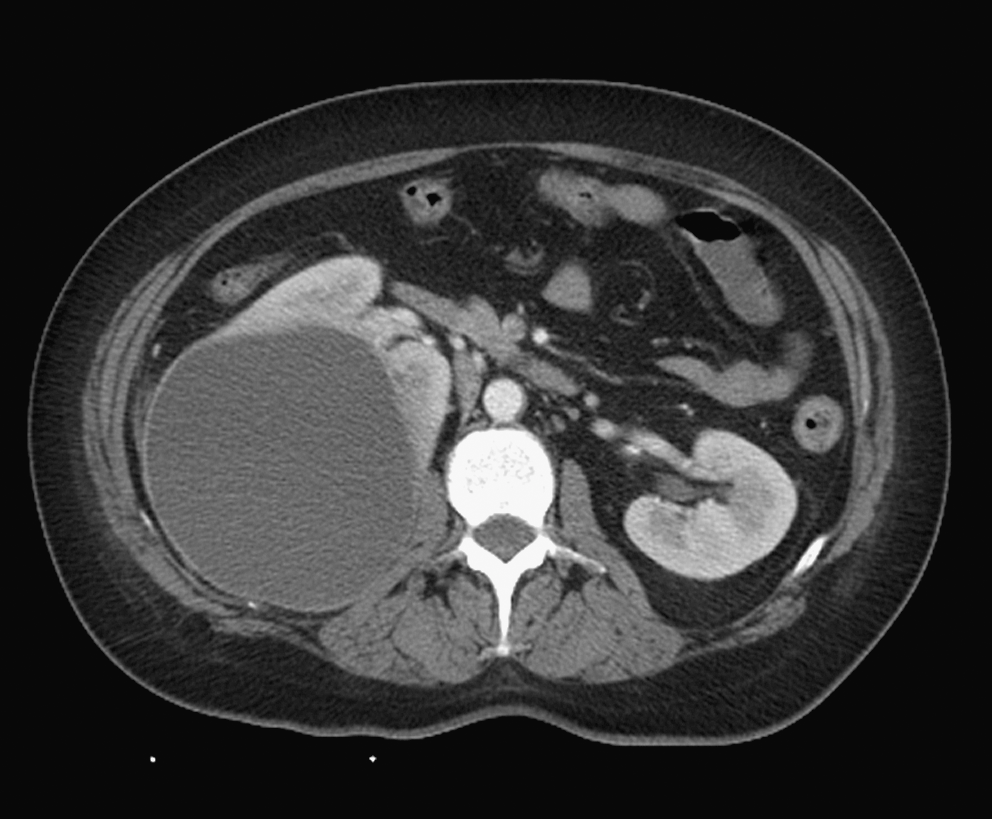
Abdominal CT scan performed for the evaluation of abdominal pain revealed a large homogeneous right posterolateral renal cyst.
