
Abstract
Objective:
To avoid unnecessary surgical treatment of small renal masses (≤4 cm), a more accurate diagnostic method would be desirable since radiological differentiation between malignant and benign is difficult and nondiagnostic biopsies account from 9% to 37%. Optical coherence tomography (OCT) measures backscattered light versus depth, with an attenuation coefficient (μ t) that may vary among different histological types. We hypothesize that quantitative measurements of μ t using OCT can differentiate between normal renal parenchyma and renal cell carcinoma (RCC).
Materials and Methods:
Both normal and tumor renal tissues (RCC) were harvested after partial or radical nephrectomy. Analysis of μ t was based on difference of (1) μ t between normal and tumor tissue across all patients and (2) μ t between normal and tumor tissue within individual patients.
Results:
Tissue samples of 18 patients were measured, of which 4 were excluded (urothelial carcinoma, oncocytoma, and benign lesion without normal tissue available). Of the remaining 14 patients, 8 contributed with both normal and RCC tissue and 6 with only normal or RCC tissue. Independent observation showed a significant difference between the median μ t of normal renal tissue (4.95 mm−1) and the median μ t of RCC (8.86 mm−1). No statistically significant difference was found when comparing the difference in μ t between normal renal parenchyma and RCC within individual patients.
Conclusion:
There is a significant difference in μ t between normal and RCC tissue across all patients. These results overpower the lack of significant difference within individuals, encouraging further research and suggesting a possible role for OCT in the diagnostic work-up of renal masses.
Introduction
Optical coherence tomography (OCT) is the optical equivalent of B-mode ultrasonography imaging. Instead of back-reflected sound waves, OCT images are based on back-scattered light. Depth-resolved detection of the back-scattered light results in high-resolution cross-sectional images with a maximal image depth of 1.5 to 2 mm.
The maximal imaging depth is caused by the loss of signal by scattering and absorption of light within the tissue. This attenuation of OCT signal is directly related to the optical properties of the tissue. Consequently, the attenuation coefficient (μ t), describing the decay of detected light intensity with depth, can be quantified using OCT by using Beers law. 8 Recent studies demonstrate that quantitative measurement of μ t using OCT indeed is sensitive for changes of optical properties in tissue, as depicted in analysis of atherosclerotic plaque components, 9,10 as a method to distinguish apoptosis and necrosis in human fibroblasts 11 and in thin optical phantom layers. 12
Because malignant renal tissue displays larger and irregularly shaped nuclei compared with normal tissue, 13 light scattering is expected to be larger, resulting in both changes in morphological appearance in an OCT image and in changes in μ t.
OCT can reveal real-time pathological changes in living kidney of rats both ex vivo 14 and in vivo. 15,16 However, neither of these studies investigated OCT in its ability to distinguish malignant from benign renal tissue in patients with renal cell carcinoma (RCC). Whereas optical spectroscopy has already been evaluated in several studies with promising results in distinguishing benign from malignant renal tumors, 17 –19 until date only one nonpeer review promising report on the field of RCC is available. In that report OCT was able to detect structural abnormalities adjacent to and on the capsule of nine histological confirmed RCCs. 20
To assess the feasibility of OCT we assess in this pilot study the ex vivo ability of OCT to distinguish malignant renal tissue from normal renal parenchyma in patients with RCC based on the attenuation coefficients of these tissue types.
Materials and Methods
Data collection and sample preparation
From March to July 2009 consecutive patients scheduled for nephrectomy (because of tumor or other causes) or partial nephrectomy because of tumor were enrolled in the study. Inclusion was based on informed consent and conjoint availability of the Department of Pathology and of OCT equipment at the Department of Biomedical Engineering and Physics at time of surgery.
Immediately after surgical excision the specimen was transferred to the Pathology Department. There, the specimen was prepared by a pathologist, and, if not compromising the procedures for standard clinical care, a random sample (1–2 cm3) of macroscopic tumor tissue as well as a random sample (1–2 cm3) of macroscopically normal looking renal parenchyma were harvested and preserved in saline. Without any delay the samples were transferred to the Department of Biomedical Engineering and Physics for OCT analysis.
