
Abstract
Purpose:
To assess the current indications, perioperative morbidity, and stone-free outcomes for percutaneous nephrolithotomy (PCNL) worldwide.
Patients and Methods:
The Clinical Research Office of the Endourological Society (CROES) collected prospective data for consecutive patients who were treated with PCNL at centers around the world for 1 year. PCNL was performed according to study protocol and local clinical practice guidelines. Stone load and location were recorded, and postoperative complications were graded according to the modified Clavien grading system.
Results:
Between November 2007 and December 2009, 5803 patients were treated at 96 centers in Europe, Asia, North America, South America, and Australia. Staghorn calculus was present in 1466 (27.5%) patients, and 940, 956, and 2603 patients had stones in the upper, interpolar, and lower pole calices, respectively. The majority of procedures (85.5%) were uneventful. Major procedure-related complications included significant bleeding (7.8%), renal pelvis perforation (3.4%), and hydrothorax (1.8%). Blood transfusion was administered in 328 (5.7%) patients, and fever >38.5°C occurred in 10.5% of patients. The distribution of scores in modified Clavien grades was: No complication (79.5%), I (11.1%), II (5.3%), IIIa (2.3%), IIIb (1.3%), IVa (0.3%), IVb (0.2%), or V (0.03%). At follow-up. the 30-day stone-free rate was 75.7%, and 84.5% of patients did not need additional treatment.
Conclusion:
With a high success rate and a low major complication rate, PCNL is an effective and safe technique overall for minimally invasive removal of kidney stones.
Introduction
In addition to surgery, current options for interventional management of renal stones also include ureteroscopy, percutaneous nephrolithotomy (PCNL) and shockwave lithotripsy (SWL). After the first description of the technique in 1976, 4 use of PCNL became initially widespread. With the introduction of SWL in the early 1980s, which gained popularity as a noninvasive, easy-to-use, and effective treatment, use of PCNL diminished. Recent studies have indicated a resurgence in the use of PCNL during the last 10 years, 2,5,6 which can be attributed to two factors. First, awareness of the limitations of SWL has emerged with accumulating clinical experience of this approach. Second, improvements in the PCNL procedure, which continue, have led to reductions in morbidity and yielded stone-free rates of >90% in treated patients. 7,8 Several key factors have been identified that impact treatment outcomes and complication rates with PCNL, including indications for treatment, renal access, and available equipment. Specifically, the introduction of balloon dilation of the tract, use of flexible nephroscopes, improved intracorporeal lithotripters (including ultrasound, pneumatic devices, and the holmium:yttrium-aluminium-garnet laser), and the trend to smaller or no nephrostomy tubes have contributed to increased efficacy of percutaneous stone disintegration and decreases in the overall morbidity rates for PCNL. Such improvements in techniques for percutaneous stone removal have resulted, for example, in significant decreases in transfusion rates, which were 25% in early reports and have decreased to 1% to 2% in more recent studies. 9
PCNL has demonstrated safety and efficacy in the management of large, multiple, or complex renal stones. 10 Other indications are the composition of the stone, the site of the stone, and the existence of obstruction distal to the stone, the certainty for the final result, the failure or the contraindication to SWL, and the presence of renal anatomic variation.
Inherent with the developmental progress of PCNL is an increase in variations of the technique. For example, PCNL has been performed with the patient in various positions, including the conventional prone position, semisupine, flank, supine with a pad under the leg or buttock, and complete supine. Other major variables in the technique include imaging modality, site of kidney puncture, method of tract dilation, size of nephroscopes and tubes, and use of kidney drainage (if any) after PCNL. In addition, while an interventional radiologist has traditionally been needed to acquire renal access for percutaneous renal surgery, increasingly urologists have performed this procedure without the assistance of a radiologist and with similar success. 11,12 There are regional variations in the number of procedures performed by urologists, 13 and training for urologists in techniques to establish a safe and reliable percutaneous access is essential. 1
The Endourological Society, one of the major international urologic societies, was established to facilitate scientific dialogue among endourologists worldwide. Founded during the World Congress of Endourology meeting in 2008, the Clinical Research Office of the Endourological Society (CROES) was established as a unit within the Endourological Society responsible for organizing, structuring, and facilitating a global network for endourologic research. 14 The activities of the CROES thereby support the Endourological Society's overall objective of further advancing the broad knowledge and skills in endourology and related emerging technologies by implementing high quality scientific and clinical research in this field of medicine.
