
Abstract
Background and Purpose:
Subclinical rhabdomyolysis (RM) has been reported to occur at a high frequency in patients who are undergoing hand-assisted laparoscopic (HAL) surgery. Compressive forces of the surgeon's hand pushing the patient down onto the operating table may increase the patient's effective weight, a factor that is correlated with risk of RM. The purpose of this study was to evaluate the changes in effective patient weight during pure laparoscopic (PL) and HAL surgery.
Materials and Methods:
Using an in vitro model, 10 subjects performed translocation and knot tying tasks with both PL and HAL techniques. Changes in weight were monitored using a dynamic industrial scale with real-time digital recording. The means of the average changes in effective weight during the different tasks were compared using the Wilcoxon signed rank test with a P value of <0.05 considered significant.
Results:
The mean of the average weight increases during translocation was 2.99 kg with HAL compared with 0.06 kg with PL (Z=4.3, P<0.05). The mean average weight increase during knot tying was 1.28 kg in HAL compared with 0.02 kg (Z=2.6, P<0.05) in PL. The mean maximum weight increase was 8.70 kg and 8.01 kg in HAL compared with 0.43 kg and 0.59 kg in PL during translocation and knot tying tasks, respectively (P<0.05 for each).
Conclusions:
HAL surgery results in a significant increase in effective patient weight compared with PL surgery. This increased effective weight during HAL surgery may increase the risk for subsequent RM.
Introduction
Because postoperative RM occurs secondary to prolonged tissue ischemia from muscle compression and reperfusion injury, 5 transmitted forces from the surgeon to the patient may have a role in the subsequent development of RM. During hand-assisted surgery, the surgeon's hand pushing down for retraction and exposure and the surgeon's arm pushing through the hand-assist device may transmit additional downward force into the patient, thereby increasing the effective weight. Recently, the hand-assisted technique for renal procurement was shown to be associated with a 23% risk of subclinical RM. 6 In addition, the risk of subclinical RM is eight-fold greater with hand-assisted laparoscopic (HAL) surgery compared with pure laparoscopic (PL) surgery. 7 The purpose of this study was to determine the changes in effective patient weight while performing routine surgical tasks using a HAL and PL surgical approach.
Materials and Methods
An in vitro model was constructed to simulate the human abdominal cavity and rectus abdominis fascia (Fig. 1). Three 12-mm laparoscopic trocars (Ethicon Endosurgery, Cincinnati, OH) and a hand-assist device (GelPort, Applied Medical, Irvine, CA) were inserted in a standard configuration to allow surgical tasks using either a PL or HAL approach. The hand access device was placed through an 8-cm incision in the simulated rectus fascia. A dynamic industrial scale (CPWplus 15, Adam Equipment Inc, Danbury, CT) with accuracy within 0.005 kg and digital recording function was placed beneath the simulated abdominal cavity, and effective weight data were recorded continuously (Fig. 1). Effective patient weight change was defined in this study as the weight recorded on the scale after zeroing the scale with the in vitro model, trocars, and hand access device in place.

In-vitro model used for data collection.
Ten participants, with varying degrees of training in laparoscopic surgical techniques, completed an intracorporeal knot tying task and a translocation task using both PL and HAL approaches with the help of an assistant holding the laparoscopic camera for each task. For the translocation task, a series of five beans were grasped with an atraumatic laparoscopic grasper for PL and by the surgeon's hand for HAL and then placed into a receptacle located 15 cm from the simulated abdominal fascia with an opening slightly larger than the bean. Knot tying was performed using two standard laparoscopic needle drivers when performed using a PL approach and one needle driver and the surgeon's nondominant hand when performed using a HAL approach. Each study participant completed both tasks with both PL and HAL techniques.
The mean and maximum average weight change during task completion using PL and HAL approaches were compared using a nonparametric Wilcoxon signed rank test. A Z value of >1.96 (equivalent to P<0.05) was considered to be significant. The percent change in effective weight was also calculated assuming a 70 kg patient and using the formula:
Results
A sample tracing of the measured force transmitted with both translocation and knot-tying tasks with the HAL and PL approaches is shown in Figure 2. The mean average weight increases and mean maximum weight increases with the HAL and PL approaches are shown in Figures 3 and 4.
