
Abstract
Background and Purpose:
Previous studies have demonstrated the feasibility of open radical prostatectomy in the high-risk setting. Management of high-risk disease with robot-assisted laparoscopic radical prostatectomy (RALP) is controversial. We examined biochemical recurrence in a selected cohort of high-risk patients who were undergoing RALP.
Patients and Methods:
Men with high-risk prostate cancer who underwent bilateral nerve-sparing, nonsalvage RALP by a single surgeon without adjuvant or neoadjuvant therapy of any kind were identified. High risk was defined by preoperative prostate-specific antigen (PSA) level >10 ng/dL, Gleason score ≥8 on final pathologic evaluation, or stage ≥pT3. Postoperative PSA value ≥0.2 ng/dL defined biochemical recurrence.
Results:
A total of 73 men were identified. There was no significant difference in surgical margin positivity (38% overall) or prostate size between recurrence and nonrecurrence cohorts. Biochemical failure was significantly associated with higher pathologic Gleason score (P = 0.0085) but not pathologic stage (P = 0.22) or preoperative PSA level (P = 0.18). With follow-up to 85 months (mean 31.8 mos), biochemical recurrence-free survival was 77% with mean time to recurrence of 7.7 months. Recurrence occurred significantly earlier than later (P < 0.001).
Conclusions:
Reasonable short- to intermediate-term biochemical outcomes can be achieved in a recurrence-prone group of high-risk men who are undergoing RALP. RALP is feasible in a selected cohort of high-risk men who are undergoing aggressive local therapy.
Introduction
Without randomized, controlled clinical trials, we are unlikely to find definitive answers to the management of RP in the high-risk setting. Several contemporary studies have demonstrated acceptable long-term oncologic and functional outcomes of open RP in high-risk prostate cancer, however. 4,6 –9 These studies have shown that RP either alone or as part of multimodal therapy (usually with ADT) has an overall survival in the 70% range at 10 years.
None of these studies specifically examined the use of robot-assisted laparoscopic prostatectomy (RALP). Approved by the United States Food and Drug Administration for RP in 2001, use of the Da Vinci radical prostatectomy grew by 30% in 2008 with 73,000 RALPs performed worldwide in 2008. 10 Clearly, there is a need to further characterize the outcomes of RALP, a procedure that now accounts for an estimated two of every three RPs performed in the United States. 10 There is concern about the use of RALP because of lack of tactile feedback, 11 which would be particularly relevant for high-risk prostate cancer. Therefore, we evaluated the feasibility of RALP as primary, unimodal therapy in high-risk prostate cancer patients.
Patients and Methods
From an Institutional Review Board-approved, prospectively maintained database, men with high-risk prostate cancer who underwent RALP from 2002 to 2008 by a single experienced surgeon were identified. We excluded men who received adjuvant or neoadjuvant therapy of any kind. We also excluded men who underwent non–nerve-sparing RALP or salvage RALP. High-risk prostate cancer was defined as a prostate-specific antigen (PSA) level >10 ng/dL, final pathologic Gleason score ≥8, or final pathologic stage ≥pT3. Pathologic staging was used to define high-risk cancer to eliminate bias from downstaging of clinical T3 or higher tumors on final pathologic determination. Clinical staging included serum metabolic chemistries, PSA levels, digital rectal examination, bone scan, and CT of the abdomen and pelvis in most cases.
RALP was performed intraperitoneally with a running vesicourethral anastomotic suture. Bilateral, interfascial nerve-sparing procedures were performed in all patients in this series. Frozen sections were liberally used to verify questionable margins. Limited lymph node dissections were performed bilaterally but were not performed if patients' preoperative risk was low according to established preoperative guidelines. 12 All prostate specimens were serially sectioned and processed at a single facility, with a positive surgical margin defined as cancer at the inked margin. All men were followed locally by the operating surgeon and included a PSA measurement at 3 months postoperatively and subsequently every 3 to 6 months. Additional follow-up information was gleaned from the surgeon records, primary care physician records, hospital records, and telephone inquiries.
SPSS 14.0 was used for all statistical analysis (SPSS Inc, Chicago, IL). Our primary end point was biochemical recurrence, which was defined by a postoperative PSA level ≥0.2 ng/dL. Serum PSA level and age were considered continuous variables. Gleason score was examined as categoric variables Gleason ≤7, 8, 9, and 10, and pathologic stage as categoric variables pT2, pT3a, pT3b, and pT4. The two-tailed t test and Fisher test were used to compare biochemical recurrence vs nonrecurrence cohorts. Chi-square, Wilcoxon test, and Kaplan Meier method were used to analyze time to recurrence and biochemical survival.
