
Abstract
Purpose:
Laparoendoscopic single-site (LESS) surgery was used to treat various urological operations by a single surgeon who was skilled in conventional laparoscopic surgery. The effectiveness and safety of the procedure were examined.
Patients and Methods:
LESS surgery was performed on 70 patients by using a homemade single port device composed of an Alexis® wound retractor and a powder-free surgical glove. There were 29 cases of varicocelectomy (including two bilateral cases), 21 cases of renal cyst marsupialization (including one bilateral case), 16 cases of ureterolithotomy, 3 cases of radical nephrectomy, and 1 case of radical nephroureterectomy. The mean patient age was 42.90 ± 17.58 years (range, 11 to 74 years), and the male-to-female ratio was 55:15.
Results:
In two cases (one ureterolithotomy and one radical nephrectomy), the LESS surgery was converted to conventional laparoscopic surgery. The mean operative time was 96.02 minutes (range, 30 to 285 minutes), the estimated blood loss was 60.80 mL (range, 0 to 500 mL), and the mean hospital stay was 5.10 days (range, 3 to 15 days). Only one patient had to use patient-controlled anesthesia due to pain; none of the patients developed major complications; and all patients were satisfied, with 85.7% expressing a high degree of satisfaction.
Conclusion:
In the urological field, LESS surgery using a homemade single-port device appears to be a feasible and safe surgical treatment option that could replace conventional laparoscopic surgery.
Introduction
Before they can be routinely used, new surgical procedures have to be not only safe and reproducible but also practical. Although LESS surgery has been performed all over the world by using ready-made commercially available single-port devices, such devices may not be suitable for the medical environments of other countries. Two Korean studies have shown that it is possible to perform LESS operations by using a homemade single-port device composed of a wound retractor and a surgical glove. 3,4 To assess the safety and reproducibility of this device in the urological field, the first 70 cases that were performed by a single surgeon in a single center were assessed.
Patients and Methods
Patients
Between January 2009 and January 2010, a surgeon (S.W.L.) skilled in conventional laparoscopic surgery used LESS surgery to treat 70 cases of urological diseases. The surgical decisions were made after obtaining informed consent from the patients and Institutional Review Board approval from the ethical committee of the hospital. The same inclusion and exclusion criteria that are used for conventional laparoscopic surgery were applied. There were 29 cases of varicocelectomy (two were bilateral), 21 cases of renal cyst marsupialization (one was bilateral), 16 cases of ureterolithotomy, 3 cases of radical nephrectomy, and 1 case of radical nephroureterectomy. The mean patient age was 42.90 ± 17.58 years (range, 11 to 74 years), the male-to-female ratio was 55:15, and the mean body mass index was 23.52 ± 2.46.
General surgical procedure
For all operations, the patient was placed under general anesthesia, and a 2–4 cm circular incision was made in the lateral side of the umbilicus. A 1-cm extended fascial incision was then made, and the peritoneum was resected by using an open technique. The transperitoneal approach was used for surgery. A homemade single-port device was constructed by using an Alexis® wound retractor (Applied Medical, Rancho, Santa Margarita, CA) and a powder-free surgical glove (Triplex P-free Glove®; KM Healthcare, Guri, Korea). The wound retractor was inserted into the umbilicus incision site, and the upper part of the wound retractor ring was covered with a size 6 or 6½ surgical glove (Fig. 1A). The surgical glove was folded and inserted so as to minimize the gap between the abdominal wall and the glove. Three fingers of the glove were cut off, and three trocars were inserted and immobilized with 1-0 silk (Fig. 1B). The three trocars consisted either of one 5-mm and two 12-mm trocars, or one 12-mm and two 5-mm trocars. Intraperitoneal CO2 pressure was maintained at 15 mmHg. A 10-mm rigid laparoscope was inserted into the peritoneum through the 12-mm trocar along with the homemade single-port device; and the whole peritoneum, including the area destined for surgery, was examined. The flexible laparoscopic instruments, namely the LaparoAngle® (CambridgeEndo, Framingham, MA) and the Roticulator® (Autosuture, Norwalk, CT), were then inserted through the remaining trocars and passed into the peritoneal cavity through the single incision port. Surgery was performed by bending the tip of the articular laparoscopic equipment (Fig. 1C, D) so that it had a shape similar to the basic 5th movement of ballet (Fig. 2). In cases where more instruments were required during surgery, an additional finger of the glove was cut, a trocar was installed as described earlier, and the required instrument was inserted. After completing the surgery, the skin of the single incision site was sutured with Dermabond® (Ethicon Inc., Somerville, NJ).