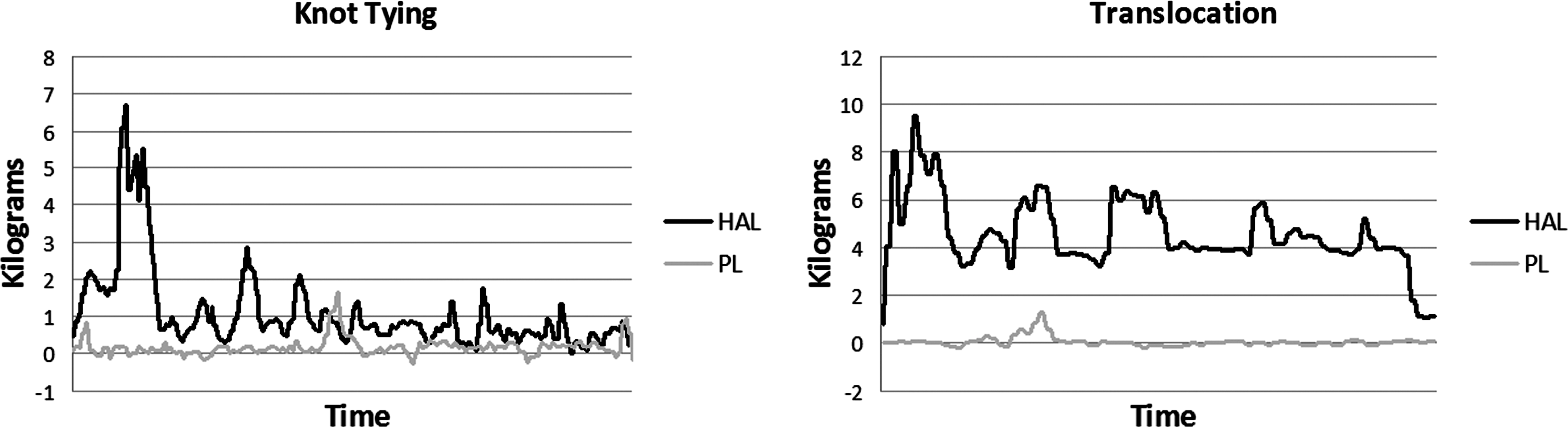
Graphic display of a single participant's data performing knot tying and translocation. HAL=hand-assisted laparoscopic; PL=pure laparoscopic.
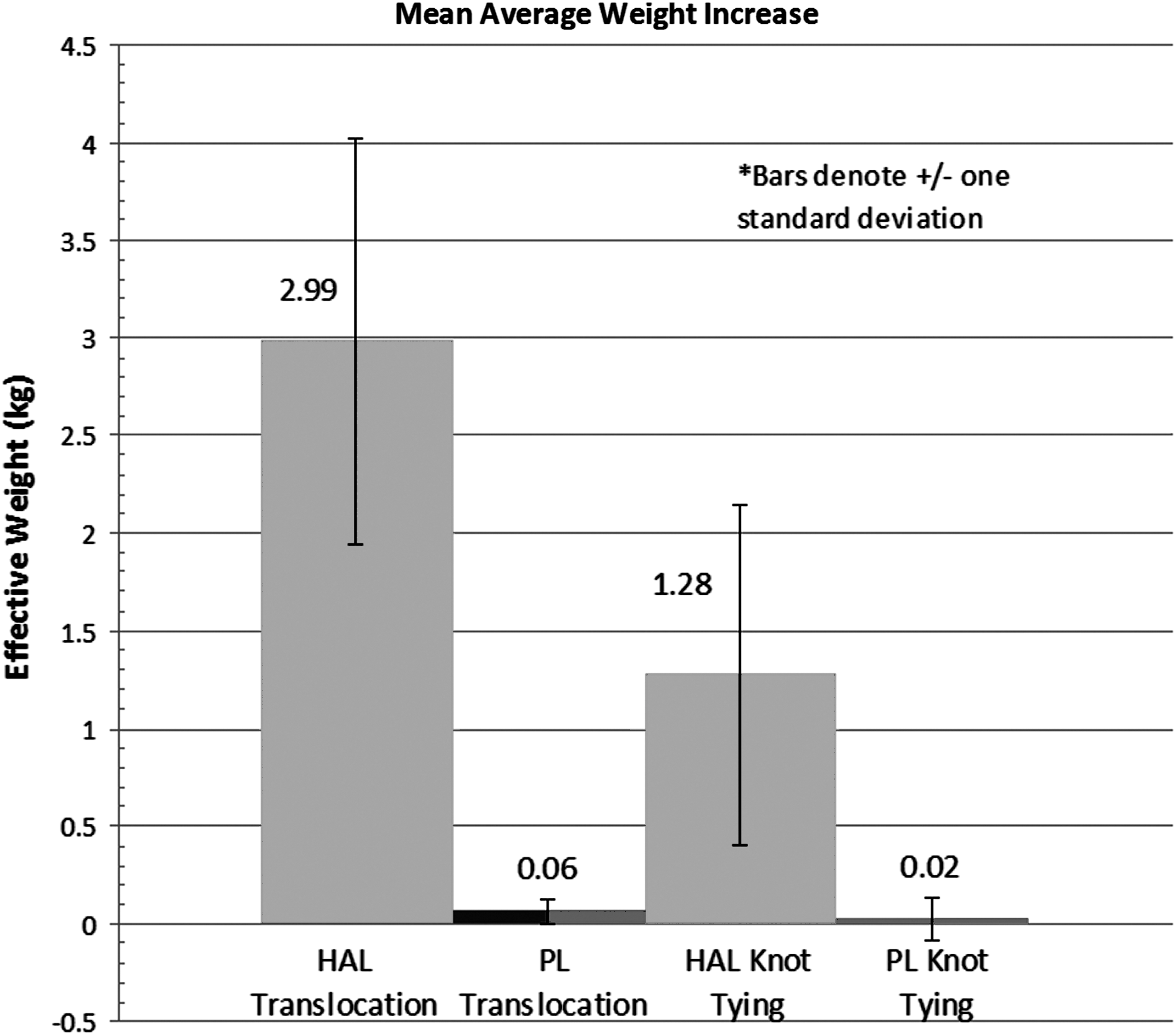
Mean average weight increase of hand-assisted laparoscopic (HAL) translocation vs pure laparoscopic (PL) translocation and HAL knot tying vs PL knot tying.
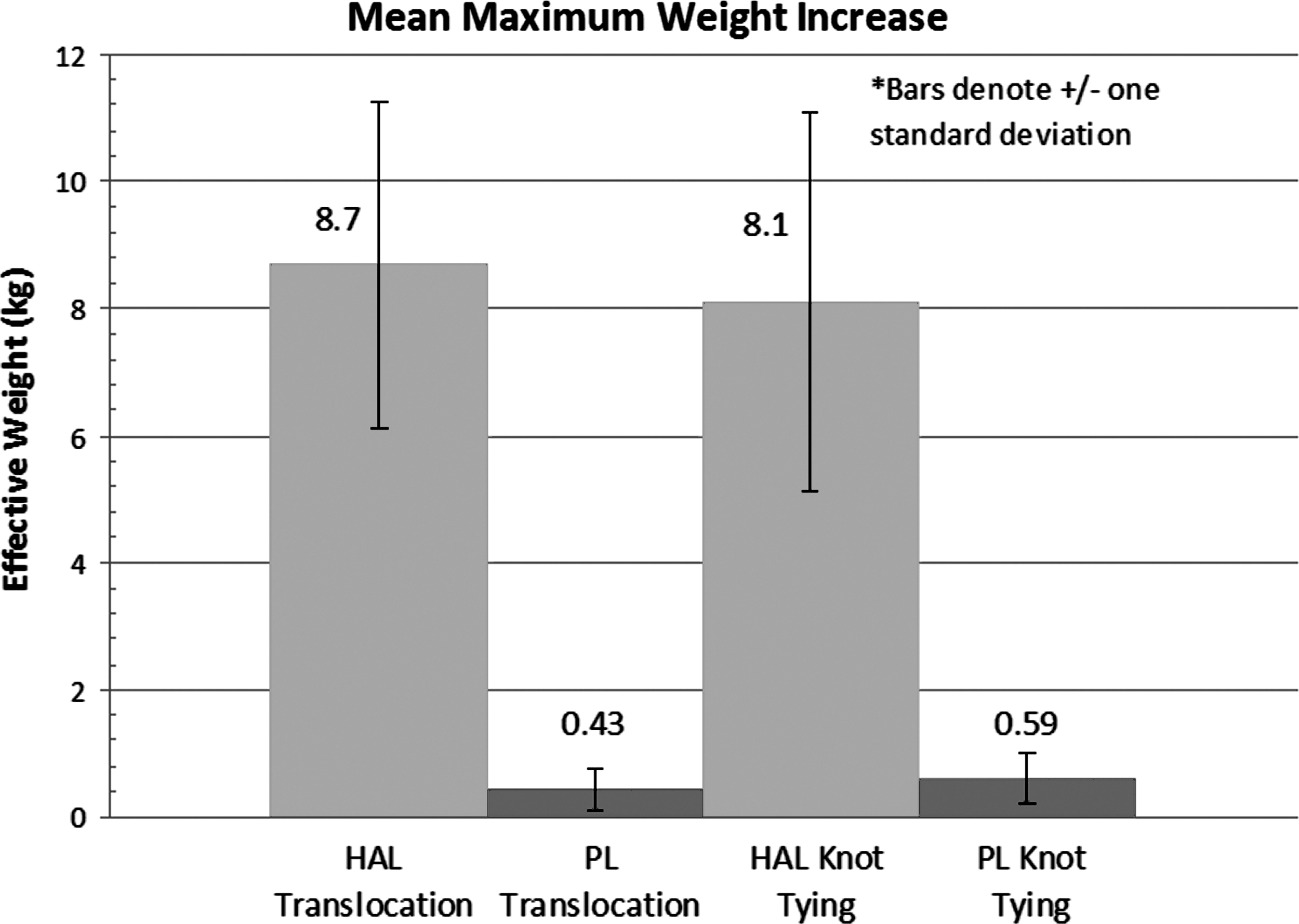
Mean maximum weight increase of hand-assisted laparoscopic (HAL) translocation vs pure laparoscopic (PL) translocation and HAL knot tying vs PL knot tying.
The mean average weight increase with the HAL approach was 2.99 kg (range 1.94–4.46, standard deviation [SD]±1.04) and 1.28 kg (range 0.01–2.88, SD±0.87) compared with 0.06 kg (range −0.01–0.16, SD±0.06) and 0.02 kg (range −0.09–0.18, SD±0.11) with the PL approach during translocation and knot tying tasks, respectively.
The mean maximum weight increase with the HAL approach was 8.70 kg (range 4.89–12.74, SD±2.70) and 8.01 kg (range 5.20–13.46, SD±3.12) compared with 0.43 kg (range 0.18–1.29, SD±0.33) and 0.59 kg (range 0.45–1.67, SD±0.41) with the PL approach during translocation and suturing tasks, respectively. In all weight comparisons, the HAL approach was associated with a statistically significant increase in effective patient weight (Z>2.5, P<0.05).