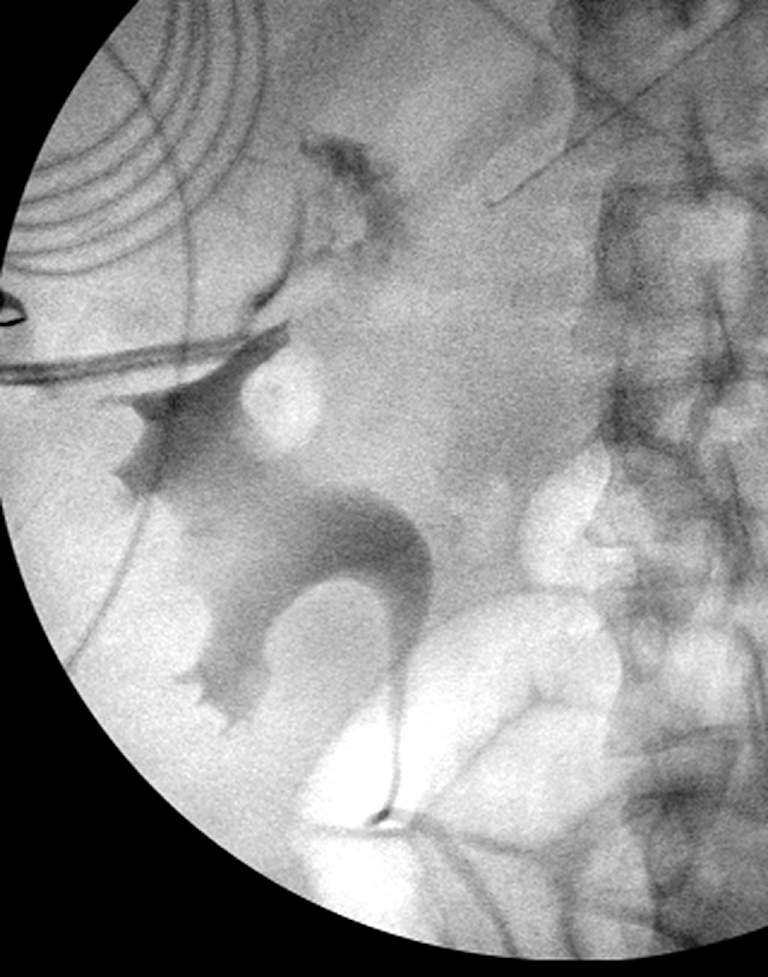
Intraoperative cystoscopy and retrograde pyelography revealed a posterolateral deflection of the collecting system, with no apparent continuity between the collecting system and cyst (Fig. 2). On entering the abdomen, multiple adhesions between the colon, liver, and abdominal wall to the right renal cyst were noted, and a rent was made within the cyst during attempts at mobilization. Purulent exudate was aspirated with subsequent cyst wall excision, ablation, and placement of a perinephric drain.

Right retrograde pyelogram confirms no continuity between the collecting system and the renal cyst.
In the immediate postoperative period, fever and peritonitis developed from a urine leak. Retrograde pyelography demonstrated contrast extravasation from a portion of the superior calices (Fig. 3). A 6F × 30 cm ureteral stent was then placed without complications. Despite maximal urinary drainage, output from the perinephric drain remained high, and the patient showed very little clinical progress. Repeated CT scan showed a fluid collection in the superior right kidney that was percutaneously drained and analyzed, revealing a noninfected urinoma.
Right retrograde pyelogram demonstrates urinary extravasation from an upper pole calix.
A CT scan 1 week later demonstrated a reduction in the size of the fluid collection. Delayed images, however, showed contrast extravasation from an apparent fistulous tract originating from a minor pole calix in the upper pole of the right kidney. At this time, open surgical repair was contemplated, but reports of endoscopic management of urinary fistulas with fibrin glue injection prompted our attempt at endoscopically repairing the upper pole caliceal injury.
Repeated retrograde pyelography confirmed the urinary leak from a minor calix in the superior pole of the right kidney. Two 5F open-ended ureteral catheters were directed into this minor calix over dual wire access with the aid of fluoroscopy and ureteroscopy, which allowed attachment of the fibrin glue applicator (Figs. 4a, 4b). With the patient in a steep Trendelenburg position, 5 mL of fibrin glue was injected, followed by ureteral stent placement. Postinjection retrograde pyelography confirmed resolution of the urine leak (Fig. 5).

5F open-ended ureteral catheters attached to the dual-chamber applicator

Retrograde pyelogram reveals resolution of urinary extravasation after retrograde injection of fibrin glue.
Initially, there was a significant decrease noted in both the perinephric and CT-guided percutaneous drain output, and the patient felt subjectively better with less abdominal pain and no fever. The perinephric drain was pulled. The remaining percutaneous drain output began to progressively increase, however. A renal scan performed in preparation for possible nephrectomy showed bilateral symmetric function and incidentally revealed no extravasation of radiotracer from the upper pole segment. The tracer was contained within the collecting system and surprisingly drained into the percutaneous catheter, indicating that the catheter was in the upper pole collecting system and not in the bed of the previously decorticated cyst. This catheter was therefore clamped, which resulted in a subsequent increase in Foley catheter output. The patient was discharged from the hospital in a stable condition. Her Foley catheter and percutaneous drain were removed at follow-up at 2 and 4 weeks, respectively, and the patient has remained asymptomatic to date.
