
Abstract
Background and Purpose:
Several different methods of teaching laparoscopic skills have been advocated, with virtual reality surgical simulation (VRSS) being the most popular. Its effectiveness in improving surgical performance is not a consensus yet, however. The purpose of this study was to determine whether practicing surgical skills in a virtual reality simulator results in improved surgical performance.
Materials and Methods:
Fifteen medical students recruited for the study were divided into three groups. Group I (control) did not receive any VRSS training. For 10 weeks, group II trained basic laparoscopic skills (camera handling, cutting skill, peg transfer skill, and clipping skill) in a VRSS laparoscopic skills simulator. Group III practiced the same skills and, in addition, performed a simulated cholecystectomy. All students then performed a cholecystectomy in a swine model. Their performance was reviewed by two experienced surgeons. The following parameters were evaluated: Gallbladder pedicle dissection time, clipping time, time for cutting the pedicle, gallbladder removal time, total procedure time, and blood loss.
Results:
With practice, there was improvement in most of the evaluated parameters by each of the individuals. There were no statistical differences in any of evaluated parameters between those who did and did not undergo VRSS training, however.
Conclusion:
VRSS training is assumed to be an effective tool for learning and practicing laparoscopic skills. In this study, we could not demonstrate that VRSS training resulted in improved surgical performance. It may be useful, however, in familiarizing surgeons with laparoscopic surgery. More effective methods of teaching laparoscopic skills should be evaluated to help in improving surgical performance.
Introduction
The Box Trainer (Simulations Trainer, Germany) is one method used for teaching minimally invasive surgical skills. Manipulation of inanimate objects using laparoscopic instruments in a self-illuminated box replicates the principal maneuvers used in live surgery. To increase the realism and efficiency of the learning process, “virtual” anatomic images could be incorporated. With the development of advanced computer programs, the first virtual reality surgical simulator (VRSS) was created, similar to the flight simulators implemented in the training of pilots. 4,5
VRSS provides a novel method of training in laparoscopic skills, without the ethical and financial issues associated with the use of human cadavers or animal models. Other advantages include a means to perform basic to more complex skills without any limitation on the number of repetitions and the ability to record each session for performance analysis. It has disadvantages as well, including the high start-up costs, the need for purchasing ongoing upgrades, the lack of tactile feedback (haptics), and the artificial representation of tissue deformity using computer-generated algorithms with poor fidelity. 6
Preliminary studies suggested that the training of inexperienced surgeons with the VRSS resulted in rapid learning of laparoscopic skills and improved surgical performance when exposed to the real clinical environment. 7 –10 More recent studies, however, demonstrated discordant results. 11,12 Consequently, the role of VRSS in surgical training remained debatable. The purpose of this study was to determine whether practicing surgical skills in a VRSS results in improved surgical performance.
Materials and Methods
Fifteen medical students (from the first to the fourth year) at the University of São Paulo Medical School, with no previous experience in laparoscopy, were recruited for the study. Informed consents were obtained. The participants were randomly divided into three groups, each composed of five students. The first group (control) received no training. The second group received training with the virtual reality surgical simulator LapVRTM (Immersion Medical, San Jose, CA).
The training consisted of performing the following basic laparoscopic skills: Camera manipulation, cutting, peg transfer, and clipping. For each skill, there were three levels of difficulty. During each training session, all tasks were performed at each level of difficulty. The length of the training was 10 weeks, with each weekly session lasting 2 hours each. Based on the literature, this regimen allowed all students adequate time to achieve maximal learning, as measured by a plateau in their learning curve. 13,14
The third group received the same training as those in group II, but, in addition, performed weekly a “virtual reality” cholecystectomy created by the simulator.
After completing the training course, all participants were asked to perform a cholecystectomy in a swine model. To insure uniformity, all participants were assisted by the same surgeon, who placed the trocars, provided explanations, and controlled the camera during the procedure. The procedures were digitally recorded. The estimated blood loss (EBL) for each procedure was based on the volume of blood in the suction system (no irrigation was used during the procedure).
Surgical performance was evaluated based on analysis of the recorded videos. Quantitative assessment included the total surgical time and the time needed to perform each step of the operation: 1) isolation of the cystic artery and cystic duct; 2) clipping the pedicle of the gallbladder; 3) division of the pedicle; and 4) releasing the gallbladder from the liver. Qualitative assessment was based on a scoring system that was developed by Vassiliou and associates. 15 This scoring system consists of a 5-item global rating scale that evaluates depth perception, bimanual dexterity, efficiency, tissue handling, and autonomy (Table 1), and an 8-item task-specific checklist for the dissection of the gallbladder from the liver (Table 2). A higher score correlates with better performance. Scoring of surgical performance was performed by two experienced laparoscopic surgeons blinded to the participants' training history. The overall score for each participant was taken as the average. Statistical analysis was performed using a Kruskal-Wallis test, with 95% confidence interval.