A 70 kg patient undergoing a HAL procedure would have an increase in effective weight by an average of 4.3% during translocation tasks and 1.8% while knot tying. In addition, the same patient would experience episodic increases in his or her weight by as much as 12.5%. In contrast, the same patient undergoing a PL procedure would experience an average weight increase of only 0.086% during translocation tasks and 0.029% while knot tying.
Discussion
The incidence of clinical (symptomatic) RM after laparoscopic renal surgery has varied greatly, with some centers reporting laparoscopic series with no cases of RM, 8,9 but most series reporting an incidence of between 0.4% to 4.9% of cases. 1,4,10,11 RM in its early subclinical stages may have no symptoms and subsequently be significantly underreported. 6 Postoperative RM after laparoscopic renal surgery has even been reported in completely healthy kidney donors undergoing laparoscopic donor nephrectomy. Kuang and colleagues 2 reported a 32-year-old healthy man who underwent laparoscopic donor nephrectomy, and RM developed. The patient was in a 40- to 60-degree lateral decubitus position with kidney rest elevation for 4 hours 45 minutes, and acute renal failure necessitating dialysis developed. Since then, a number of case reports 3,12,13 and series, 1,4,7,10,11 including a prospective series, have been reported on postoperative RM after laparoscopic renal surgery. 7
Risk factors for the development of RM during laparoscopic nephrectomy may include flexed lateral decubitus position or modified flank position, use of the kidney bridge, and prolonged operative times, which intensify or prolong the compressive forces to dependent soft tissue areas. 1 Other factors, including male sex, high body mass index (BMI), and ethnicity (African American race) have been associated with the development of postoperative elevated creatine kinase (CK) levels, 7 but the underlying mechanisms are not well understood. Deane and colleagues 14 have shown in a bench-top model that there are significantly higher skin-to-operating-table-surface pressures in men compared with women, in those with a BMI ≥25, with a fully flexed surgery position, and with the use of a kidney rest. No previous study has compared the influence of the HAL and PL techniques on patient effective weight.
