
Abstract
Purpose:
To evaluate the efficacy and safety of simultaneous resection in the treatment of nonmuscle invasive bladder cancer (NMIBC) with benign prostatic hyperplasia (BPH).
Patients and Methods:
Combined published data from comparative studies on simultaneous transurethral resection of bladder tumor/transurethral resection of the prostate (TURBT/TURP) vs TURBT alone in NMIBC were analyzed, considering possible confounding factors. Odds ratios (ORs) and 95% confidence intervals (CIs) were used as the primary effect size to estimate the outcome of overall tumor recurrence, recurrence in bladder neck/prostatic fossa.
Results:
In six eligible clinical trials, 483 patients were treated with simultaneous resection and 500 with TURBT alone. Within the follow-up period, tumor recurrence developed in 203 (42%) patients in the simultaneous resection group and 256 (51.2%) patients in the control group. The combined analysis indicated that the recurrence rate in the simultaneous resection group was statistically significantly lower than in the control group in the overall pooled data (combined OR = 0.67; 95% CI 0.52 to 0.88, P = 0.003). Tumor recurrence of bladder neck/prostatic fossa developed in 37(7.7%) patients in the simultaneous resection group and 42 (8.4%) patients in the control group. No statistically significant difference was found between the two groups (combined OR = 0.92; 95% CI 0.57 to 1.49, P = 0.74). Potential confounders, such as mean age, mean follow-up duration, multiplicity of tumor, and year of publication did not significantly influence the results.
Conclusion:
There was at least the evidence that simultaneous TURBT/TURP did not increase the overall recurrence rate and recurrence rate in bladder neck/prostatic fossa. Simultaneous TURBT/TURP might be preferable for patients with NMIBC and BPH.
Introduction
Some studies have reported that simultaneous resection of bladder tumor and prostate was not preferable. Simultaneous resection was first reported by Kiefer 4 and Hinman 5 based on four and three patients. The results indicated that simultaneous resection was inadvisable because of the high recurrence (100%) in vesical neck or prostatic urethra. Golomb and associates 6 reported 36 patients who underwent simultaneous suprapubic prostatectomy and bladder cancer excision. Recurrence in the vesical neck or prostatic urethra developed in nine (25%) patients. The author recommended separating these two procedures because of the higher recurrence rate in the bladder neck. Subsequently, the in vitro and in vivo studies had similar results. 7,8 The fact that the recurrence occurred often not at the site of previous resection led to the theory of implantation of free floating tumor cells released during the procedures at sites of trauma and implanting on the denuded urothelium. 7,8 Therefore, many urologists avoided simultaneous TURBT/TURP and preferred to perform a separate procedure for each pathologic condition.
Other studies, however, found simultaneous resection was preferable without increasing the risk of tumor recurrence. Greene and colleagues 9 in 1972 reported 100 patients who underwent simultaneous transurethral resection. The result indicated that the recurrence of neoplasm in the prostatic urethra was not causally related to simultaneous transurethral prostatic resection. In recent researches, 10 –17 there were few reports about the deleterious effects of simultaneous TURBT/TURP. Some investigators even thought that earlier resolution of intravesical obstruction not only decreased the recurrence rate, but also had a positive effect on the quality of the patient's life. 17
Was simultaneous resection of bladder tumor and prostate safe and preferable for patients with NMIBC and BPH? The present meta-analysis was conducted to evaluate the efficacy and safety of simultaneous transurethral resection on the treatment of NMIBC with BPH.
Patients and Methods
For the methods of data extraction, statistical analysis, and reporting, the rules and principles of the Cochrane Collaboration Reviews 18 and those published meta-analysis reports on the treatment against NMIBC recurrence were applied as far as was possible and feasible. 19
Literature search
An electronic search of MEDLINE, the Cochrane Central Search Library, Web of Science, Elsevier, Springlink, and EBSCO databases through December 2009 was performed. We retrieved citations using combinations of the medical subject heading search term “simultaneous transurethral resection” and text terms “bladder tumor,” and “prostate.” For MEDLINE, we limited the search to the English language, using the limits function and expanded the search using the related articles function. Additional information was requested from the individual authors by personal contact. Duplicate references, as well as repeated references to the same data sets, were removed. We also performed manual searches of references that were identified in electronically abstracted articles.
