
Abstract
Robot-assisted partial nephrectomy (RAPN) is emerging as a viable minimally invasive surgical technique for small renal tumors. The warm ischemia time (WIT) during laparoscopic partial nephrectomy has been reduced using an early unclamping (EU) technique. We present our technique of EU technique in RAPN. From November 2009 to June 2010, 12 consecutive RAPNs were performed by a single surgeon (A.W.) using EU technique. The median operative time was 227 minutes (176–315); median WIT, 16 minutes (11–25). Median estimated blood loss was 150 mL (50–500) and length of stay 2 days. There were no intraoperative or postoperative complications. RAPN using EU technique is a safe and feasible option in experienced hands, allowing for a shorter WIT without increasing blood loss. This approach requires a highly skilled bedside assistant who is imminently familiar with the robotic system and advanced laparoscopic techniques.
Introduction
Technique
Bowel preparation: One 10-ounce bottle of magnesium citrate and clear liquid diet the day before surgery.
Patient position: Modified lateral position (30-degree tilt). Pressure points carefully padded with pillows and foam pads. Table positioned at 20–30-degree contralateral tilt (Fig. 1).
Trocar position: After establishment of pneumoperitoneum, abdominal access and camera port placement is achieved using a 12-mm visual access trocar 10 cm lateral and 3 cm superior to the umbilicus. Two robotic working ports are placed: left working port 3 cm medial to the ipsilateral anterior superior iliac spine; right working port below the costal margin in the midclavicular line. Two assistant ports are placed: left-hand 12-mm port 5 cm inferior to the camera port; right-hand 5-mm port placed in the upper midline. For right-sided procedures, a 5-mm trocar is added for liver retraction (Fig. 2). In the case of high-body-mass-index patients, we modify the port placement to a more lateral position.
Docking the robot: The robot is docked over the ipsilateral shoulder at a 30-degree angle from the patient's spine.
Procedure: 0-degree camera lens is used throughout the procedure. Once the colon is mobilized, ureter and lower pole are lifted off psoas muscle, hilum is identified, and the renal artery is dissected from the vein. For upper pole tumors the entire kidney is mobilized from sidewall and diaphragm, which is usually not necessary for lower pole tumors. We use intraoperative ultrasonography in all cases for identification and demarcation of tumor margins, which are scored into the capsule with cautery 5 mm from nearest edge of tumor. While the assistant performs ultrasonography, the surgeon employs the TilePro feature, allowing observation of ultrasonography image and laparoscopic image simultaneously. The artery is clamped by the bedside assistant using two straight laparoscopic bulldog clamps, and the surgeon resects the tumor with endoshears. The surgeon controls the scissors and bipolar with the first and second arm respectively, whereas the assistant uses the suction/irrigation to keep the field clean and a grasper for holding the kidney if needed. Often during tumor resection, we raise pneumoperitoneum pressure to 20 mmHg to allow liberal suction by the assistant. Once the resection is completed, the Argon Beam is used for coagulation of the periphery of the resection bed (making sure to open a port vent during this infusion of gas). A running 3-0 Vicril on an SH needle (Ethicon Inc.) or self-locking, 3-0 absorbable Polyglyconate suture (V-lock 90™; Covidien Inc.) is used to close large sinuses, end arteries, and collecting system at the base of the resection. This is secured with a Lapra Ty (Ethicon Endo-Surgery Inc.). The bulldog clamps are removed. The assistant compresses the resection bed with a 4 × 4-inch gauze (preplaced) and any pulsatile bleeding oversewn using 3-0 Vicril. When arterial bleeding is controlled, 3 or 4 interrupted 0-Vicryl sutures on CT-1 needles (Ethicon Inc.) are placed across the defect to close the parenchyma upon itself using a sliding renorrhaphy technique with large Hem-o-lok® clips (Teleflex Medical) and LapraTys. 8 A perirrenal fat flap can be placed into larger defects, but no fibrin glue or cellulose rolled bolsters are used. Gerota's fascia is closed over the repair using 0 Vicryl on CT-1 needle and the kidney fixed to the lateral wall with Vicril if it was completely mobilized. The robot is undocked. The 30-degree standard laparoscope is inserted for closing. The specimen is placed into a 10-mm specimen bag. A Jackson-Pratt drain is brought out through the lower 8-mm robotic port site. The specimen is removed from the 12-mm assistant port with extension of the incision if necessary.
Closing: A fascial closing device is used for closing the two 12-mm ports using #1 Vicril suture. Absorbable monofilament 4-0 suture is used for subcuticular skin closure.
