
Abstract
Purpose:
To demonstrate a novel technique of self-cinching anastomosis using a barbed and looped suture during robot-assisted radical prostatectomy (RARP).
Patients and Methods:
This is a feasibility study of 50 consecutive patients who underwent this novel self-cinching anastomotic technique using a V-Loc™ 180 absorbable barbed suture after RARP for clinically localized prostate cancer. The results were then compared with 50 consecutive patients who underwent RARP by the same surgeon before this new technique. We examined whether this novel technique had any effects on posterior reconstruction time, vesicourethral anastomosis time, and thus total reconstruction and operative time by inference.
Results:
The V-Loc 180 group had significantly shorter posterior reconstruction (40 seconds vs 60 seconds; P = < 0.001) and vesicourethral anastomotic times (7 min vs 12 min; P = < 0.001). By inference, this meant that total reconstruction and operative times were also significantly less (8 minutes vs 13.5 min; P = < 0.001 and 106 min vs 114.5 minutes; P = < 0.001, respectively).
Conclusion:
We have shown that this technique is feasible and improves posterior reconstruction and anastomotic times. Further follow-up will determine any benefits of this technique on anastomotic urinary leak rates, continence, and catheter removal times.
Introduction
These factors all contribute to the potential for suboptimal anastomosis, which can result in devastating consequences, including acute urinary leak, ileus, elevated creatinine level, other electrolyte imbalances, prolonged catheterization, prolonged hospitalization, and even long-term incontinence. An anastomotic technique that is highly dependable and technically simple would therefore be welcome.
Recently, we were introduced to a new barbed suture by our plastic surgical colleagues who use its novel design to minimize inflammation and maximize secured and tension-free tissue approximation. 8 –10 Our technique of self-cinching anastomosis is based on the use of this novel suture. In this feasibility study, we present our initial results with this technique.
Patients and Methods
Patient cohort
This is a prospective cohort study of 50 consecutive patients (study group) who underwent this novel self-cinching anastomotic technique using a V-Loc™ 180 absorbable barbed suture (Covidien, Norwalk, CT) after RARP for clinically localized prostate cancer from March to April 2010. Under a protocol that was reviewed and approved by the Institutional Review Board, clinicopathologic outcomes data were collected and entered into a password-protected Microsoft® Access database (Microsoft Corp, Redmond, WA). All 50 patients had cystography to evaluate for urinary leak before catheter removal on postoperative day 5 to 7. The results were then compared with those of 50 consecutive patients (control group) who underwent RARP by the same surgeon before this new technique.
The control group patients underwent total anatomic reconstruction 6,11 that involved posterior reconstruction 3,6,12 using a single looped suture, a vesicourethral anastomosis using two poliglecaprone 25 3-0 sutures tied at the back end, 1 and anterior reconstruction as described previously. 13 The study group also underwent the same reconstruction as the control group, the only difference being the use of the V-Loc 180 absorbable barbed suture instead of poliglecaprone 25. Bladder neck reconstruction is not routinely performed in our unit, and 3/50 patients in the study group had it performed compared with 2/50 in the control group (not significantly different; P = 0.620).
Suture material
For the purpose of this study, we used two 6-inch 3-0 commercially available V-Loc 180 barbed sutures. The V-Loc 180 absorbable wound closure device is prepared from a copolymer of glycolic acid and trimethylene carbonate and consists of a barbed absorbable thread armed with a surgical needle at one end and a loop end effector at the other (Figs. 1a, 1b). The suture has tensile strength of 80% after 7 days, 75% after 14 days, and 65% after 21 days. It is fully absorbed by 180 days. The distance between the barbs, which are unidirectional, is 0.025 inch (40 barbs per inch). The barb and loop end effector design allow for tissue approximation without the need to tie surgical knots except when the two sutures are tied together at the end of the reconstruction. The unidirectional barbs prohibit suture slippage and also evenly distribute tissue forces at several barbed points such that tearing and ischemic changes in the suture line are avoided if precise bites are taken.