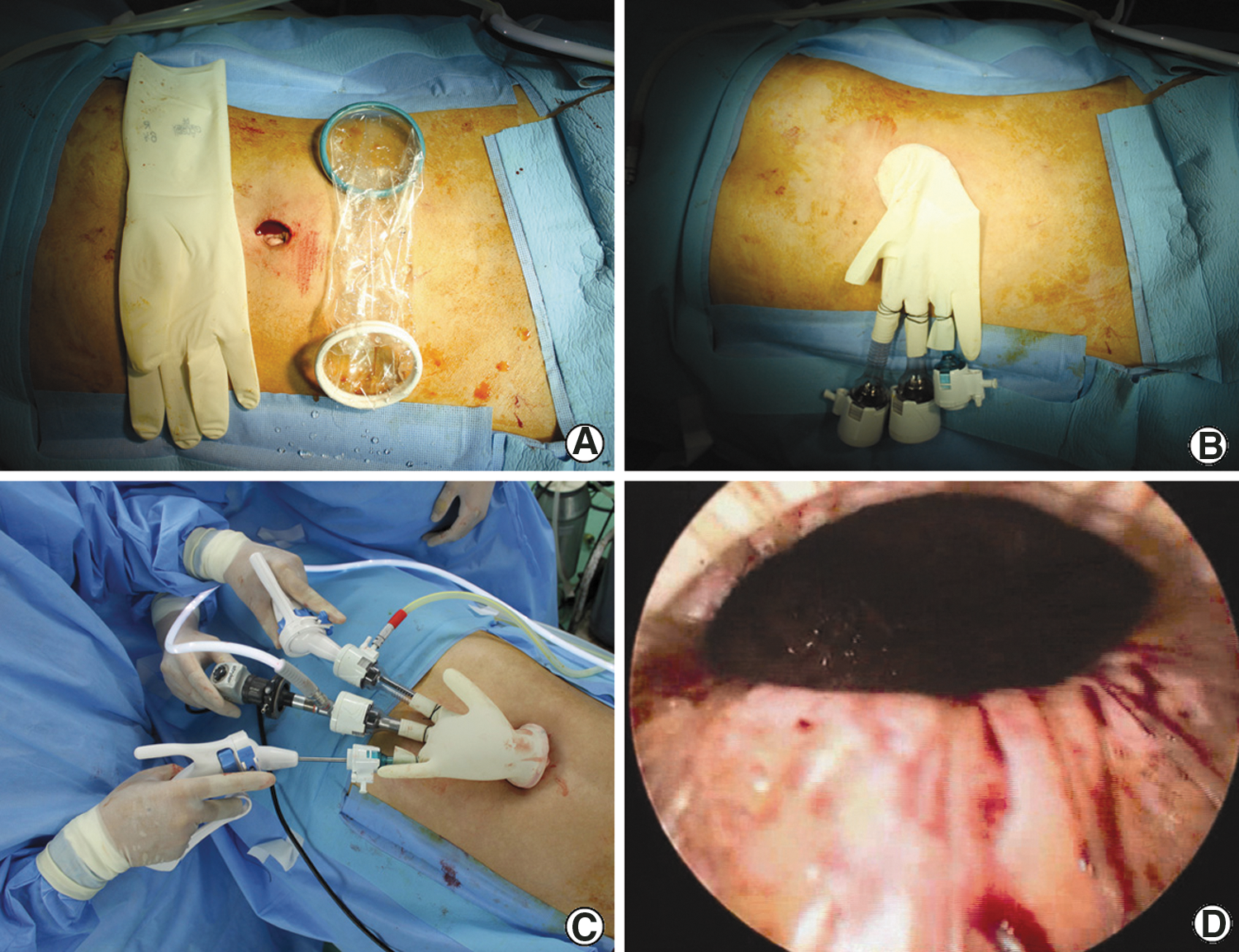
Laparoendoscopic single-site surgery.