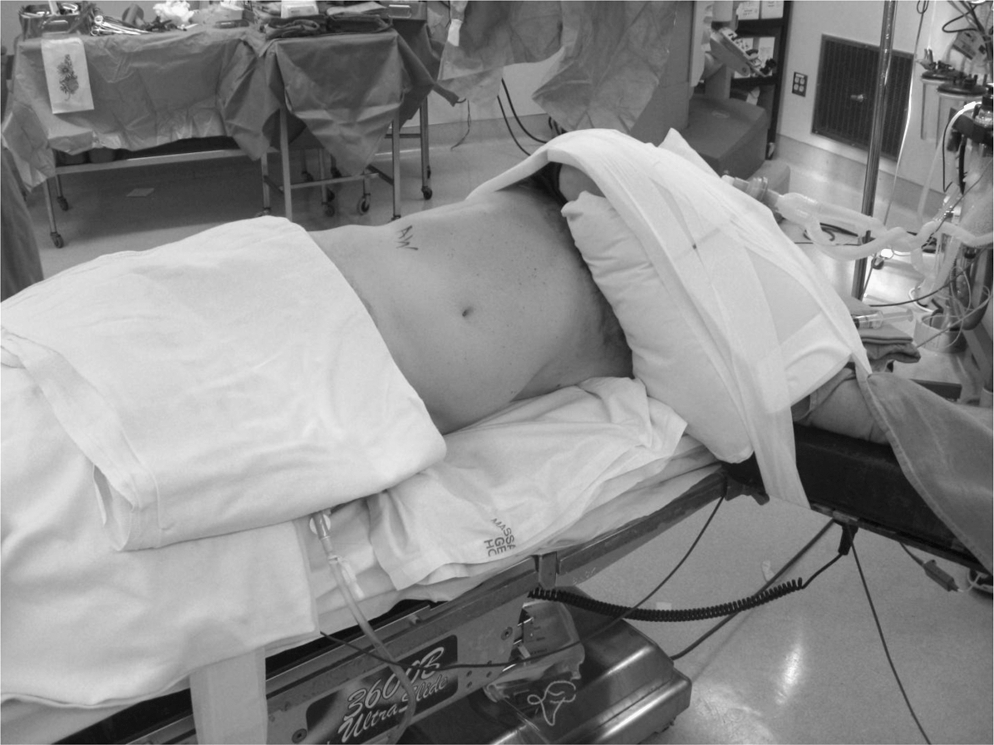
Patient position. The patient is positioned in a modified lateral tilt (30 degrees) and secured to the operating table, which is then tilted 20–30 degrees to create a flank position. The table is positioned at a 30-degree angle relative to the robot.
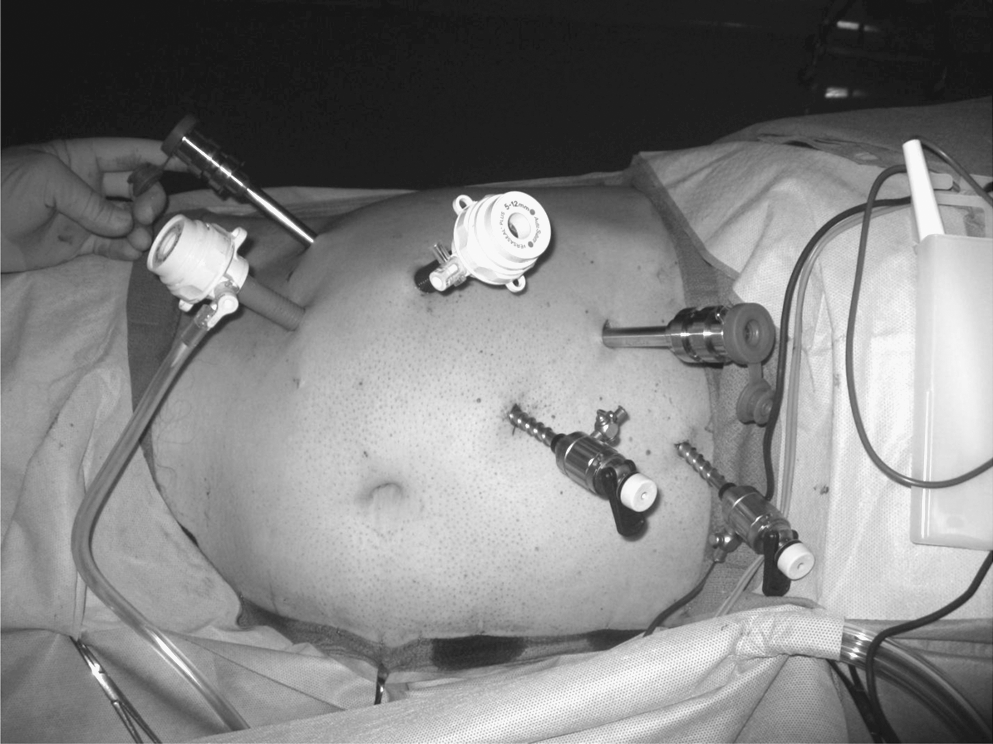
Trocar placement. A 12-mm visual trocar is 10 cm lateral and 3 cm superior to the umbilicus for the camera. Two 8-mm robotic working ports are placed, one just medial to the anterior superior iliac spine and one below the costal margin at the mid-clavicular line. One 12-mm assistant port is placed in the right lower quadrant. One 5-mm assistant port is placed on the upper midline and for right side cases; a 5-mm trocar is added for liver retraction.