In recognizing the renaissance of PCNL as a primary treatment for patients with renal stones, the CROES initiated the PCNL Global Study to establish a prospective global database for the current indications and outcomes of PCNL. The purpose of the study was to better understand the fundamental differences between clinical institutions around the world in the use of this procedure and to identify specific factors that might influence treatment-related morbidity. In this communication, we report the overall results for indications, complications, and outcomes in more than 5800 patients who were reported by the centers that participated in the CROES PCNL Global Study. This is the first in a series of articles that will be presented from the study.
Patients and Methods
This was a prospective observational study during which data were collected for consecutive patients who were treated at each participating center over a 1-year period.
Study objectives
The primary study objective was to assess the current indications for PCNL treatment and outcomes in terms of the stone-free rate. Secondary study objectives were to assess the perioperative morbidity (30 days) of PCNL by using the modified Clavien grading system and to define risk factors for the development of perioperative morbidity after PCNL.
Study organization
The authors were invited by the CROES council to form a globally representative Steering Committee that was responsible for directing the CROES PCNL Global Study. All were members of the Endourological Society and were selected for the Steering Committee based on their recognition as experts in PCNL treatment. Study sites were eligible to participate in the study if they were considered by the Steering Committee to have high expertise in this medical field. The objective of the Steering Committee was to recruit 100 centers worldwide with an assortment of sites, including smaller centers that treated low numbers of patients as well as larger “higher volume” centers and clinical training centers. Each center was invited to include all patients who were treated consecutively for 1 year, with the study period at each site starting with the treatment of the first included patient.
Inclusion criteria and treatment protocol
Patients who were eligible for inclusion were all those who were candidates for percutaneous surgery as the primary indication or after failure of previous treatment. There were no specific exclusion criteria. Treatment of patients with PCNL was based on the presence of symptoms of pain in the flank, hematuria, fever and/or sepsis, and/or dilatation of the upper urinary tract. For the PCNL procedure, patients were positioned either in the supine or prone position. Access to the upper tract was guided by ultrasonography and/or radiography in combination with (retrograde) intrarenal contrast injection.
Once access was obtained, a guidewire was inserted and preferably maneuvered toward the ureter. Dilation was performed with balloon, telescopic, or serial dilators, and an Amplatz sheath was then positioned. In follow-up, the system was inspected by the rigid nephroscope, and the stones were either disintegrated by laser, ultrasound, or ballistic devices or removed in toto with graspers. The procedure was considered to have been completed when all removable stones had been taken out. Internal and/or external drain(s) were positioned according to the judgment of the surgeon.
Patient follow-up
Postoperative renal assessment was performed by ultrasonography, radiography, or CT based on availability or local clinical practice. Success of treatment was defined as the patient being stone free by 30 days post-treatment. Severity of bleeding was assessed by the treating physician according to clinical judgment and the necessity for blood transfusion based on local clinical practice guidelines. Perioperative complications were assessed and graded according to the modified Clavien system 15 as applied to PCNL. 16
Secondary treatment
Secondary treatment was deemed necessary if there were still significant remnant stones, if remaining stones obstructed the upper urinary tract, or for other reasons, according to the clinical judgment of the treating physician. Secondary treatment that involved repeated PCNL, ureteroscopy, or SWL was selected according to clinical assessment.