Schematic illustration shows a shape similar to the basic 5th movement of ballet.
LESS varicocelectomy
The patients were placed under general anesthesia and oriented in the supine position, after which the homemade single port device was installed, the 20° Trendelenberg position was taken, and the surgery was performed. For this, the mesentery or intestine attached to the surgical area was dissected. In addition, the retroperitoneum was dissected in the area 2–3 cm above the internal inguinal ring along the spermatic vessels and in the lateral side. The spermatic vessels and adjacent tissues were also dissected. The artery in the exposed spermatic vessels was identified on the basis of its pulsation, after which it was separated from the vein. Two Hem-O-Lok clips (Weck, Research Triangle Park, NC) were then installed at the proximal and distal sites of the separated spermatic vein, and the area between the clips was cut. To treat the contralateral variococele in bilateral varicocele cases, the operator and the first assistant moved to the opposite side of the patient and rotated the camera by 150°; thus, additional transcutaneous ports were not needed. After checking for hemorrhage, the homemade single-port device was removed. A drain was not inserted.
LESS renal cyst marsupialization
After resecting the line of Toldt, the large intestine was retracted to the medial side, and the kidney was exposed. In cases where the cysts were covered by the liver or spleen, an additional glove finger was cut off, and another instrument was inserted to expose the lesion by traction. In most cases, the renal cyst was readily detected due to the protrusion of Gerota's fascia. After dissecting the fascia, the renal cyst fluid was aspirated by tapping; its color and volume were assessed; and it was subjected to cytological and chemical tests. The cystic wall was resected and sent out for histopathological analysis. The remaining renal cystic wall was electrocauterized to prevent recurrence. To treat the contralateral cyst in bilateral cyst cases, the patient was simply placed in the opposite flank position; thus, additional transcutaneous ports did not have to be inserted. After checking for hemorrhage, the homemade single-port device was removed. A drain was not inserted.
LESS ureterolithotomy
Under general anesthesia, the patient was placed in the flank position, and surgery was performed. Within the peritoneum, the large intestine was resected and placed on the medial side, and the ureter was exposed. After locating the ureteral stones, a longitudinal incision that was big enough to remove the stones was made with a pair of laparoscopic Metzenbaum scissors, and the stones were removed with laparoscopic forceps. Subsequently, the Roadrunner guidewire (Cook Inc., Chicago, IL) that had been placed below the stones before starting the surgery was advanced upward, and the vertically resected ureter was subjected to continuous suture using 5-0 polyglactin. Surgicel® (Ethicon Inc.) was then placed onto the suture area. Large stones were placed into a Lap-bag® (Sejong Medical, Paju, Korea), which was then extracted. After confirming the absence of hemorrhage, a drain was placed in the vicinity of the ureter. The patient was then placed in the lithotomy position, and a double-J stent was inserted by using the guidewire that had already been inserted through the ureter.