OCT analysis
From each tissue sample, one investigator (D.M.dB.) obtained two or three OCT images, depending on the amount of available tissue (i.e., in total five to six images per patient). The tissue samples were imaged with a commercially available 50 kHz swept source OCT system (Santec Inner Vision 2000; 10 μm axial resolution, 11 μm lateral resolution, with light with a wavelength around 1300 nm). The OCT images were stored to be analyzed at later date. To obtain a quantitative analysis of the OCT images, the decrease of light intensity per millimeter (attenuation coefficient or μ t, in mm−1) of the tissue was determined (Fig. 1) as described before, taking into account the apparatus function 21 and the point spread function 8 of the OCT system. When renal capsula was present in a specimen, the attenuation coefficient was measured below the level of the capsula. When performing the analysis, the investigator was blinded for tissue type and definitive pathology of the tissue samples.

Optical coherence tomography image of a normal renal tissue sample
Statistical analysis
Standard pathological report was considered as the gold standard for comparison. All data were collected in an SPSS 16.0.1. database and analyzed in cooperation with the Biostatistics Department of our clinic. In our analysis we looked at
(1) Difference of attenuation coefficient between normal renal parenchyma and RCC tumor tissue across all patients, treating each tissue sample as an independent observation. The determined μ t are presented as median and interquartile range (IQR).
(2) Difference of attenuation coefficient between normal renal parenchyma and RCC tumor tissue within individual patients, taking possible dependencies between tissues from the same patient into account.
For both analyses, the data were not normally distributed and therefore the Mann–Whitney U test was used in the comparison of normal renal parenchyma with RCC tissue across patients and the Wilcoxon Signed Ranks test in the comparison within the individual patient. For both tests differences were considered statistically significant if the two-sided p-value was <0.05.
Results
In total 26 specimens of 18 patients were measured. Four patients were excluded because of definitive pathological diagnosis of urothelial carcinoma (n = 2), oncocytoma (n = 1), or a benign lesion (n = 1) without suitable normal renal parenchyma to contribute to the control group. From the remaining 14 patients, 8 patients contributed with both tumor (RCC) and normal renal parenchyma. The other 6 patients contributed either with normal renal parenchyma (n = 5) or tumor (RCC) tissue (n = 1). Table 1 describes demographic and pathological data of patients included in the study.
RCC = renal cell carcinoma.
Since more than one OCT image was recorded from each patient, multiple values of μ t were available per patient for both normal and tumor tissue (8 patients), or either normal or tumor tissue (14 patients). We therefore calculated the mean μ t ± standard deviation for each patient and then grouped these values according to the pathology report. In total 59 OCT images were analyzed. The accuracy of individual μ t determinations was derived from the fit statistics. In all cases, the 95% confidence interval on μ t was <1.34 mm−1.
Group comparison: normal tissue versus RCC tissue
We collected 9 cases in the RCC group and 13 in the normal renal parenchyma group. The median μ t of the normal tissue group was 4.95 mm−1 (IQR 4.05–5.68) compared with 8.86 mm−1 (IQR 5.09–11.65) of RCC tissue group (see Fig. 2). A statistically significant difference was seen when comparing the median attenuation coefficient of normal renal parenchyma and of RCC tissue (Mann–Whitney U test, p-value = 0.030).