Data collection
Data were collected in a central database held at the CROES office. Because the PCNL Global Study was the first project of CROES, the initial design of the database was to examine the support for a global study. Current CROES studies are using a web-based database, available through the website:
Data analysis
The data were analyzed using SPSS version 16.0. All data are descriptive and based on frequencies. The amount of missing values ranges between 0 and 8.1%. Thirty-eight (79.1%) of 48 primary variables in the Global PCNL database that are reported in this article had less than 2.5% absence. The rest had between 2.5% and 8.1% missing values. The mechanisms of absence of the variables were not reported. For calculating the percentages, the missing values have not been included.
Results
Between November 2007 and December 2009, 5803 patients were treated at 96 centers in Europe, Asia, North America, South America, and Australia. This total included 3249 patients at 60 sites in Europe, 1369 patients at 16 sites in Asia, 830 patients at 16 sites in North America, 345 patients at 3 sites in South America, and 10 patients from 1 site in Australia. The number of participating centers per country and number of patients per country are shown in Table 1.
Patient characteristics
Not all of the parameters that were recorded in the database were available for the entire population of 5803. For this reason, percentages are expressed as the percentage of patients for whom data are available. The study population comprised 3263 (56.3%) males and 2532 (43.7%) females. The distribution of patients according to age, body mass index (BMI) and operating time are presented in Figures 1 –3. Approximately one-third of patients