A 4X microscopic image of the V-Loc 180 barbed suture showing unidirectional barbed absorbable thread
Surgical technique
RARP was performed using our previously described technique. 14 –16 After the radical prostatectomy specimen and pelvic lymph nodes are packed in an Endo Catch™ bag (Covidien, Norwalk, CT), the posterior reconstruction and vesicourethral anastomosis were performed. A 6-inch V-Loc 180 barbed suture is used for the first layer of the posterior reconstruction. The first bite is taken from the rectourethralis muscle 17 –19 starting on the left side (Fig. 2a). The barbed suture is secured with the loop to the urethra, and a second bite is taken from the retrotrigonal layer 20 behind the bladder opening. The next bite is taken from the rectourethralis muscle on the right side. One additional bite is taken on the right side of the retrotrigonal layer (Fig. 2b). The V-Loc 180 suture is lifted anteriorly, with the right needle driver holding the suture close to the tissue. The left needle driver pulls the suture while the right one pushes the tissue distally toward the urethra. With each synchronized pull and push, the bladder is pushed toward the urethral stump (Fig. 3a).

Posterior reconstruction using the V-Loc 180 barbed suture.
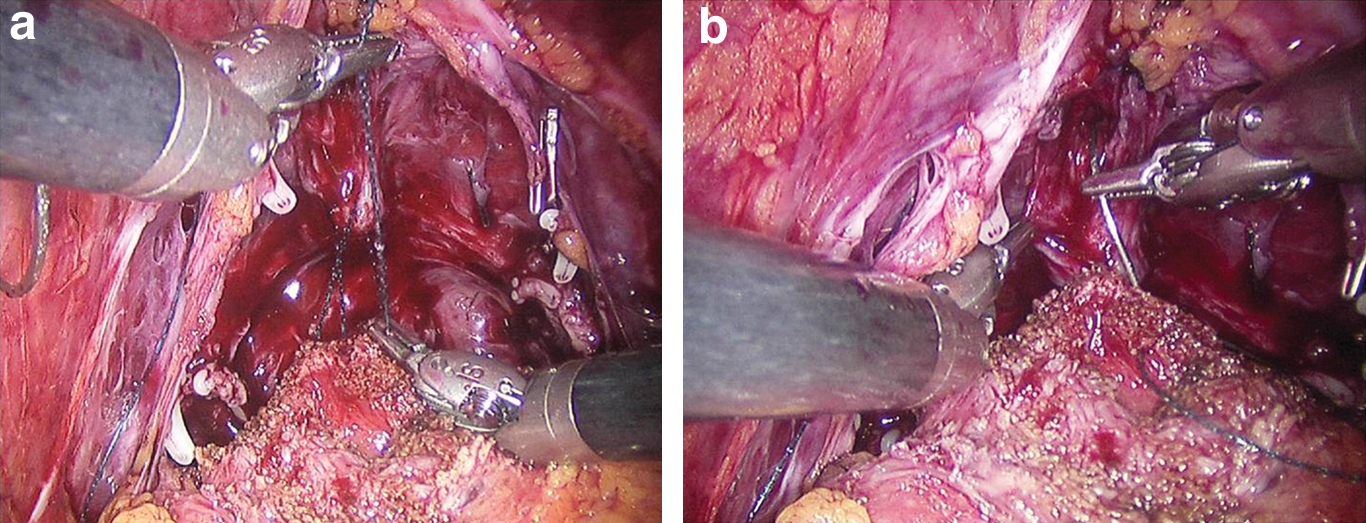
This process is repeated until the tissue is cinched down, and there is no gap between the rectourethralis and retrotrigonal layer. Now the needle is on the right side of the retrotrigonal layer and is introduced into the posterior edges of the bladder on the right side coming outside in. An inside-out bite is then taken through the urethra on the right side and care is taken to include mucosa (Fig. 3b). The outside-in bites on the bladder and the inside-out bites on the urethra are taken moving toward the left side, and the anastomosis is cinched down using the synchronous pull and push technique described above. The V-Loc™ 180 suture the holds the tissue very safely and prevents it from retracting or pulling through. The suture is brought to the anterior side after finishing the entire left wall of the anastomosis (Fig. 4a).