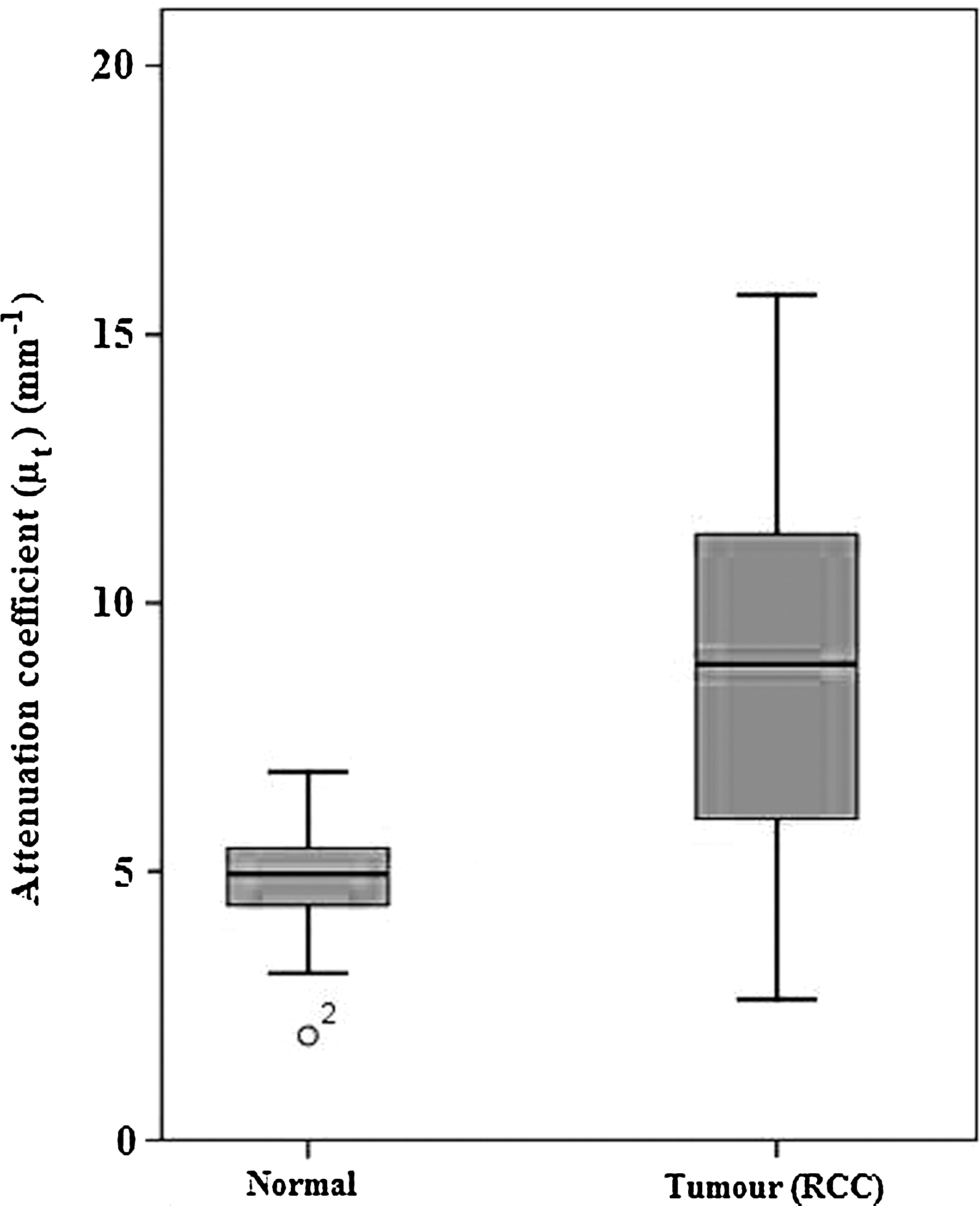
Attenuation coefficient of normal tissue versus tumor (RCC) tissue with one outlier in the normal group. Bars indicate the 95% confidence interval.
Individual patient comparison
Further, in the eight patients with both normal renal parenchyma and RCC tumor tissue, we compared their mean μ t of normal renal parenchyma with their mean μ t of RCC tissue (i.e., patients as their own control). Figure 3 displays the outcomes per patient. No statistically significant difference was found between the mean μ t of normal and RCC tumor tissue (Wilcoxon Signed Ranks Test, p-value = 0.069).