2 = midterm between grades 1 to 3; 4 = midterm between grades 3 to 5.
Results
The average times for each step of the procedure, total surgical time, and total surgical time excluding the gallbladder removal step are summarized in Figures 1 and 2. The average EBL for each of the groups are shown in Figure 3. There was no observed statistical correlation between any of quantitative parameters measured and the amount of training on the VRSS simulator (all P > 0.05). The average scores for each group in the assessment of depth perception, bimanual dexterity, efficiency, tissue handling, autonomy, and dissection of the gallbladder from the liver bed are shown in Figure 4. Again, there was no observed statistical correlation between any of qualitative parameters that were measured and the amount of training on the VRSS simulator (all P > 0.05).
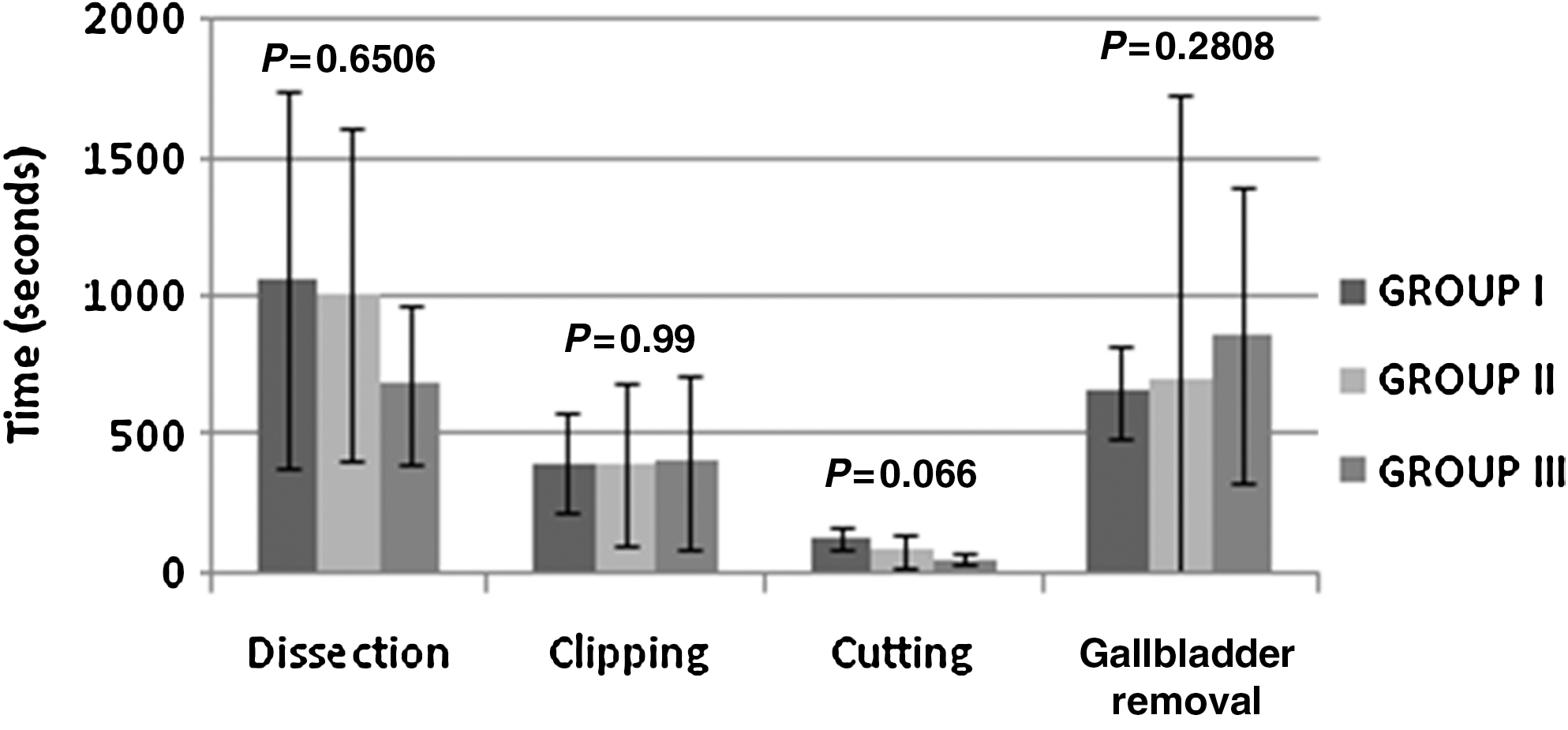
The average time to perform each step.