All available published data on the simultaneous treatment results in patients with BPH and NMIBC were selected for analysis, provided that all the following data were available: The data source was a controlled clinical trial or a controlled observational cohort study. The study design included the comparison of the efficacy on recurrence, recurrence in the prostatic urethra/bladder neck of both groups. The regimens, as well as the follow-up duration, the mean age of patients, the status of tumor were reported.
Two independent reviewers (SJL and YJL) extracted and interpreted the data according to the analysis protocol. For the final evaluation, six clinical trials were eligible (Table 1). The primary outcomes of this meta-analysis were total recurrence, recurrence in the prostatic urethra/or bladder neck, and recurrence time. The primary exposure was simultaneous transurethral resection. The multiplicity was analysis as covariates in this study. The previous recurrence, tumor size, and postoperative intravesical therapy were not concluded because of lack of data.
Simultaneous group = simultaneous transurethral resection of bladder tumor (TURBT) + transurethral resection of the prostate; control group = TURBT alone.
Study quality assessment adapted from original definition for Cochrane Reviews as A, prospective, randomized, controlled, clinical trials; and B, observational cohort studies or prospective, controlled clinical trials with missing information about randomization. 18
Statistical methods
The meta-analytic procedures used were those described by Yusuf and coworkers.
20
This method is a modification of the Mantel-Haenszel method and is based on a fixed-effects model. Study data are arranged in a 2 × 2 matrix and a summary odds ratio (OR) and its 95% confidence interval (CI) are calculated. The 2 × 2 matrices were constructed in such a way that an OR of greater than 1 indicated a more frequent occurrence of total recurrence, recurrence in the prostatic urethra/bladder neck separately in the simultaneous arm vs the control (TURBT alone
Before estimation of a summary OR, the heterogeneity was evaluated by the Cochran-Q. This procedure tested the hypothesis that the effect sizes were equal in all of the studies. 21 If Q exceeded the upper tail critical value of chi-square (P < 0.05) at κ-1 degrees of freedom (where κ equals the number of studies analyzed or the number of comparisons made), the observed variance in study effect size was significantly greater than that expected by chance if all studies shared a common population effect size. If the hypothesis that the studies were homogeneous was rejected, the studies did not measure the effect of same magnitude. In this instance, calculation of a pooled estimate of effect could be of questionable validity. Study effect sizes could be disaggregated by grouping studies into appropriate categories until Q was not rejected within those categories or regression techniques could be used. Therefore, reasons for the observed heterogeneity must be sought. In essence, Q was a diagnostic tool for determining if all the variance in the observed effect sizes was accounted for.
In addition to an analysis for heterogeneity, sensitivity analyses were used, if necessary. These tests assessed the robustness of the results to specific methods used in the meta-analysis conduct. The potential for publication bias was not statistically examined. Publication bias could occur because published studies were not representative of all studies that had ever been done. The funnel plot method and other statistical adjustments had been constructed in an attempt to address this issue. Unfortunately, these methods lack firm statistical theoretical support and are not generally recommended for medical applications. 18 The following software was used for analysis: Review Manager 5.0, Comprehensive Meta-Analysis, StatsDirect, SPSS, and Excel 2003.
Results
In six eligible 11 –16 clinical trials with a total of 983 patients, the sample size range of the included trials was 48 to 287 patients. In total, 483 patients were treated with simultaneous TURBT/TURP and compared with 500 patients who were treated with TURBT alone. One of these studies was a prospective randomized clinical trial, 15 and five were retrospective observational cohort studies with concurrent groups (Table 1). There was no significant difference in the mean follow-up duration between the simultaneous group and the control group.
Combined recurrence of all studies
Within the follow-up period, tumor recurrence developed in 203 (42%) of 483 simultaneous TURBT/TURP-treated patients and 256 (51.2%) of 500 TURBT alone-treated patients. Studies by Vicente and associates 12 and Hamand colleagues 16 showed the recurrence rate in the simultaneous group was statistically significantly lower than in the control group, while other studies showed no statistically significant difference. In the combined analysis, a statistically significant difference of recurrence rate between two groups was found. The fixed-model combined OR was 0.67 (95% CI 0.52 to 0.88, P = 0.003; Fig. 1). Thus, the overall results of the six eligible studies were consistent with the conclusion that the tumor recurrence of the simultaneous group was statistically significantly lower than in the control group in the overall pooled data.