had significant comorbid illness, such as diabetes mellitus or cardiovascular disease (Table 2). The majority of patients had an American Society of Anesthesiologists score of 1 or 2. A total of 3072 previous stone treatments had been undertaken (PCNL, SWL, pyelolithotomy, or ureteroscopy; Table 2). In 437 (7.7%) patients, a percutaneous drain had been placed before PCNL. In 887 (15.9%) patients, a positive urine culture was found at workup, and in 5541 (96.5%) cases, antibiotic prophylaxis was prescribed.
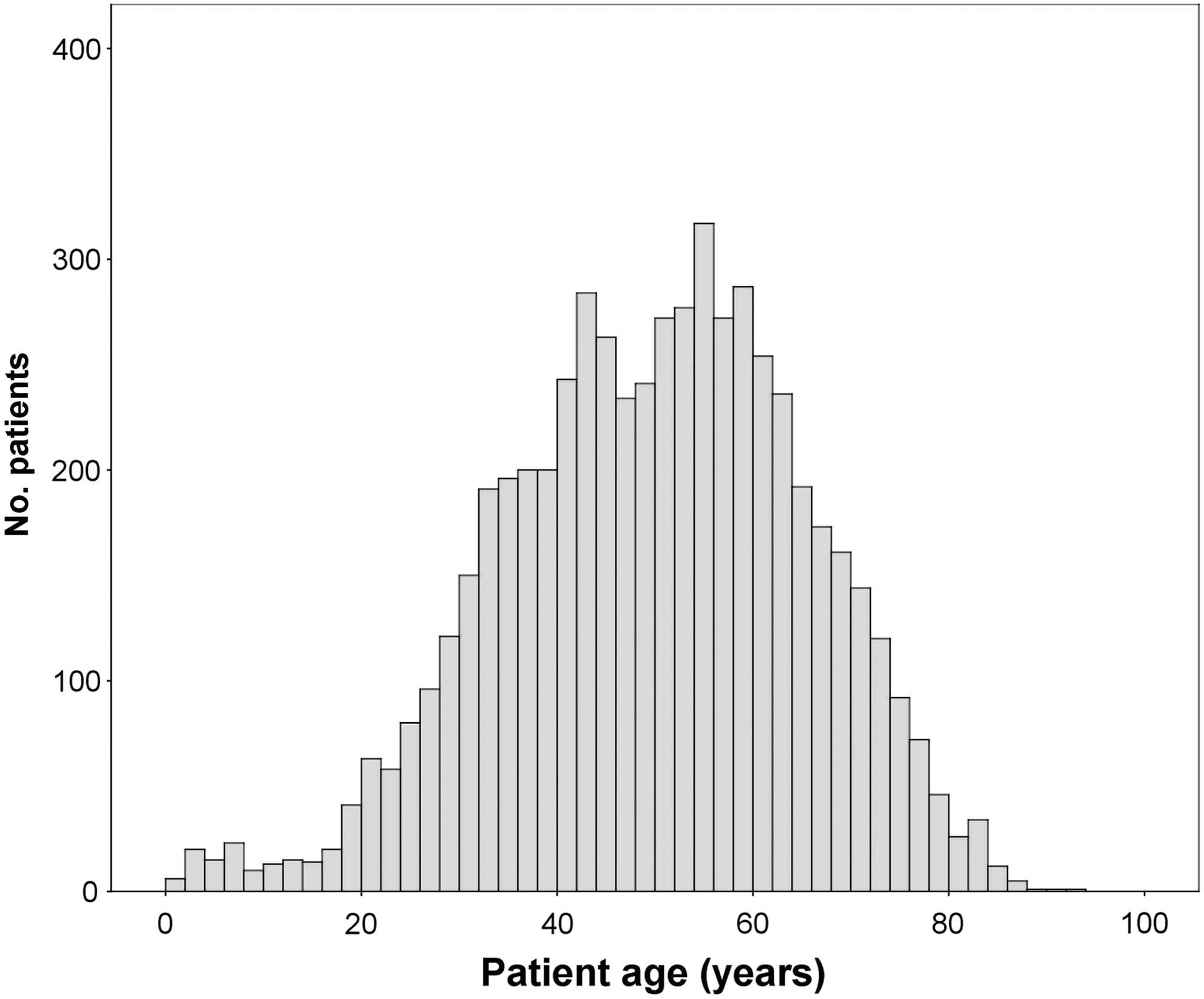
Age distribution of patients enrolled in the Percutaneous Nephrolithotomy Global Study (n = 5792).

Distribution of body mass index in patient cohort (n = 5556).
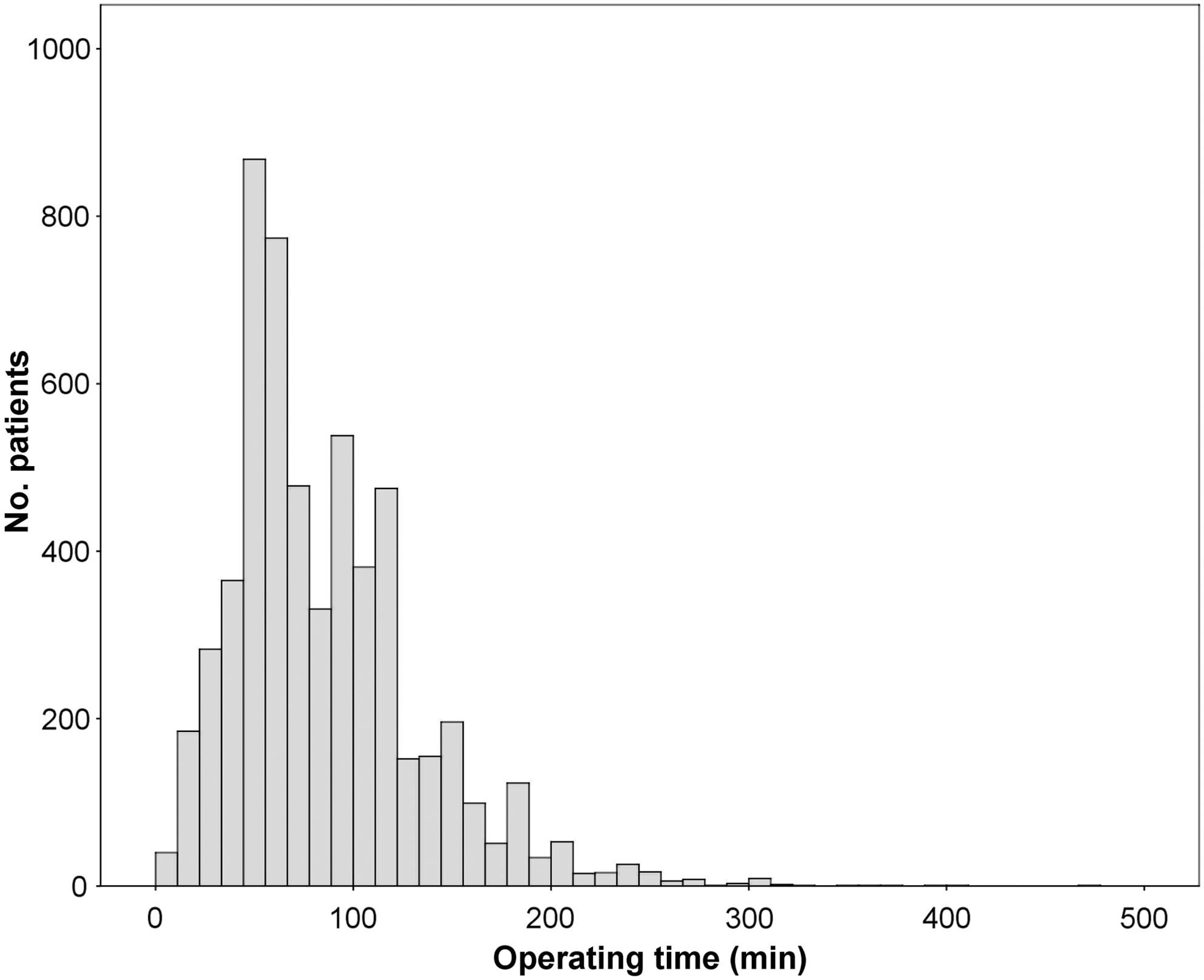
Distribution of operating times among patients who were treated with percutaneous nephrolithotomy (n = 5691).
SD = standard deviation; BMI = body mass index; PCNL = percutaneous nephrolithotomy; SWL = shockwave lithotripsy; URS =ureteroscopic stone removal; ASA = American Society of Anesthesiologists.
Renal stones were present in 391 patients with anatomic kidney abnormalities, including a functional monokidney (n = 189; 3.3%), a horseshoe kidney (n = 102; 1.8%), a malrotated kidney (n = 74; 1.3%), and an ectopic kidney (n = 26; 0.5%). A staghorn calculus was found in 1466 (27.5%) patients.
Intraoperative characteristics of PCNL
Access for PCNL was obtained by a urologist in 5170 (90.1%) patients and by a radiologist in 571 (9.9%) patients. The majority of patients were treated in the prone position (n = 4637; 80.3%), and others were treated supine (n = 1138; 19.7%). The stones were located in the upper calix in 940 cases, in the interpolar calix in 956 patients, and in the