Equipment
Da Vinci Surgical System S HD (Intuitive Surgical Inc.)
Fenestrated bipolar forceps, curved scissors, and large needle drivers (Intuitive Surgical Inc.)
Laparoscopic 0- and 30-degree lens and Da Vinci 0-degree lens
Two 12-mm trocars (one visual and one bladeless obturator)
One (left side) or two (right side) 5-mm trocars for assistant
Laparoscopic suction/irrigator
Laparoscopic graspers and scissors for assistant
Laparoscopic ultrasound probe
Two long, straight (45 mm) laparoscopic bulldog clamps and applier/remover (Aesculap AG & CO)
Laparoscopic argon beam coagulator
V-Loc™ 90 3-0 absorbable polyglyconate knotless wound closure device and V-20 needle (Covidien Inc.)
Vicryl 0 (CT-1 needle) and 3–0 (SH needle) (Ethicon Inc.)
Hem-o-lok® Large size (L-purple) clips and applier (Teleflex Medical Inc.)
Lapra-Ty™ absorbable suture clips and applier (Ethicon Endo-Surgery Inc)
Endoscopic specimen bag, 10 mm.
Closed suction drain
Role in Urologic Practice
We started to use the RAPN EU technique after experience with >100 LPN, >150 laparoscopic radical nephrectomies, 5 robotic radical nephrectomies, and 5 RAPN performed using the standard clamping technique where the entire reconstruction was performed during WIT. Additionally, our robotic team had experience with >100 radical prostatectomies. We hypothesized that resection and reconstruction might be augmented by the improved optics and instrumentation of the robotic system. This transition to the EU technique was only attempted after achieving a certain level of expertise with both laparoscopic and robotic upper tract surgery. Moreover, these cases were attempted only after robotic team cohesiveness and experience had matured. Of the 12 patients, median age was 58 years and body mass index 29. Median tumor size was 2.6 cm, with the majority in the upper pole. Median operative time was 227 minutes, WIT 16 minutes, EBL 150 mL, and hospital stay 2 days (Table 1). Pathologic examination showed two benign tumors and one positive margin. There were no intraoperative or postoperative complications. By comparison, in our initial five cases performed according to the standard technique, we experienced a median surgical time, WIT, and EBL of 266 minutes, 27 minutes, and 100 mL, respectively. Definitive conclusions cannot be drawn from these data because of the small number of patients; however, there was an important and immediate reduction in WIT (median reduction 11 minutes).
BMI = body mass index; WIT = warm ischemia time; ASA = American Society of Anesthesiologists; RCC = renal cell carcinoma.
It is well known that shorter WIT is desirable during partial nephrectomy. Becker et al 5 concluded that WIT should not be >20 minutes regardless of surgical approach. Gill et al 9 showed a reduction of WIT over time from 32 to 14 minutes, primarily by using the EU technique. In our current series, WIT was reduced by 40% (27 to 16 minutes). Longer-term follow-up of renal function will allow us to determine whether this reduction is clinically significant.
We have found visualization very good during resection, allowing for safe dissection of tumor. After resection, suturing the base of the defect, and removing the clamp, there are often 1–2 arterial bleeders that need to be addressed. Expert assistance allows for localization of these vessels. This step is also facilitated by a 4 × 4-inch X-ray detectable sponge, which allows direct compression. Subjectively, we have felt far more comfortable with overall hemostasis with this technique, even during hilar tumor resection, as all arterial vessels are controlled before closing the renal parenchyma over itself.
The role of the bedside assistant cannot be underestimated during both kidney mobilization and tumor resection. The bedside assistant must possess the ability to create traction/countertraction, place and remove laparoscopic bulldog clamps, aggressively clear operative field of blood during tumor resection, cauterize cortical edges with the argon beam coagulator, rapidly introduce and retrieve sutures, and place any laparoscopic clips during reconstruction of the kidney.
Major disadvantages of RAPN using EU include the lack of surgeon control of hilar clamping and unclamping, requirement for an experienced bedside assistant, and the surgeon need for advanced robotic training and upper tract laparoscopy experience.
In conclusion, RAPN using the EU technique is safe and feasible in the hands of experienced surgeons and robotic surgical teams. The EU technique did not increase EBL in our series, and the WIT is comparable with the EU technique in the largest LPN series. RAPN, in particular the EU technique, requires a highly skilled bedside assistant.
Footnotes
Disclosure Statement
A. Wagner received an unrestricted educational grant, not used for this project, from Intuitive Surgical, Inc.
Abbreviations used
*
A video demonstrating this technique is available at
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.