Tumor recurrence (all studies) with odds ratio as effect size.
Combined recurrence in bladder neck/prostatic fossa of all studies
Within the follow-up period, tumor recurrence developed in the bladder neck/prostatic fossa in 37 (7.7%) of 483 simultaneous TURBT/TURP-treated patients and 42 (8.4%) of 500 TURBT alone-treated patients. In all individual studies and in the combined analysis, there was no statistically significant difference in the recurrence rate in bladder neck/prostatic fossa between two groups. Ham and coworkers 16 reported no recurrence in both groups, and the data were not estimable. The fixed-model combined OR was 0.92 (95% CI 0.57 to 1.49, P = 0.74; Fig. 2). The overall results of the six eligible studies were consistent with the conclusion that there was no statistically significant difference between the two groups on tumor recurrence in the bladder neck/prostatic fossa in the overall pooled data.
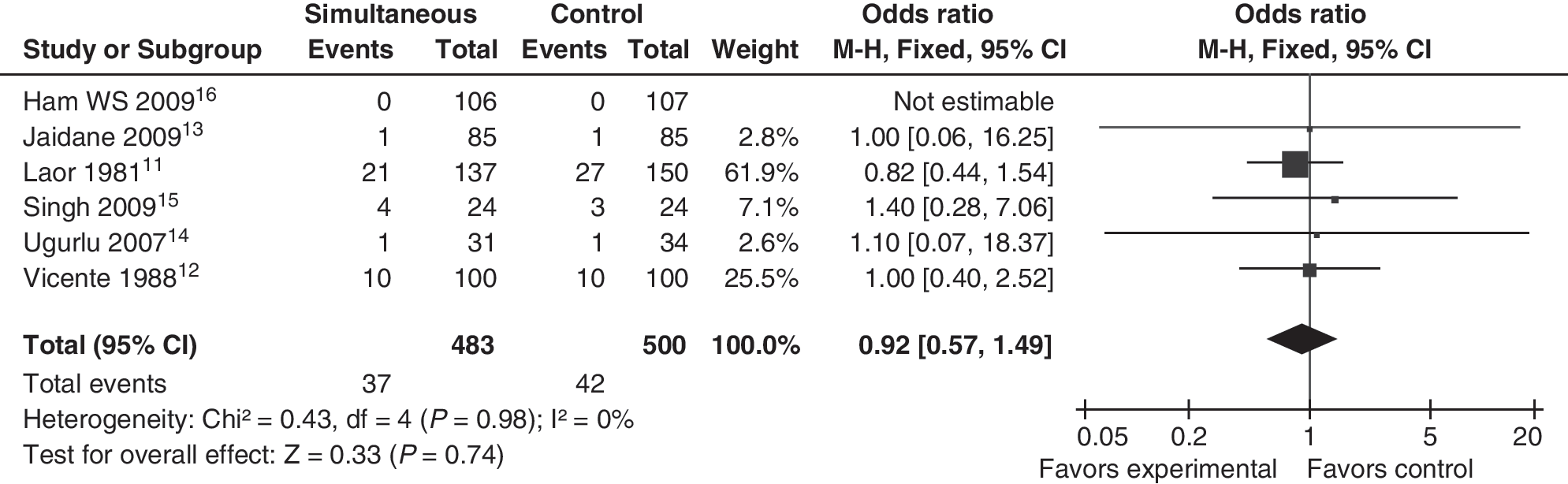
Recurrence in bladder neck/prostatic fossa (all studies) with odds ratio as effect size.
Elapsed time to recurrence
Three of six studies 12,14,15 reported the elapsed time to recurrence (Table 1). The individual analysis showed no statistically significant difference between the two groups. Ham and associates 16 reported that the 60-month recurrence-free probability in the simultaneous group and the control group was 52.0% and 43.4%. The time to recurrence was significantly longer after simultaneous TURBT and TURP (P = 0.021). 16
Potential confounding effects on simultaneous treatment efficacy against tumor recurrence and progression
Clinical and pathologic factors for NMIBC recurrence have been studied extensively over the years. 22 –26 Although studies vary in the number of patients involved, duration of follow-up, variables analyzed, and statistical analysis, the most important variables for prediction of recurrence in patients with NMIBC are multiplicity, previous recurrence rate, and tumor size while CIS, grade 3, and stage T1 for progression. 22 –26 Sylvester and colleagues 22 calculated the probability of recurrence using data from 2596 patients who participated in seven European Organizations for Research and Treatment of Cancer trials. The weighted score was based on six variables (Table 2). 22 The European Association of Urology subsequently adopted this system in its guidelines, and based on these scores, classified patients as low, intermediate, and high risk for recurrence and progression. 2,22
Table reprinted with permission, Elsevier. 22
CIS = carcinoma in situ; WHO = World Health Organization.