LESS radical nephrectomy and nephrouretectomy
After installing a urethral Foley catheter and a nasogastric tube, the patient was placed in the flank position slanted by 70° and surgery was performed. The large intestine was dissected along the line of Toldt, and the kidney was exposed. While dissecting the area between Gerota's fascia and the lower pole of the kidney, the renal artery was identified by approaching the renal hilum, after which it was clamped with 4-5 Hem-O-Lok clips and resected. The renal vein was then ligated by using an endovascular stapler. Thereafter, the ureter was ligated with clips and resected. In radical nephroureterectomy cases, the distal ureter was dissected to render it fully mobile, after which the bladder was dissected as much as possible, the tissues (including the bladder cuff) were ligated using Hem-O-lok and LaproTy clips, and the distal ureter was resected. The resected kidney was moved to the lateral side of the peritoneum, inserted into a Lap-bag that had been inserted into the peritoneum through the 12-mm port, and extracted. Thereafter, the pressure within the peritoneum was decreased to below 5 mmHg, and the possibility of hemorrhage was assessed. In two cases, a drainage tube was not inserted; whereas in two cases where the hemorrhage site could not be assessed even by careful hemostasis, a drainage tube was inserted and the port device was removed.
Statistical analysis
The success of all 70 cases of LESS was evaluated by determining the number of cases of conversion to open abdominal surgery, the operation time, the surgical complications, the dose of analgesics needed after surgery, the duration of hospital stay, the duration of the postsurgical recovery period, and the time needed to return to routine life. Safety was evaluated by assessing the complications that occurred before and after surgery. The pain experienced by the patients was analyzed by using the preoperative and postoperative 10-point visual analogue pain scale (VAPS), where no pain and the worst pain are scored at 0 and 10 points, respectively. Before discharge after surgery, the patients were instructed to complete the VAPS at home on postsurgery days 1, 2, 3, and 7 days, and bring the completed forms when visiting the outpatient clinic. Patient satisfaction was evaluated by using a four-level classification method comprised of very satisfied, somewhat satisfied, somewhat dissatisfied, and very dissatisfied. With regard to our study, a patient was deemed to be satisfied if he or she reported being very or somewhat satisfied. Paired t-test was used to compare the preoperative and postoperative VAPS scores. Data and statistical analyses were performed by using the Open
Results
Of the 70 cases of LESS surgery using a homemade single-port device, conversion to conventional laparoscopic surgery occurred in two (2.86%), namely a ureterolithotomy case and a radical nephrectomy case (Table 1). Both cases occurred shortly after the surgeon had started performing LESS surgery; after LESS, ureterolithotomy and LESS radical nephrectomy were each performed twice, and none of the subsequent cases had to be converted to conventional laparoscopic surgery. For the 70 cases of LESS surgery, the mean operation times for varicocelectomy, renal cyst marsupialization, ureterolithotomy, radical nephrectomy, and nephroureterectomy were 51.84 ± 12.15, 115.18 ± 6.91, 137.40 ± 33.91, 139.40 ± 27.87, and 285 minutes, respectively. The mean estimated blood loss for all patients during surgery was 60.80 ± 75.37 mL. Three patients had to receive transfusions due to a decrease in serum hemoglobin levels (4.29%); each patient only received 1 pint. There were five cases of minor postsurgical complications (7.14%), namely fever (three cases, 4.29%) and mild ileus (two cases, 2.86%). There were no major complications. For all 70 patients, the average hospital stay was 5.10 ± 2.20 days; whereas for varicocelectomy, renal cyst marsupialization, ureterolithotomy, radical nephrectomy, and nephroureterectomy, the average hospital stays were 4.72 ± 1.21, 4.45 ± 1.04, 4.40 ± 1.17, 9.67 ± 1.53, and 15 days, respectively (Table 1). For all 70 patients, the VAPS scores on postsurgery days 1, 2, 3, and 7 were 4.14 ± 1.36, 2.48 ± 1.09, 1.78 ± 0.13, and 0.92 ± 0.78, respectively (p < 0.001 when the day 1 VAPS score was compared with the day 2, 3, or 7 scores) (Table 2). Only one patient used patient-controlled anesthesia after surgery (1.43%). Of the 68 patients on whom LESS surgery was successfully performed, all began oral intake immediately after surgery, and the return to routine life occurred on average 3.54 ± 1.84 days after surgery. The survey on the level of satisfaction felt by the patients revealed that 60 (85.71%) felt very satisfied and the remaining ten (14.29%) felt somewhat satisfied; thus, all patients treated with LESS expressed satisfaction. The average wound size of patients 1 month after surgery was 3.06 ± 0.26 cm.