The etiology of RM in the surgical setting is multifactorial. Compressive forces on soft tissue result in prolonged muscle ischemia followed by reperfusion injury when the compressive forces are removed at the conclusion of the surgery. Subsequent intravascular volume depletion, renal hypoperfusion, and myoglobinuria lead to tubular injury and renal dysfunction. 5 Acute renal failure develops in 4% to 33% of patients with symptomatic RM, with an associated mortality rate of 7% to 50%. 15 Additional complications of RM include metabolic acidosis, disseminated intravascular coagulation, and electrolyte abnormalities. 5
Fifteen years after the first laparoscopic nephrectomy in 1991, 16 88% of all donor nephrectomies were performed laparoscopically, with 30% performed PL and 58% HAL. 17 Patients undergoing HAL have been shown to have a 23% incidence of subclinical RM (postoperative CK elevation >1000 IU/L). 6 Furthermore, the incidence of RM has been shown to be higher in patients undergoing HAL surgery when compared with a PL approach, even when controlling for operative time, age, sex, and other variables known to result in RM. 7 In addition, the risk of subclinical RM was shown to be eight-fold greater with HAL compared with PL. 7
Our study demonstrates a mechanism that may partially explain how HAL surgery may place patients at an increased risk for RM. In comparison with the HAL approach, there was very little force transmitted to the patient during the PL approach. This increased weight provided by the force transmission from the surgeon's hand or arm to the patient during HAL surgery may significantly increase the compressive forces acting at the interface between the table and patient. Increased patient weight and BMI are known to correlate with an increased risk for RM. 18
Many forces are continually acting on a patient and may play a role in determining the effective weight, including the weight of the drapes, surgical instruments, and equipment and cords that are placed on the patient. The surgeon's or assistants' hands that are resting on the patient or additional forces from leaning onto the patient may also increase the effective weight. In particular, with the HAL technique, the insertion of the hand through the hand-assist device causes additional transmitted force to the patient. This may be compounded by a surgeon's attempts to provide a small cosmetically pleasing incision that will necessitate additional force for insertion of the surgeon's hand. Also, as the surgeon reaches further into the abdomen and the larger portions of the arm make contact with the hand-assist device and the patient's fascia, additional force is transmitted to the patient increasing the effective weight. In addition, the increased pressure of the arm in the hand-assist device may make the rectus muscles ischemic and increase the risk for RM. Reduced perfusion pressures as a result of the use of pneumoperitoneum have also been proposed to be a contributing factor to RM 4 but would not explain the differences seen between HAL and PL approaches.
Potential methods to minimize transmitted forces to the patient may include placing trocar sites closer to the kidney, avoiding leaning on the patient, and minimizing placement of instruments on the patient. For the hand-assisted technique, the incision length for the hand-access device may also need to be extended to accommodate surgeons with larger arm circumference.
There are some potential limitations of this study. This is a bench-top study that potentially introduces biases because of the absence of living tissue. It is impossible to control for all factors present in a living system in a bench-top model. In addition, patient size may play a significant role in the amount of force transmitted to the patient. In our study, the working distance from the hand-assist device to the working area was only 15 cm. In a very large patient, the surgeon's arm may have to be inserted much further, and the larger portions of the arm may even further increase the effective weight transmitted to the patient. Furthermore, in larger patients, more force might be needed to complete surgical tasks. Hence, this study may underestimate the forces transmitted in larger patients.
In addition, this study tested only two surgical tasks, while during the course of a surgery there are many other maneuvers that may variably alter the patient's effective weight. Furthermore, this study tested only one hand-assist device. Other devices, not tested in this study, may have different effects on patient effective weight. Despite these limitations, this study demonstrates that hand-assisted surgery may increase a patient's effective weight and represent one risk for RM.
Conclusions
Postoperative RM is a potentially serious complication of laparoscopic renal surgery. HAL surgery significantly increases the effective patient weight compared with PL in an in-vitro model. Efforts to reduce the amount and duration of transmitted forces to the patient may help prevent RM and improve the safety of HAL surgery.
Footnotes
Acknowledgments
Reference 17 was supported in part by Health Resources and Services Administration contract 234-2005-370011C. The content is the responsibility of the authors alone and does not necessarily reflect the views or policies of the Department of Health and Human Services, nor does mention of trade names, commercial products, or organizations imply endorsement by the United States Government.
Disclosure Statement
No competing financial interests exist.