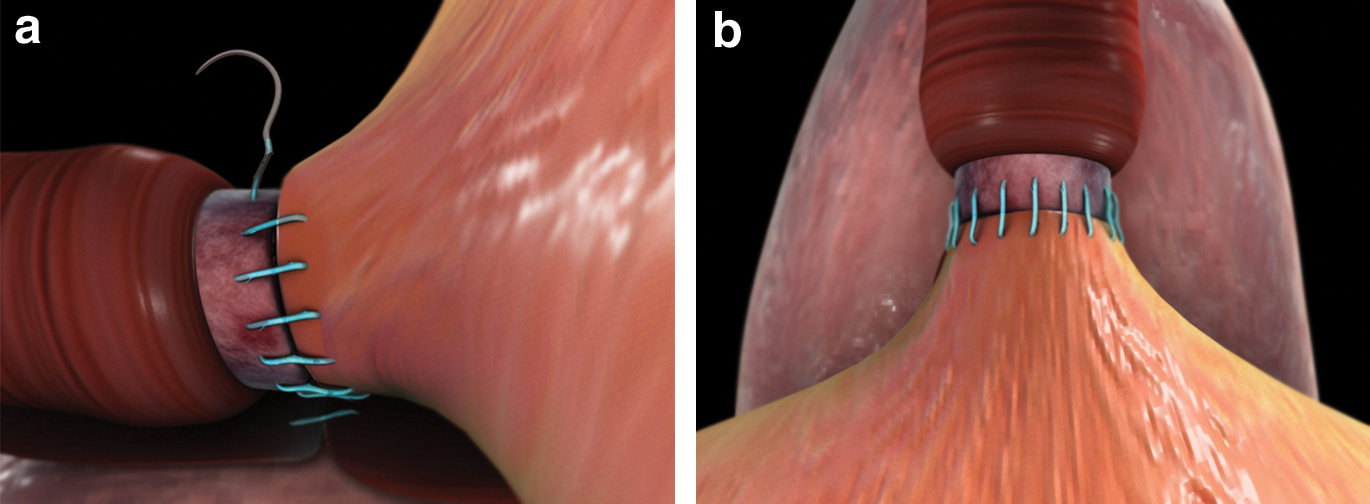
A second V-Loc 180 suture is used for the right side of the bladder. At the end, the right side suture is reversed and the needle is brought out on the bladder side. Again, the synchronous pull and push technique secures the barbed suture and allows the anastomosis to cinch very easily. Care is taken during the anastomosis to incorporate some surrounding tissue to the bladder and urethral mucosa such that if they are thinned, the suture does not tear through. The two V-Loc 180 sutures are then tied to each other (Fig. 4b), and the tail is used to complete the anterior reconstruction by bringing the puboprostatic ligaments and the arcus tendineus toward the edge of the bladder.
Outcomes measurement
We collected data on these 50 patients for standard preoperative and perioperative variables as for our entire patient series of RARP procedures. In this feasibility study, we examined whether this novel technique had any effects on posterior reconstruction time, vesicourethral anastomosis time, and thus total reconstruction and operative time by inference. These operative times were recorded by stopwatch during video playback of all cases. The posterior reconstruction time was measured from the first bite onto the rectourethralis until the first bite onto the bladder. The vesicourethral anastomosis time was measured from the first bite onto the bladder until the two sutures were tied together and cut from the needle.
Statistical analysis
Statistical analysis was performed using PASW version 17.0 (SPSS, Inc, Chicago, IL), with statistical significance considered at P < 0.05. The two groups were compared at baseline for age, body mass index, prostate volume, prostate-specific antigen, biopsy Gleason score, and clinical and radiologic stage. Student t tests were performed to compare the means of the groups and the chi-square and Fisher exact tests were used to compare categoric variables. Posterior reconstruction time, vesicourethral time, and, by inference, total reconstructive and operative times were also measured and the medians of the groups compared with Mann-Whitney U tests.