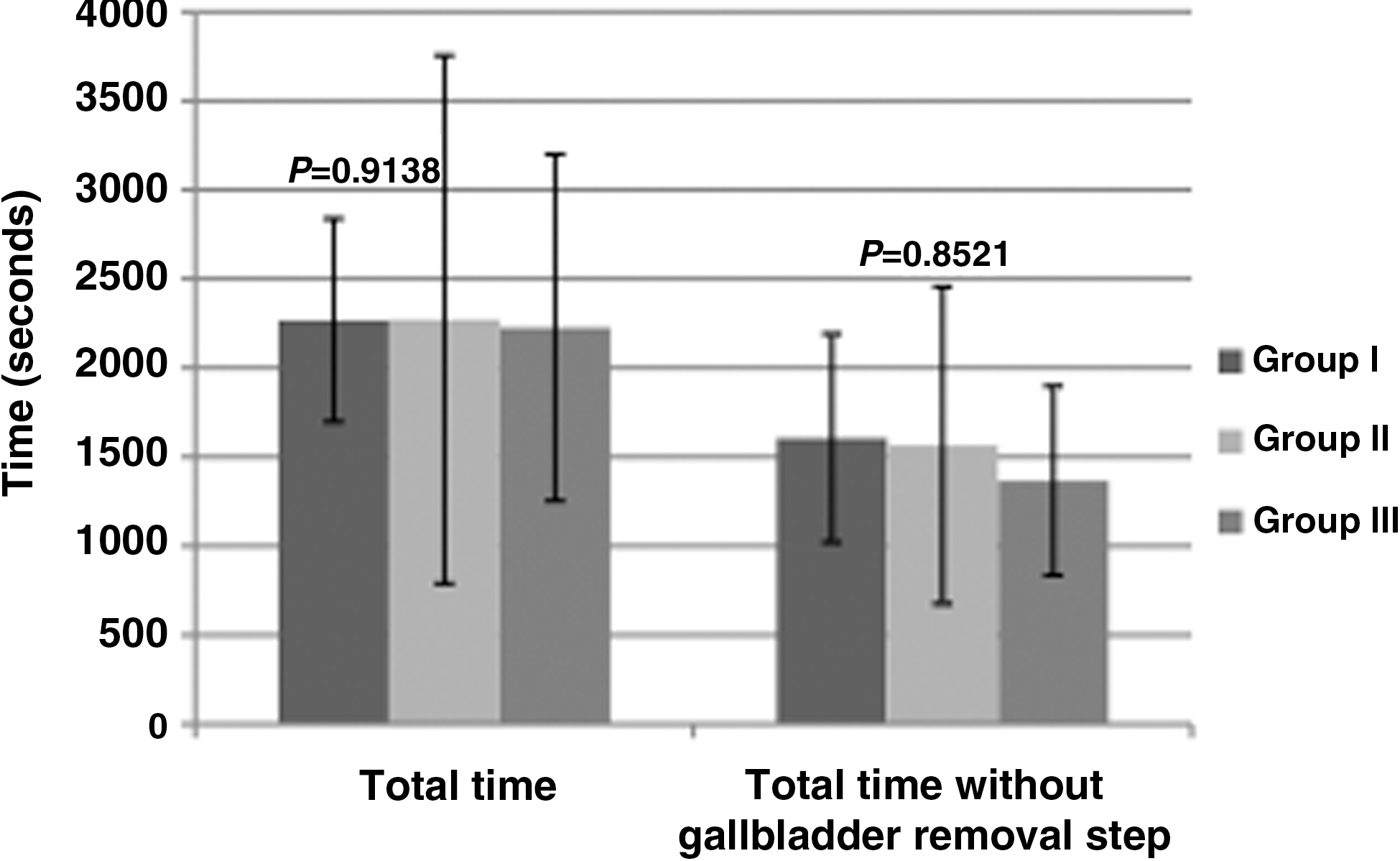
Total surgical time and total surgical time excluding the gallbladder removal step.

