
Abstract
Purpose:
To evaluate the efficacy and safety of percutaneous nephrolithotomy (PCNL) for patients in the supine position vs prone position.
Materials and Methods:
Eligible studies were identified from electronic databases (Cochrane CENTRAL, Medline and EMBASE). The database search, quality assessment, and data extraction were independently performed by two reviewers. Efficacy (stone-free rate, operative time) and safety (complication, such as fever and transfusion rate) were explored by using Review Manager 5.0. Sensitivity analysis was performed to explore the influence of low-quality studies.
Results:
Two randomized controlled trials and two case-control studies including 389 patients met the inclusion criteria. Meta-analysis of extractable data showed that PCNL in the supine position was associated with a significantly shorter operative time than PCNL in the prone position (mean difference
Conclusion:
PCNL in the supine position took a shorter operative time than the prone position, but both positions appeared to be equivalent with regard to the stone-free rate and complication rate, transfusion rate, and fever rate. In brief, PCNL in the supine position is as effective and safe as PCNL in the prone position and was an alternate option for removal of renal calculi in PCNL.
Introduction
With the rising number of PCNL procedures and increasing confidence and experience of urologists, the supine position has been developed to overcome these drawbacks and simplify the procedure. In 1987, Gabriel Valdivia and colleagues 6 described their first case of PCNL in the supine position. Eleven years later, he and coworkers presented 557 consecutive PCNL performed in this way. 6 Since then, several other investigators have reported their experience with this technique.
Compared with the prone position, the supine position has the following advantages: Safer and easier for the patient; less cardiovascular change; no need for patient repositioning (with less operative time and less relevant risk of nervous system injuries); and more comfortable and less radiation exposure to the surgeon; but also allows a simultaneous PCNL and ureteroscopy. 4,5
Despite the potential advantages, the supine position necessitates more lateral displacement of the renal puncture site than the prone position, which may increase the possibility of visceral injuries and cause trauma to intrarenal vessels. 3
Therefore, controversy has emerged as to which is the better position for PCNL. Most of the information relevant to the patient position of PCNL comes from case series and observational studies. Although these studies may enhance the feasibility of PCNL, they often accepted an idea beneficial to them, but ignored a different idea; thus, considerable bias emerged. Currently, the choice depends on surgeon preference and experience. 7 Therefore, it is necessary to undertake a systematic review and meta-analysis to evaluate the efficacy and safety of PCNL with the patient in the prone or supine position.
Materials and Methods
We searched the Electronic databases as follows: Cochrane central register of controlled trials (CENTRAL), Medline, EMBASE. The reference lists of the identified reports, reviews, and other relevant publications were hand searched. The following Medical subject heading terms and key words were used to identify relevant studies: percutaneous nephrolithotomy or nephrostomy, percutaneous or percutaneous nephrostomy or nephrostomy or PCNL or PNC or PNL. Then we combined those with supine or supine position. Articles in all languages were sought. Randomized controlled trial (RCT), quasi randomized controlled study, case-control study and cohort study were included if they met the criteria that comparing the efficacy and safety of the PCNL in the supine position and prone position. All titles and abstracts retrieved by electronic searching were screened by two reviewers. Discrepancy was resolved in consultation with the third reviewer. Non-English papers were translated before assessment.
Our primary outcome was the stone-free rate, followed by operative time, complication rate, transfusion rate, and fever rate as secondary outcomes. Stone free was defined as no stone with maximum diameter >5 mm evaluated by kidneys-ureters-bladder radiography or ultrasonography after the first postoperative day. Operative time was defined as the total time spent in the surgical suite, including surgical, anesthetic, and equipment setup, positioning and repositioning time. Fever was defined as body temperature >38°C during hospital stay after surgery. Fever, urinary tract infection, renal colic, urinary leakage, septicemia, hemorrhage necessitating blood transfusion and organ injuries were considered as complications.
The relevant data were extracted by two reviewers. When the data were missed, we attempted to contact the trial authors to request missing data; otherwise, missing data were imputed by calculating from the confidence interval (CI), t statistics, P values or individual variances for intervention and control groups. The quality of RCT studies was assessed by the Cochrane Collaboration's tool, 8 which included assessment of sequence generation, allocation concealment, blinding, incomplete outcome data, selective reporting of outcomes, and other possible sources of bias. The non-RCT studies were assessed with a modification of the Newcastle-Ottawa Scale. 9 Scores 5 to 9 were defined as high quality, and a score <5 as low quality. Two reviewers performed the quality assessment independently. Discrepancy was resolved in consultation with the third reviewer.