Results
There was no significant difference in baseline characteristics between our study cohort and our control group (Table 1). There were no suture breakages in either group. The results of comparisons between the study and control groups are shown in Table 2. The V-Loc 180 group had significantly shorter posterior reconstruction (40 seconds vs 60 seconds; P = < 0.001) and vesicourethral anastomosis times (7 min vs 12 min; P = < 0.001). By inference, this meant that total reconstruction and operative times were also significantly less (8 min vs 13.5 min; P = < 0.001 and 106 min vs 114.5 min; P = < 0.001, respectively). There was no significant difference in positive margin rates for all patients (6% vs 4%) and T2 patients (4% vs 2%) between the control and study groups. There were no significant differences in the two patient groups in terms of catheter duration. We routinely remove catheters at 5 to 7 postoperative days, and that was unchanged. One of the patients in the study group re-presented with constipation, and we performed cystography that demonstrated a small urinary leak necessitating delayed catheter removal. The control group did not receive cystography. No patient in either group had postoperative urinary retention.
NS = not significant; BMI = body mass index; N = not applicable; PSA = prostate-specific antigen; IQR = interquartile range; MRI = magnetic resonance imaging.
IQR = interquartile range; EBL = estimated blood loss; NS = not significant; NA = not applicable.
Discussion
RARP remains a technically challenging procedure, and the vesicourethral reconstruction postprostate removal can be problematic. This is a prospective study of 50 consecutive patients who were undergoing RARP by one surgeon (AT) in which a novel technique not previously described in the literature was used. We have shown that this technique has no adverse effect on positive margin rates and that it appears safe, with no clinically significant urinary leaks or urinary retention postoperatively. Of patients in the barbed suture group, 1/50 (2%) had a urinary leak, although it had no clinical impact. We do not routinely perform cystography in our RARP patients, and thus we do not know the cystographic leak rate for the control group patients. Hence, we did not use cystographic evidence to alter the time to catheter removal in the study cohort. A leak rate of 2% in the study cohort compares favorably with the large published contemporary series from Menon and associates 21 (8.6%). We have also shown that the technique is feasible and improves surgical times by more than 40% in our hands. Given this significant reduction at our institute, we postulate that its impact on reducing operative times will be even greater for surgeons earlier in their robotic experience.
We recognize that patient numbers in this study are small and that the results relate only to intraoperative and short-term postoperative variables. Our follow-up is not yet long enough to report continence, erectile function, and other clinical outcomes, and thus this report is a feasibility study. We are also aware of another suture, the QuillTM SRS (Angiotech Pharmaceuticals, Vancouver, BC), which has been used in a very preliminary setting for vesicourethral anastomosis during RARP. 22 This suture has bidirectional barbs, and we are currently performing a randomized controlled trial with three arms: (1) Conventional (poliglecaprone 25); (2) unidirectional barbed (V-Loc); (3) bidirectional barbed (Quill SRSTM). This study will evaluate whether the improved surgical times and operative safety translate into improved patient outcomes in terms of continence, erectile function, catheter removal times, and oncologic results. It may also be speculated that the barbed nature of the suture causes a greater degree of inflammation of adjacent tissue than the conventional sutures. This has not been shown to be the case in the plastic surgical literature, most likely as a result of an improved quality, secured, tension-free anastomosis, 10 –12 and we are currently investigating this in animal models.
One potential drawback of the use of this suture is that it is not easily withdrawn back through the tissues, and thus the suture may need to be cut for removal. This is less of a problem for the posterior reconstruction than for the vesicourethral anastomosis, which takes longer to perform, and given that the main advantage of the barbed suture is in bringing the bladder and urethra together nicely, it might be that its use for posterior reconstruction alone is enough. In any case, in our experience with this suture, it can easily be withdrawn if only one or two bites have been taken; else, it can be cut and a new suture thrown tied to the first suture. We have not found that the barbed nature of the suture makes withdrawing significantly more tricky than with the conventional poliglecaprone 25 suture.
Conclusion
The self-cinching technique with the V-Loc 180 suture allows for a secure anastomosis without the need to tie knots except when the two sutures are tied together at the end of the reconstruction. Its unidirectional barbs precisely grasp the tissue at numerous points, distributing tension throughout the anastomosis. This is an intuitive and easy to use technique for anastomosis that significantly improves operative times even in already expert hands. Further studies will determine if this translates into improved clinical outcomes.
Footnotes
Disclosure Statement
Ashutosh Tewari discloses that he has received research grants from Intuitive Surgical, Prostate Cancer Foundation, and NIH. He is also the endowed Ronald P. Lynch Professor of Urologic Oncology. No competing financial interests exist for the other authors.