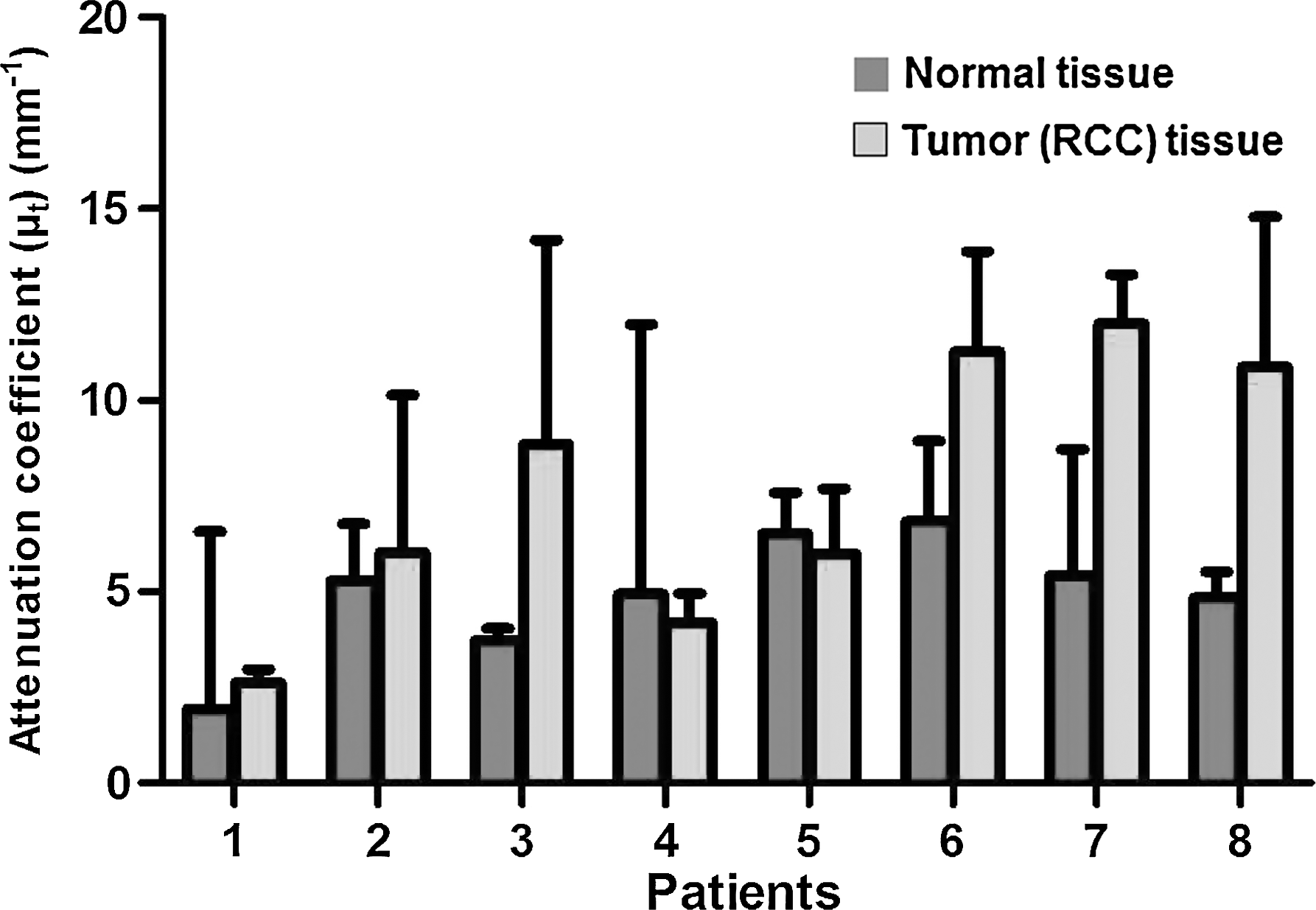
Attenuation coefficients (μ t) of normal and tumor tissue per individual patient. Bars display the 95% confidence interval. Relative large error bars are because of small sample size (n = 2 or n = 3) per patient per tissue type.