Results
A total of 73 men met our inclusion criteria (Table 1). Mean age was 61 years (range 52–74). Racial distribution was 51 (72%) white men, 18 (25%) black men, and 2 (3%) other. Average prostate gland size was 54 g. Overall positive surgical margin rate was 38%, with 58% of men overall having evidence of extracapsular extension on final pathologic determination and 25% with seminal vesicle invasion. Eighty-two percent had multifocal disease and 4% had positive lymph nodes, although lymph node dissections were not uniformly performed on all patients. No intraoperative or postoperative complications were noted.
PSA = prostate-specific antigen.
Characteristics of biochemical recurrence vs nonrecurrence cohorts are listed in Table 2. There was no statistically significant difference in positive surgical margins between the two groups. There was also no significant difference in prostate size, extracapsular extension, seminal vesicle invasion, or tumor multifocality between the two cohorts. Biochemical failure was significantly associated with higher pathologic Gleason score (P = 0.0085) but not pathologic stage (P = 0.22) or preoperative PSA level (P = 0.18). Biochemical recurrence occurred significantly earlier than later (P < 0.001, Fig. 1). With follow-up to 85 months (mean 31.8 mos), biochemical recurrence-free survival was 77% with a mean time to recurrence of 7.7 months.
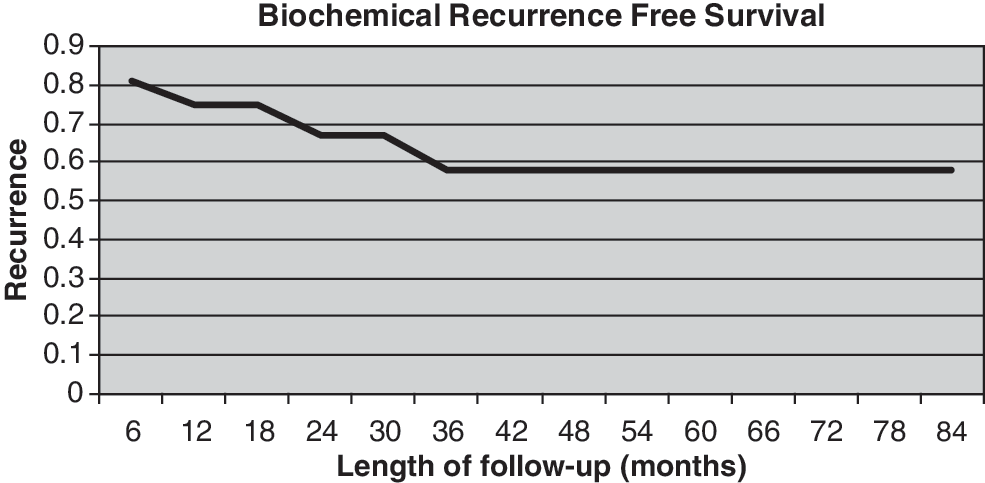
Recurrence-free survival after robot-assisted laparoscopic prostatectomy for high-risk prostate cancer.
PSA = prostate-specific antigen.
Discussion
Despite the lack of definitive evidence for any particular treatment modality in locally advanced prostate cancer, there exists a bias toward nonoperative options. Meng and associates 2 demonstrated through the CaPSURE database that men at high risk were significantly more likely to receive radiation therapy than RP. Similarly, using a Surveillance, Epidemiology, and End Results sample, Denberg and colleagues 1 showed that by 2001, 70% of high-risk prostate cancer patients were receiving aggressive local therapy, but EBRT was 6.5 times more common than RP. Of concern, 23% of men aged <70 years in 2001 had no therapy for local control while only 16% underwent RP. In addition, over the study period from1995 to 2001, RP use declined by half from 18% to 9%. 1
Early studies of RP for locally advanced prostate cancer noted poor outcomes, such as a 29% actuarial cancer-specific survival at 10 years for poorly differentiated cancers in one study encompassing 298 men from 1970 to 1993. 13 This may have influenced the perception that potential cure with RP did not outweigh the side effects of surgery. Several contemporary studies, however, have shown acceptable oncologic outcomes up to 15 years. The Mayo Clinic has long advocated the role of RP in high-risk disease. 14 With a median follow-up of 10.3 years in a group of 842 men with cT3 disease who were treated at Mayo Clinic, Ward and coworkers 6 reported biochemical recurrence-free survival (defined as PSA level ≥0.4 ng/dL), cancer-specific survival, and overall survival of 38%, 79%, and 53% at 15 years. It should be noted that 78% received adjuvant ADT in this study.