lower pole calix in 2603 patients. In the remaining cases, the stones were located in the renal pelvis. To obtain access, the puncture was made above the 11th rib in 87 (1.5%) patients, above the 12th rib in 861 (15.2%) patients, below the 12th rib in the remaining 4712 (83.3%) patients for whom there were data. Multiple punctures were performed in 461 (8.0%) of the total number of procedures. The imaging technique used for guidance to the upper tract was radiography alone in 3595 patients, renal ultrasonography alone in 589 patients, and both techniques combined in 846 cases. Other approaches to guide access in the remaining 625 patients included CT and endoscopy.
Conceptually, the similarities between telescopic and serial dilators led to the pooling of outcome with these two methodologies. Telescopic/serial dilators were used in 58.9% of cases and balloon dilators in 41.1%. Once access was obtained, fragmentation was performed using a pneumatic device (41.6%), ultrasonic device (24%), combined pneumatic and ultrasonic device (18.3%), laser (7.0%), electrohydraulic lithotripsy (1.0%); no device was used in 8.1% of patients.
Postoperative outcomes
The majority of patients received a percutaneous drain (91.2%), and a ureteral stent was introduced in 42.7% of patients. Operative procedures were considered uneventful in 4922 (85.5%) patients. In other patients, complications included significant bleeding (n = 446; 7.8%), renal pelvis perforation (n = 191; 3.4%), hydrothorax (n = 104; 1.8%), and failure to complete the procedure in 99 cases. Blood transfusion was administered in 328 (5.7%) patients, and fever >38.5°C occurred in 598 (10.5%) patients. The distribution of modified Clavien grading scores is shown in Table 3.