Specifically, heterogeneity was analyzed using the chi-square test on N-1 degree of freedom, with an alpha of 0.10 and with the I2 test. I2 values of 25%, 50%, and 75% correspond to low, medium and high levels of heterogeneity. In case of lack of heterogeneity, fixed-effects models were used for the meta-analyses; otherwise, random-effects models were used. The stone-free rate, complication rate, transfusion rate, and fever rate were assessed using odds ratio (OR) with 95% CI. For operative time, the mean difference (MD) with 95% CI was calculated. All analyses were performed by the Review Manager software version 5.0 (The Cochrane Collaboration, Oxford, UK). Publication bias was evaluated by using a funnel plot. When data are available and sufficient, subgroup analysis was performed by grouping the trials on RCT group and case-control study group to explore possible heterogeneity. Sensitivity analysis was performed to explore the influence of low quality studies.
Results
Sixty-three studies were identified from the electronic database and hand search. After study assessment, we identified four trials 10 –13 — two RCTs and two case-control studies—that met our including criteria (Fig. 1).
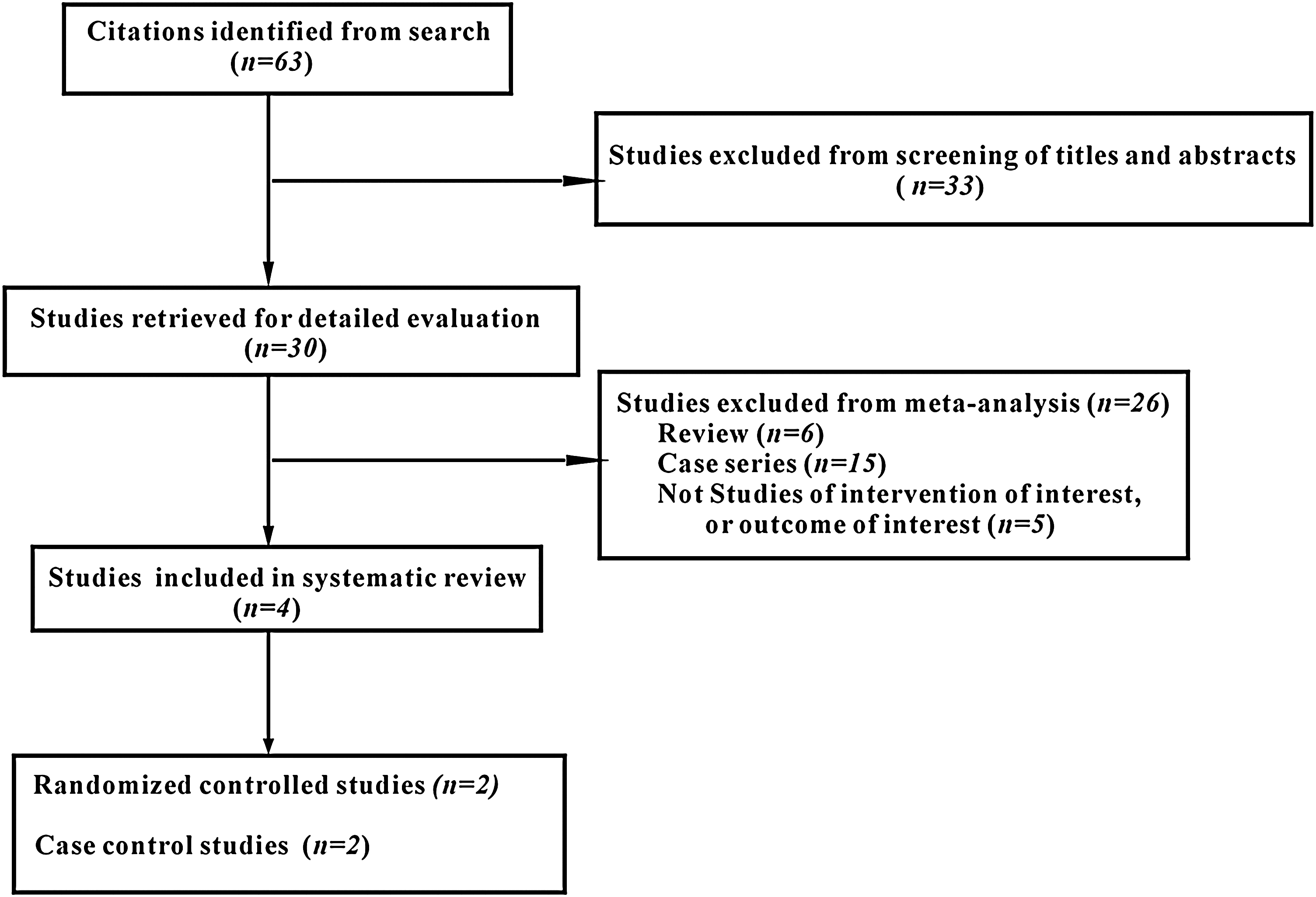
Literature flowchart of meta-analysis.