The stratified meta-analysis and exact nonparametric statistical tests did not show any statistically significant confounding effects on the results when stratified by mean age, mean follow-up duration, multiplicity of tumor (Table 3), and year of publication (Fig. 3). Previous recurrence rate, tumor size, and postoperative intravesical therapy were not concluded in this study.

Funnel plot of comparison.
Discussion
Many individual trials have low power to detect medically plausible differences between two treatment regimens, especially if both regimens are of valid efficacy. One way to overcome this problem is to perform a combined analysis of available material using meta-analysis techniques. Particularly consistent and strict meta-analytical techniques have been developed, validated, and applied by the Cochrane Collaboration 18 to establish and support the framework of evidence-based medicine. The present study was the first combined analysis concerning simultaneous transurethral resection of bladder tumor and prostate.
The major problem after TURBT is recurrence and progression. The superficial bladder tumors (Ta–T1) are notorious for recurrence (50%–70%) and progression (10%). 27,28 The high recurrence rates of NMIBC can be explained by the multicentricity of the bladder tumors, incomplete excision of the primary tumor, continued exposure to urinary carcinogens, propensity of patients' urinary epithelium to form neoplastic tissue, and/or tumor cell implantation during transurethral resection. 7, 8,10,29,30 Postvoid residual (PVR) urine is related to exposure to carcinogens; early resolution of bladder outlet obstruction (BOO) and lower PVR volume may decrease the exposure to carcinogens and decrease the recurrence rate. 16,17 Otherwise, adjuvant intravesical chemotherapy in patients may have more dwell time in the bladder and prostatic urethra after TURP to decrease further recurrence. Our meta-analysis confirmed that simultaneous TURBT/TURP had decreased the recurrence (42% vs 51.2%).
The concept of urothelial cancer cell implantation was put forth by Albarran and Imbert 31 more than 100 years ago while discussing mechanisms of bladder recurrences after removal of urothelial tumors of the upper urinary tract. Subsequently, in vitro, in vivo studies, and some clinical cases 4 –8 demonstrated that implantation of tumor cells on denuded urothelium is possible and can lead to tumor recurrence. Most of these studies and experiments, however, are open excision. Recent studies and our analysis of simultaneous transurethral resection showed the recurrence rate in bladder neck/prostatic fossa had no statistically significant difference in two groups. The mechanism of this result is complex. One potential is that the relief of BOO may lower the likelihood that residual bladder cancer cells will adhere to the bladder cancer cells and lead to tumor recurrence. 16
There are many risk factors related to recurrence and progression, such as age, initial tumor characteristics, and postoperative intravesical chemotherapy. Most studies we used were not randomized controlled trials; the mean age, mean follow-up duration, multiplicity of tumor, and year of publication did not significantly influence the results. There were, however, some other potential confounding effects, such as tumor size and previous recurrence rate, that could not be eliminated and might cause bias. The evidence from this formal meta-analysis indicated that simultaneous TURBT/TURP had decreased the incidence of overall tumor recurrence and had no effect on the incidence of recurrence in bladder neck/prostatic fossa. Considering the potential confounding effects, we thought that at least simultaneous TURBT/TURP did not increase the recurrence rate at. Multicenter prospective randomized controlled trials would be the ideal way to definitively rule out the influence of simultaneous TURBT/TURP in tumor recurrence and progression, and to estimate the complications and establish the criteria for selecting patients to perform simultaneous resection.
Conclusions
There was at least the evidence that simultaneous TURBT/TURP did not increase the overall recurrence rate and recurrence rate in bladder neck/prostatic fossa. Simultaneous TURBT/TURP might be preferable for patients with NMIBC and BPH.
Footnotes
Disclosure Statement
No competing financial interests exist.