PCNL = percutaneous nephrolithotomy.
In 4336 (75.7%) patients, the urologist confirmed that the patient had become stone free. The stone-free rate was based on evaluation either by radiography (n = 4029; 73.4%), renal ultrasonography (n = 682; 12.4%), or CT (n = 775; 14.1%) The majority of patients did not receive any further treatment for renal stones (n = 4819; 84.5%), whereas ureteroscopy, repeated PCNL, and SWL were performed in 1.4%, 6.9%, and 6.2%, respectively.
Discussion
The present CROES PCNL Global Study is the largest prospective database of patients who have been treated with PCNL to be reported to date. The results reflect the routine clinical treatment of patients with a variety of indications for PCNL, and thus represent the use of this technique in a “real life” scenario. Use of a central reporting system not only allowed the study to have affordable global coverage but also facilitated rapid and standardized reporting from a wide variety of clinical centers. The study also confirms that a substantial, high-quality clinical dataset can be generated rapidly within the collaborative CROES network.
This first analysis of the study revealed an overall stone-free rate achieved by PCNL of 76%. While higher rates have been reported by some studies, this rate is consistent with those found for a variety of patient and renal characteristics. 5 Further analysis may identify which of these characteristics influence the stone-free rate in subgroups of this study population. An important finding of the study is that stone-free rates were most commonly determined by conventional radiography, and only 14% of stone-free patients were confirmed by CT. It is therefore likely that the true overall stone-free rate is lower than that reported, given the lower sensitivity of plain film radiography compared with CT. 17 Recurrence of renal stones in this patient population may then be higher. Alternatively, while almost one-quarter of patients had residual fragments, the proportion undergoing further treatment was only about 15%. Further analysis of these data may suggest how best to determine the stone-free rate, and which patients should be re-treated.
Notably, one-quarter of the study population had a large stone load, and a significant number of patients with special anatomic conditions were also treated. This amounted to nearly 400 patients with either a solitary functional kidney, a horseshoe kidney, with malrotation, or with an ectopic kidney. To the extent of our knowledge, this is the largest series of patients with rare conditions undergoing PCNL and will allow us to study outcomes in this patient subgroup in a separate analysis.
A large number of previous stone treatments had been undertaken, including PCNL, SWL, pyelolithotomy, or ureteroscopy. Further analysis of this patient group will address issues of whether different previous treatments worsen the outcomes of subsequent PCNL in terms of treatment success and PCNL-associated morbidity, as well as which patient characteristics are associated with previous treatment failure. Correlation of other patient characteristics, such as BMI, age, and the presence of comorbid illness, with outcomes will also be tested.
Overall, the data gathered by this multicenter observational study show that PCNL had a complication rate of 15%. Complications were documented by modified Clavien morbidity score, which has been shown to be a reliable tool for more objective outcome comparisons after renal stone treatment. 18 Modified Clavien scores were low and illustrate that, overall, PCNL is a safe procedure. Bleeding necessitating blood transfusion has been identified as the most common individual complication of PNCL. The overall transfusion rate of 5.7% in the current study compares favorably with rates of 11% to 17.5% in the literature, 8 although transfusion rates in the range 1% to 2.5% have been reported by more recent studies. 19 –21 Total complication rates after PCNL vary widely, with reported rates of between 29% and 83%. 7,8,16,22,23 Major or significant complications are, however, generally rare. Skolarikos and de la Rosette 23 have reported that the frequency of major complications after PCNL was 0.9% to 4.7% for septicemia, 0.6% to 1.4% for renal hemorrhage necessitating intervention, 2.3% to 3.1% for pleural injury, and 0.2% to 0.8% for colonic injury. Consequently, reported overall rates may include complications that are mostly clinically insignificant, such as minor bleeding or fever, combined with those that are significant, such as urosepsis or organ damage related to access. 8
The development of a PCNL-specific complication score that assigns complications score values commensurate with severity would be a valuable clinical asset. Despite the low complication rate of PCNL confirmed by this study, the difficulty of the procedure should not be underestimated. Training is still a very important issue, because complications in inexperienced hands can still be significant. 1 Percutaneous management of staghorn calculi in particular necessitates considerable expertise. 24
This global observational study of PCNL is the first study to be initiated by CROES, and the results it has generated represent an important clinical data resource. It is anticipated that through CROES, we will be able to provide insights into patterns of clinical practice around the world. This approach supports the communication of best practice across the urologic community, provides opportunities for innovation by our partners in industry, guides further development of existing technology, and, most importantly, helps deliver the best care to our patients.