Study characteristics
There are 389 patients involved in the four trials: 207 receiving prone position treatment and 182 receiving supine position treatment. Table 1 shows the study characteristics of the four studies included in the systematic review. Baseline information was comparable between supine and prone position groups.
RCT = randomized controlled study; CCS = case control study; A-V = arteriovenous.
Quality assessment showed that one of the case-control studies 12 was deemed as high quality, the other, 11 as low quality. Although two RCTs 10,11 were adequate in sequence generation and incomplete outcome data, inadequate in allocation concealment and blinding, because of the limitation of ethics factor and characteristic of surgery studies, they were deemed as high quality.
The included studies had several limitations, however. Three studies 11 –13 described their supine position with a water bag below the ipsilateral flank; one study 10 described its supine position without the bag or cushion under the flank. In the definitions of the outcome of operative time and success rate, differences were found among included studies. Shoma and associates 13 did not report operative time in their study. We contacted the authors for these missed or incomplete data, but nothing could be provided. Therefore, those data were not included in the meta-analysis. De Sio and colleagues 11 reported mean operative time with range and P value; the standard deviation was estimated using the statistical method. 8
Efficacy
Stone-free rate
All studies including 389 patients reported success rates for PCNL in the supine and prone position. Heterogeneity was not observed in pooled analysis (P = 0.94; I2 = 0%). In meta-analysis of four studies, their total stone-free rate was 83.5% (152/182) in the supine position vs 81.6% (169/207) in the prone position (fixed-effect model; OR: 1.16; 95% CI: 0.68–1.98; P = 0.59), indicating that there was no significant difference between the two groups (Fig. 2A). After deleting the data of case-control studies, sensitivity analysis demonstrated that there was still no statistical significance between the supine position and prone position (fixed-effect model; OR: 1.03; 95% CI: 0.43–2.49; P = 0.95; I2 = 0%). This indicated that the meta-analysis was little influenced by case-control studies.

Operative time
Three studies including 259 patients reported operative time for PCNL in both positions. Heterogeneity was observed in the pooled analysis (P = 0.10; I2 = 57%). Meta-analysis for RCT combined with case-control study demonstrated a shorter operative time for PCNL in the supine position compared with PCNL in the prone position (random-effect model; MD: −24.84; 95% CI: −34.45 to −15.23; P < 0.00001) (Fig. 2B). After deleting the data of case-control studies, sensitivity analysis showed a statistical significance for operative time in the supine and prone position (fixed-effect model; MD: −29.98; 95% CI: −37.88 to −22.08; P < 0.00001; I2 = 0%). This indicated that the meta-analysis was little influenced by case-control studies.
Safety
Complication rate
Of the four studies that reported complications, De Sio and associates 11 and Shoma and coworkers 13 showed slightly higher complication rate in the supine position, and the other two studies reported more complications in the prone position. 10,12 None of the four studies had statistical difference. No heterogeneity was observed in the pooled analysis (P = 0.57; I2 = 0%). Meta-analysis of the four studies showed that both positions had similar complication rates (fixed-effect model; OR: 1.09; 95% CI: 0.67–1.80; P = 0.72) (Fig. 3A). After deleting the data of case-control studies, sensitivity analysis showed no significant difference was found between the supine position and prone position (fixed-effect model; OR: 1.29; 95% CI: 0.61–2.76; P = 0.50; I2 = 0%). Meta-analysis was little influenced by case-control studies.

Transfusion rate
Four studies reported transfusion rates. De Sio and colleagues 11 reported no blood transfusion was needed in their trial; therefore, it is impossible to integrate their data with the others. Heterogeneity was not observed in pooled analysis (P = 0.62; I2 = 0%). Three studies including 314 patients showed that the supine position had a slightly higher transfusion rate, without statistical significance. Meta-analysis of three studies showed that both groups had similar transfusion rates (fixed-effect model; OR: 2.19; 95% CI: 0.93–5.13; P = 0.07) (Fig. 3B). After deleting the data of case-control studies, sensitivity analysis showed no significant difference was found between the supine position and prone position (fixed-effect model; OR: 3.08; 95% CI: 0.75–12.61; P = 0.12). Meta-analysis was little influenced by case-control studies.