Discussion
OCT is a noninvasive imaging technique that allows high-quality, three-dimensional imaging using optical scattering of biological tissues. The technique showed its power in an experimental setting 9 and is currently clinically used in different medical fields as ophthalmology, cardiology, and gastroenterology. 22 –24
The method provides tissue morphology images at micrometer scale resolution representing a noninvasive, real-time, in situ optical biopsy. In urology most of the reports on OCT focus on bladder and prostate carcinomas. In vivo sensitivity and specificity of 97.5% and 97.9%, respectively, have been reported for OCT in combination with fluorescence in the diagnosis of bladder urothelial cell carcinoma. 25 Even though OCT has shown to reveal real-time pathological changes in living kidney of rats, 15,16 to date only one report is available showing OCT was able to detect structural abnormalities adjacent to and on the capsule of nine histological confirmed RCCs. 20
As depicted in Figure 1, the structural information in OCT images can be similar for normal and tumor tissue, which makes diagnosis based on structural appearance challenging. The strength of OCT is that in addition to providing a structural image, quantitative measurements of the optical properties of tissues, such as the amount of light attenuation by scattering and absorption, are feasible. We hypothesized that OCT can distinguish normal from malignant renal tissue based on expected differences in the attenuation coefficient (μ t): the larger and irregularly shaped nuclei that are more abundant in malignant tissue compared with normal renal parenchyma are expected to produce a larger degree of scattering.
Our study shows a significantly higher OCT attenuation coefficient in RCC tissue than in normal renal parenchyma (p = 0.03) when all patients are grouped together (Fig. 2). Others already have shown, using optical reflectance spectroscopy both solely and in combination with fluorescence imaging, 17,18 that the optical reflectance differs between renal tumor tissue and normal renal parenchyma. Further, this difference is also evident when comparing RCCs with oncocytomas, 19 suggesting that optical spectroscopy does distinguish not only between normal and tumor tissue but also between malignant and benign tumors. In the latter study, the optical characteristics of tumor surface were identical to core tumor tissue, suggesting possible application in endoscopic measurements without the need for core biopsies to be performed. 19 However, absolute and highly localized measurements of optical properties are not possible using these techniques. OCT-based techniques such as presented in this and other studies 26 can be the bridge between spectroscopic measurements and our present results.
In our study, RCC tissue showed in six out of eight patients a higher attenuation coefficient than normal renal parenchyma. In the remaining two patients this observation was reversed (see Fig. 3). One of these two patients was known with renal insufficiency and the renal parenchyma corresponded to an end-stage kidney. Indeed, differences in OCT images between normal and ischemic renal parenchyma exist 15 and this may have jeopardized the results in this case as well. Other reasons for the lack of difference may be the scarcity of the sample and the relative heterogeneity of the normal renal parenchyma in this subcohort.
We recognize the limitations of the present study. First, measurements were conducted ex vivo, and therefore tissue perfusion was absent and the specimens were stored in saline. Second uneven samples were used for comparison between nontumor renal parenchyma and RCC tissue and for the in-patient comparison. Although either nontumor and tumor tissue were available in all patients, harvesting of both without potential compromise of the standard pathological assessment was not possible in all cases.
Pilot ex vivo studies as the one hereby presented need to be confirmed and do not always preclude successful clinical results. These preliminary results are the first step in the assessment of OCT as a tool in the diagnostic process of renal mass evaluation and have justified the embarkment of a prospective in vivo study to assess possible OCT differences between normal renal parenchyma and renal tumors, and ultimately differentiation between benign and malignant renal masses.
As statistical difference implies a range, overlap could be expected between normal renal parenchyma and benign and malignant renal tumors. Predictive value of a certain attenuation coefficient, and consequent establishment of cut-offs to distinguish between benign and malignant tissue will be necessary. As far as clinical utilities of OCT are concerned, if results are confirmed in vivo, OCT may be a useful tool in assessing surgical margins after partial nephrectomy and eventually development of ultrathin OCT probes may lead to the replacement of the percutaneous needle biopsy by a percutaneous optical biopsy without the need for puncturing the tumor.
We therefore conclude that ex vivo OCT attenuation coefficients were different between normal renal parenchyma and RCC tissue with RCC tissue showing a significant higher attenuation coefficient when all patients were grouped together per tissue type. Comparison within patients did not show statistically significant differences. However, a larger and homogenous sample might be necessary to lead to definitive conclusions. On the basis of these results we do not reject our hypothesis and we will continue with in vivo OCT analysis and eventually assess the potential of OCT to differentiate between benign and malignant renal tumors.
Footnotes
Disclosure Statement
No competing financial interests exist.