Estimated blood loss.
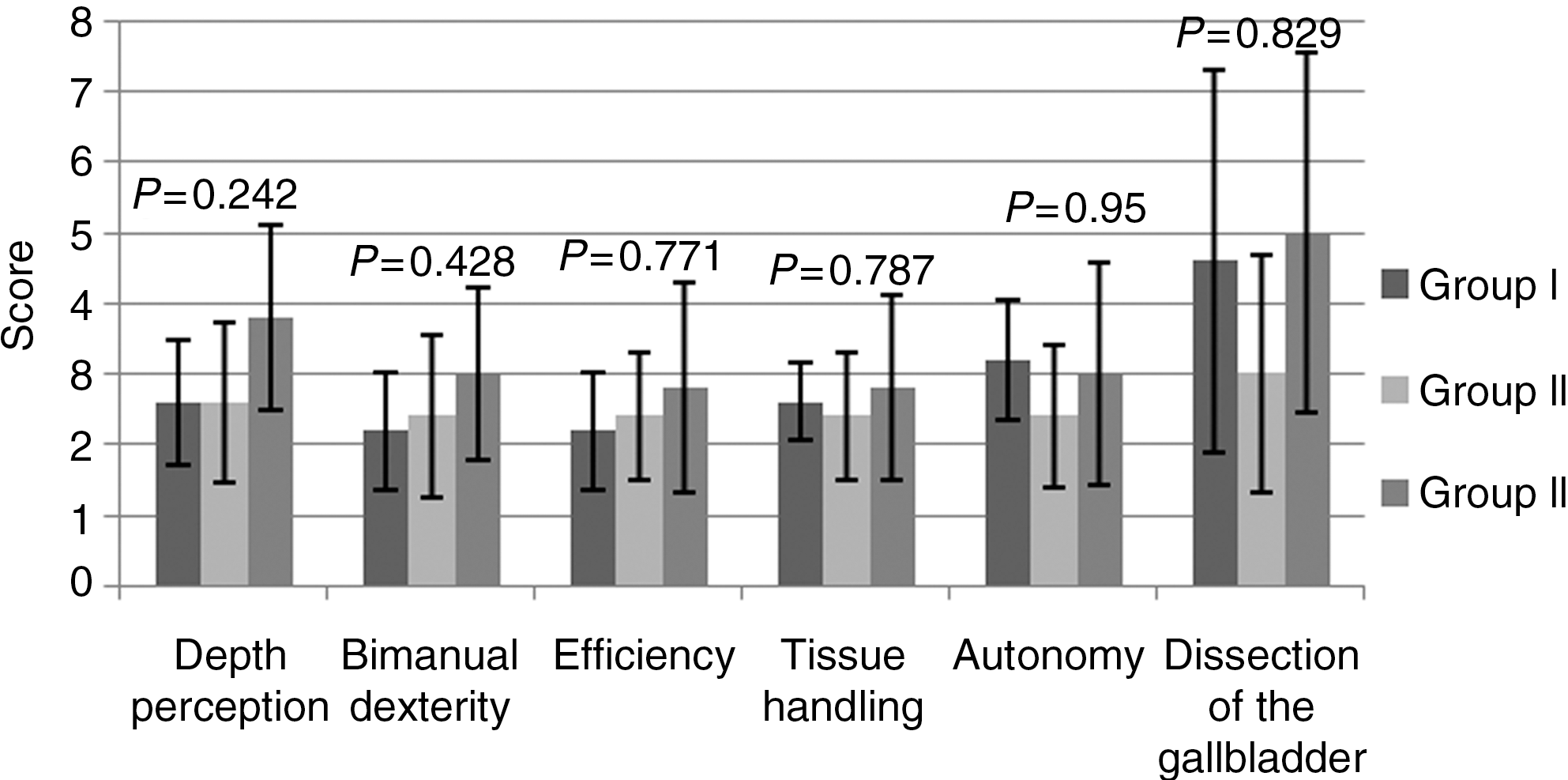
Qualitative assessment of surgical performance.
Discussion
Acquiring laparoscopic skills is a lengthy, arduous, and often expensive process. In theory, the use of virtual reality simulators can significantly reduce the time, manpower, and cost that are associated with teaching laparoscopic skills. Simulators can recapitulate surgical environment, allowing trainees to be familiarized with specific procedures before performing them on patients. Performance can be measured and immediate feedback be given without the need of an experienced teacher present during each step of the instruction. 11 Simulators can be available at any time, allowing for convenient, unlimited practice. 16 Compared with the use of animal models or cadavers for surgical training, VRSS is less expensive and does not have any associated ethical concerns.