Fever rate
Three studies reported the fever rate. They all showed that PCNL in the supine and prone position had a similar fever rate without statistical significance. The medium level of heterogeneity was observed in pooled analysis (P = 0.18; I2 = 42%). Meta-analysis of three studies showed that both groups had a similar fever rate (fixed-effect model; OR: 0.39; 95% CI: 0.13–1.16; P = 0.09) (Fig. 3C). After deleting the data of case-control studies, sensitivity analysis did not find statistical significance between the supine position and prone position (random-effect model; OR: 0.43; 95% CI: 0.02–10.79; P = 0.61; I2 = 65%). Meta-analysis was little influenced by case-control studies.
Discussion
To our knowledge, this study is the first systematic review with meta-analysis on PCNL in the supine and prone positions. Two former systematic reviews had reviewed the supine and prone position in the procedure of PCNL. 4,5 With insufficient comparative studies, however, they included case series and only depicted results without statistics in their studies; thus, their results might have considerable bias and confound readers.
In our systematic review and meta-analysis, we made precise search strategy, executed it with a librarian and strengthened our meta-analysis with sensitivity analysis. By doing so, we expected to include all of the studies related to PCNL in a comparison between supine position and prone position, hoping to reduce the confounding, limit the bias, and draw a scientific and statistically robust conclusion. A major concern with the current topic, however, is that only two RCTs met the criteria of the systematic review. 10,11 RCTs are considered the gold standard trial design for evaluating and comparing intervention by reducing bias to a minimum. To expand the number of included trials, we assessed the other two case-control studies. 12,13 Case series were not adopted for our systematic review because of varying quality.
PCNL is traditionally performed in the prone position, because it was initially considered to be the safest approach to the kidney. 3 In our study, both the meta-analysis of RCTs and RCTs combined with case-control study for stone-free rate suggested that PCNL in the supine position was as efficacious as the prone position. Although both positions had the same efficacy, surgeons must bear in mind that the supine position and the prone position had their own advantages and disadvantages. 4
Our pooled analysis and sensitivity analysis for operative time showed PCNL in the supine position is significantly shorter than that in prone position, despite of the varied definition of the operative time in their trials. We thought that these limitations do not jeopardize the validity of the conclusion, because operative time was the only parameter that had statistical significance in the included four studies. In addition, the potential advantages of the supine position over the prone position included: Ease of patient positioning, comfortable posture, and reduced radiation exposure for surgeon posture, ability to perform simultaneous PCNL and ureteroscopic procedures, better control of the airways, dependent Amplatz sheath drainage facilitating the spontaneous evacuation of stone fragments, reducing the pressure of collecting system. 3 –7,10 –13
For complications rate, fever rate and transfusion rate, regardless of pooled analysis or sensitivity analysis, our statistical results showed that the two positions have similar efficacy. Renal access is deemed as the most critical factor for blood loss in PCNL. Some studies demonstrated that the percutaneous tract in the supine position was always through the inferior calix and lower calix, which may lead to more bleeding. 3,14,15 The present meta-analysis for transfusion showed that both groups have similar transfusion rates, which was opposite to the study by Shoma and coworkers. 13
Some studies argued that visceral injuries might occur at a higher risk in the supine approach. In the four included studies, only 1 of 389 patients in the supine position had a colon lesion 12 ; it is the only colonic injury case in published studies. Some studies suggested that only 2% of the patients had a retrorenal colon when in the supine position, whereas the rate increased to 10% when in the prone position. It was the reason that the colon was more anterior in the supine position compared with the prone position. 16,17 These data suggested that independent from the calix and how lateral the puncture is, the PCNL tract in the supine position was safe.
Although the supine position was as safe and efficacious as the prone position, this approach had some disadvantages; for instance, collapse of the collecting system, difficulty in nephroscopy and in approaching the upper calix, and small surgical field for nephroscopy. 18 –22 Some studies demonstrated that PCNL in the prone position had advantages over supine PCNL for obese patients and for patients with staghorn calculi. 23,24 It was a pity that we did not find RCTs and case-control studies for supine and prone positions conducted for those patients.
Although only two single-center RCTs were included in our study, useful information can also be inferred from our study because important confounding factors were recognized and minimized by the statistical methodology of meta-analysis. Because of the small sample and limited methodologic quality of the included studies, it highlights that large scale, multicenter RCTs are needed for a further robust conclusion.
Conclusion
The results of this meta-analysis and systematic review suggested that PCNL in the supine position was as safe and efficacious as the conventional prone position, but there was no overwhelming evidence indicating which is better. The supine position was an alternate option for removal of renal calculi in PCNL. The safety and efficacy of supine position will be better understood once the large multicenter, prospective RCTs are included in the systematic review.
Footnotes
Disclosure Statement
No competing financial interests exist.