Using eight different definitions of high-risk prostate cancer, men treated at Memorial-Sloan Kettering and Baylor with RP alone were found to have freedom from additional therapy ranging from 35% to 76% at 10 years after RP. The 10-year cancer-specific mortality in these cohorts ranged from 3% to 11%. 4 Therefore, aggressive local therapy with RP alone was curative with long-term follow-up for many high-risk prostate cancer patients in this study. Other studies have confirmed these findings. 7 –9 In the series by Loeb and coworkers 9 of 288 high-risk men of whom 75% underwent bilateral nerve-sparing open RP (and of whom 46% underwent RP alone without adjuvant therapy), 10-year actuarial progression-free survival, cancer-specific survival, and overall survival rates were 35%, 88%, and 74%, respectively. 9 Another study that compared 51 clinically advanced men vs 152 clinically localized men undergoing RP by a single experienced surgeon reported 7-year cancer-specific and overall survival rates of 90% and 77% in the advanced group and 99% and 88% in the localized group. The authors concluded technical feasibility of open RP in the setting of clinically advanced disease. 8
In our study, we found an overall biochemical recurrence-free survival rate of 77% at a mean follow-up of 32 months. This is similar to rates reported in the contemporary literature for open RP in the high-risk setting, 7,9 suggesting similar feasibility of RALP in high-risk patients. This is also similar to early results presented recently on 554 high-risk men undergoing RALP. 15 We also found that biochemical recurrence occurred significantly earlier vs later after surgery. This suggests that there may be a window period immediately after RALP during which, if there is no recurrence in the high-risk patient, he may not have recurrence later. While it is impossible to predict the long-term biochemical outcomes of our cohort, others have shown that of all high-risk men in whom relapse occurs, 75% have relapse within 2 years after surgery across eight different definitions of high-risk prostate cancer. 5 Therefore, we can speculate that if a high-risk man in our RALP series did not have recurrence early, he has a reasonable chance to enjoy 10-year survival rates as stated in other series. 5 –9
Our study represents a unique, complete sample set in that all patients underwent RALP with a single experienced surgeon using the same technique with bilateral nerve-sparing procedures in every patient. All pathologic specimens were processed under one protocol, and follow-up was 100%, including all PSA measurements performed with the same assay. Many would consider bilateral nerve-sparing RALP to be a prohibitively “high-risk” procedure in high-risk patients, particularly given the lack of tactile feedback with RALP. 11 We therefore specifically sought out the high-risk men most likely to have recurrence in our database—namely, those who had received bilateral nerve-sparing surgery and had not received any adjuvant or neoadjuvant therapies, such as EBRT or ADT.
Our findings suggest that even in this selected, prone-to-recurrence group, reasonable short- to intermediate-term biochemical recurrence-free survival can be achieved with bilateral nerve-sparing RALP alone. We are not advocating bilateral nerve-sparing RP as a standard procedure in high-risk men but rather show that in our selected series, short-term recurrence rates were similar to contemporary high-risk open RP series, despite bilateral nerve sparing. We have also shown that if men are to experience recurrence, they are more likely to have recurrence very soon in their postoperative course. This has implications for the timing of adjuvant multimodal therapy in that, if a high-risk patient does not have recurrence early in the postoperative period, it may be reasonable to not immediately initiate adjuvant therapy. These findings coincide with other studies in the open prostatectomy literature. 16,17 Finally, our study establishes a baseline cohort for future comparison of high-risk patients undergoing RALP who did not receive any kind of neoadjuvant or adjuvant therapy.
Our findings must be interpreted in the context of the study design. First, our follow-up at a mean of 32 months is relatively short. In other contemporary open RP-only series for high-risk prostate cancer, a sharp drop-off in the first 12 months of biochemical recurrence-free survival is seen with a leveling off out to 60 months. 18 While we cannot say whether RALP and open RP are equivalent in terms of biochemical outcomes for high-risk disease, emerging data report similar 5-year biochemical outcomes of RALP compared with open RP for organ-confined disease. 19 Positive surgical margin rates have also been used as a surrogate outcome measure, and our 38% positive margin rate compares favorably with those reported for open RP in high-risk patients, which range from 38% to 56%. 6,9,20
Another potential limitation is our use of a relatively low PSA level cutoff for high-risk inclusion. The number of patients included as a result of a PSA level >10 was half that of those included because of high-risk pathologic stage or Gleason score, however; those included in the study because of a high PSA level alone comprised just 9% of the cohort (Table 1). This is in accordance to other investigators' findings that in the PSA screening era, the nature of high-risk patients has changed such that Gleason score is more likely and PSA level less likely to determine “high-risk” prior to local therapy. 16,21 Finally, while D'Amico risk categories 22 are the most widely used classification for high-risk prostate cancer, we sought to use a clinically meaningful definition which included pathological data and PSA > 10 ng/dl. Other investigators have suggested that any particular definition of high-risk prostate cancer has little impact on biochemical relapse-free survival variation. 23
Conclusion
Men with high-risk prostate cancer who are undergoing RALP have similar short- to intermediate-term biochemical outcomes and associations to preoperative variables as those previously described for open RP. RALP is feasible in a selected cohort of men who are undergoing aggressive local therapy for high-risk prostate cancer.
Footnotes
Disclosure Statement
Dr. Engel is an investigator for Spectrum Pharma. For Drs. Kao, Hong, and Williams, no competing financial interests exist.