Discussion
The standard management of caliceal injury after percutaneous, laparoscopic, or open treatment of renal cysts includes ureteral stent placement and bladder drainage. 1,3 –6 When conservative management of a urinary leak with ureteral stent placement or percutaneous drainage fails, open surgical repair is often indicated. 5,7 To avoid the morbidity of open surgery, however, minimally invasive techniques have been used to treat urinary fistulae, including endoscopic injection of fibrin glue.
There are multiple reports describing the use of fibrin glue in the endoscopic management of urinary fistulae. Sharma and colleagues 5 performed a retrospective review of seven patients with various urinary fistulae, including vesicovaginal, colovesical, ureterocutaneous, and urethrocutaneous, all of which were managed with retrograde endoscopic injection of fibrin glue. At 1 year of follow-up, the rate of fistula resolution was 75%.
Although open surgery remains the gold standard for urinary tract fistula repair, endoscopic management with fibrin glue may avoid the morbidity that is associated with open repair. 5 Dolay and associates 8 describe management of a rectourethral fistula with endoscopic injection of fibrin glue. Antegrade injection of fibrin glue during percutaneous nephrolithotomy has also been described and may obviate the need for percutaneous nephrostomy tube placement, thereby decreasing patient pain and hospital stay. 9 Kim and coworkers 10 describe the use of multiple hemostatic agents, including fibrin glue, on pigs undergoing percutaneous nephrolithomy. Furthermore, Evans and colleagues 11 describe the topical use of fibrin sealants for successful management of genitourinary injuries—both traumatic and surgical—and genitourinary fistulae.
Fibrin glue is composed of supraphysiologic levels of fibrinogen, thrombin, calcium, and aprotonin (fibrinolysis inhibitor), all of which are critical to its role as a hemostatic agent and tissue sealant. 5,12,13 These favorable characteristics have established fibrin sealant as an important and useful adjunct for surgery with multiple applications ranging from skin grafts, vascular anastomoses, and, with increased popularity and success, in genitourinary problems and complications. 11 Injection of fibrin glue into the urinary tract may potentially cause complications. In vitro, fibrin sealant in urine remains as a solid clot for 24 hours and transforms into a cohesive mucoid gel at 5 days. 14 Fibrin glue could potentially migrate and cause obstruction of the ureteropelvic junction, ureter, or a ureteral stent; however, there have been no clinical reports to date of such complications.
Administration of two-component fibrin glue via separate open-ended catheters, as used in our patient, also prevents inadvertent spillage of activated glue. In addition, our patient has had no known complications secondary to fibrin glue injection.
Injury to the renal calix likely occurred during ablation of the renal bed after cyst decortication, but the presence of an unrecognized caliceal diverticulum cannot be definitively excluded. Our suspicion for a caliceal diverticulum was low, however, given the normal appearance of the collecting system on preoperative retrograde pyelography and CT scan. In our patient, retrograde endoscopic application of fibrin sealant obviated the need for open surgical management of a prolonged urine leak. The patient improved clinically almost immediately after fibrin glue injection, which was discordant with her high percutaneous drain output. The probable explanation is that the drain migrated into the collecting system—effectively making the drain a nephrostomy tube. Clamping the drain led to an increase in her Foley catheter output as expected, and both drain and Foley catheter were eventually removed with no long-term sequelae.
Conclusion
For persistent urine leaks after laparoscopic cyst decortication despite maximal drainage with a ureteral stent, Foley catheter, and percutaneous drain, it is reasonable to attempt retrograde endoscopic injection of fibrin glue to seal the collecting system injury and avoid open repair.
Footnotes
Disclosure Statement
No competing financial interests exist.