Does proficiency on the VRSS translate to improved surgical performance? Previous studies had demonstrated that VRSS can be used to discriminate novices from experts and may play an important role in familiarizing novice trainees with laparoscopic skills. 17 –19 A recent systematic review of the literature by Gurusamy and colleagues 20 indicated that in trainees without surgical experience, VRSS training decreased the time that was taken to complete a task, increased accuracy, and decreased errors compared with no training. In trainees with limited laparoscopic experience, VRSS training resulted in a greater reduction in operating time, error, and unnecessary movements than standard laparoscopic training. The authors also noted, however, that most of the reviewed studies only compared training using skills with different levels of difficulty or basic skills training with and without the addition of more advance skills, such as knot tying. Only a few studies compared different types of VRSS training, and no study has compared basic skill training with and without the addition of simulated procedures, such as cholecystectomies. More importantly, the authors noted that in most of the studies, assessment of skill transfer from training to surgical performance was performed using an unvalidated tool.
In this study, we did not observe any positive association between surgical performance and training with the VRSS. Based on previous studies, 13,14 the length of training was of adequate duration to ensure that a plateau in the learning curve was achieved; yet no differences in surgical performance were observed in those who did and did not have VRSS training. Although we have not found any statistical difference in any of the evaluated parameters between the three groups, two of the six quantitative parameters and three of six qualitative parameters showed a clear linear correlation between amount of training and surgical performance.
This was similarly observed in the systematic review of the literature by Gurusamy and coworkers. 20 In addition, the gallbladder removal step, which was the portion of the procedure less practiced during the training sessions and likely less critical in terms of laparoscopic skills assessment, when excluded from the total surgical time (Fig. 2), also showed a linear correlation between amount of training and surgical performance. Based on these observations, we concluded that the use of VRSS may complement surgical training but cannot substitute for live operating room learning.
We recognized several limitations in this study. The number of participants used in our study may have been insufficient to demonstrate a statistical difference between the three groups. In support of our findings, however, Youngblood and colleagues 21 similarly noted improvement only in two of the seven assessed parameters in medical students who did (n = 17) and did not (n = 13) receive VRSS training. Perhaps increasing our casuistic could empower the study and show larger differences in the trends found, mainly on those portions of the procedure for which training was specifically obtained (notably, cutting skill, which had the most significant difference); nevertheless, the follow-up of a large number of participants would make difficult the accomplishment of the study.
Another potential limitation is the lack of surgical experience in our participants. In the two previous studies that demonstrated a positive correlation between VRSS training and surgical performance, 10,22 surgical residents rather than medical students were evaluated. Thus, it conceivable that the benefits of VRSS are more evident when the participants have some degree of basic surgical training. Further studies will need to incorporate surgical experience as a variable in the analysis.
Finally, in our study, surgical learning was assessed by evaluating the participants' performance in doing one cholecystectomy. Familiarity with working in an animal model could have affected how the participants performed. It is plausible that if the medical students performed additional cholecystectomies, the difference between the groups may be more evident. It should be noted, however, that this would also introduce a confounding variable associated with training/learning on a live animal model. Moreover, the findings obtained using cholecystectomy as a training model may not be necessarily generalized to other procedures, such as nephrectomy.
Conclusion
Laparoscopy training has evolved over time with the addition of several different methods of teaching laparoscopic skills, with VR simulation being the most popular. It assumed to be an effective tool for learning and practicing laparoscopic skills. In this study, however, we did not find that VRSS training improved actual surgical performance, although it may be useful in familiarizing surgeons with laparoscopic surgery. More effective methods of teaching laparoscopic skills that would directly result in improvement of surgical performance should be developed and evaluated.
Footnotes
Acknowledgments
We would like to thank Éder Maxwell Gouveia, Marcelo Junqueira Atanázio, Marina de Paula Andres, Osmar Bianchi da Silva, Pedro Gomes Penteado Rosa, Renato Antunes Schiave Germano, Rogério Heggendorn Sayão Filho, and Simon Benabou for taking the time to train on the VRSS. We also would like thank Débora Anselmo Juliano, Joselito da Silva Estrela, Adrina Sañudo, and the Surgical Technique Discipline of the University of São Paulo Medical School and Prof. Luiz Francisco Poli de Figueiredo for all the support given.
Disclosure Statement
No competing financial interests exist.