Conclusion
PCNL is a milestone technique that has undergone a significant development in recent years. In experienced hands, PCNL has a very low major complication rate and a high success rate. The CROES PCNL Global Study confirms that PCNL remains an important therapeutic option for the minimally invasive removal of kidney stones.
Footnotes
Acknowledgment
The PCNL Global Study was supported by an unrestricted educational grant from Olympus.
Disclosure Statement
No competing financial interests exist.
Abbreviations Used
| Country | Principal investigator |
|---|---|
| Germany | Alken |
| Spain | Amon Sesmero |
| United States | Averch |
| Italy | Bianchi |
| Netherlands | Boellaard |
| Romania | Boja |
| Australia | Bolton |
| Romania | Botoca |
| United States | Breda |
| United Kingdom | Buchholz |
| Romania | Bucuras |
| Spain | Bueno Chomon |
| Italy | Cauda |
| Italy | Celia |
| Italy | Cormio |
| Italy | Crisci |
| Italy | D'Addessi |
| Argentina | Daels |
| Netherlands | de la Rosette |
| Italy | De Lisa |
| Italy | De Sio |
| India | Desai |
| Israel | Duvdevani |
| Turkey | Erdogru |
| Italy | Frattini |
| Italy | Garofalo |
| Romania | Geavlete |
| Italy | Giusti |
| India | Gopalakrishnan |
| Sweden | Grabe |
| United States | Grasso |
| Germany | Gross |
| India | Gupta |
| Mexico | Gutierrez |
| Netherlands | Hendrikx |
| France | Hoznek |
| Spain | Ibarlucea |
| India | Kandasami |
| India | Kapoor |
| Thailand | Kijvikai |
| Austria | Klingler |
| Netherlands | Kums |
| Turkey | Kural |
| Argentina | Labate |
| Greece | Liatsikos |
| United States | Lingeman |
| Portugal | Lopes |
| Spain | Lopez Garcia |
| United States | Louie |
| Denmark | Luke |
| India | Mandal |
| Greece | Melekos |
| India | Modi |
| Italy | Montanari |
| United States | Nadler |
| United States | Nakada |
| Japan | Nutahara |
| Germany | Olbert |
| Turkey | Onal |
| Denmark | Osther |
| Czech Rep | Pacik |
| India | Pal |
| United States | Pearle |
| United States | Preminger |
| Germany | Rassweiler |
| Canada | Razvi |
| Spain | Rioja |
| Italy | Rippa |
| Italy | Saba |
| France | Saussine |
| Italy | Scarpa |
| Spain | Serrano Pascual |
| India | Shah |
| China | Shi |
| Chile | Silva Barroilhet |
| Greece | Skolarikos |
| United States | Smith |
| Israel | Sofer |
| Germany | Stolzenburg |
| Netherlands | Strijbos |
| China | Sun |
| Canada | Szymanski |
| Turkey | Tefekli |
| United Kingdom | Timoney |
| United Kingdom | Tolley |
| Turkey | Turna |
| Spain | Valdivia-Uria |
| Belgium | Van Cleynenbreugel |
| United States | Venkatesh |
| Netherlands | Vijverberg |
| Sweden | Walfridsson |
| United States | Wolf |
| United States | Wong |
| China | Xue |
| Japan | Yamaguchi |
| China | Zhang |