BMI = body mass index; EBL = estimated blood loss; OR = operating room; LESS = laparoendoscopic single-site.
VAPS = visual analogue pain scale.
With regard to the LESS varicocelectomy cases, a physical examination performed 1 month after surgery revealed the loss of the varicocele in all patients. Of the patients who presented with pain in the scrotum, the average VAPS scores before surgery and 1 month after surgery were 6.75 ± 1.03 and 0.75 ± 0.70, respectively; this represents a statistically significant decrease in pain after the operation (p < 0.001). In terms of postsurgical pain, analgesics were injected 1–2 times intramuscularly on the day of surgery but were not required after discharge. With regard to complications, there were two cases where an air layer was detected within the scrotum; both cases had occurred earlier on in the surgeon's experience with LESS. This problem was resolved by compressing the scrotum immediately after surgery. The varicocele did not recur in any of the patients. Eleven cases showed reduced sperm counts in the presurgical semen analysis, but the average postoperative sperm counts at the follow-up analysis performed 3 months after surgery were significantly higher than the preoperative sperm counts (29.36 ± 5.39 × 106/mL vs. 10.72 ± 3.65 × 106/mL; p < 0.001). The average sperm motility was also significantly higher after surgery than before surgery (41.45% ± 6.90% vs. 30.45% ± 7.98%; p = 0.004), as was the average percentage of sperm with a normal shape (16.82% ± 4.60% vs. 8.27% ± 2.57%; p < 0.001). However, two cases continued to showed hypospermia after surgery.
With regard to LESS renal cyst marsupialization, 1, 7, and 2 case involved one or more cysts on the left, right, and both sides, respectively. Fifteen and six cases had one and two cysts, respectively. The surgery was successful in all 21 cases, thus yielding a success rate of 100%. The average hospital stay was 4.45 days (range, 3 to 7 days). The only postsurgical complication was pain, which was only observed in two cases; in both cases, the pain was relieved by conservative treatments. Pathohistological tests revealed that all cysts were simple renal cysts. The average follow-up period was 4.52 months (range, 3 to 6 months), during which time none of the patients presented with symptoms that were due to the LESS surgery.
With regard to LESS ureterolithotomy, one of the ten cases was converted to conventional laparoscopic surgery to control bleeding. Of the 15 cases in which LESS surgery was successfully performed, an intravenous urography performed 1 month after surgery failed to detect any stone remnants. The mean estimated blood loss was 80.0 ± 34.96 mL and there were no intraoperative complications, including the need for transfusion. The mean hospital stay after surgery was 4.40 ± 1.17 days, and the ureteral stents were removed on average after 21.2 ± 4.21 days. There was no urine leakage or other postoperative complications.
With regard to radical nephrectomy and nephroureterectomy, conversion to conventional laparoscopic surgery was needed for one of the three radical nephrectomy cases due to intraoperative bleeding during renal artery dissection; this was also the first LESS radical nephrectomy experience for the surgeon. After the conversion to conventional laparoscopic surgery, the bleeding was successfully controlled and the radical nephrectomy could be completed.
Despite excellent surgical outcomes of LESS surgery, we found several shortcomings of the homemade single-port device in our experiences. In five cases, a surgical glove was torn due to needle puncture and instruments. Five cases included three cases of ureterolithotomy and one case each of varicocelectomy and radical nephrectomy. Tegaderm® (3M Health Care, St. Paul, MN) was applied to the puncture site of the homemade single-port device in four cases, and the whole port device was changed in nephrectomy. Mean time for making port device and inserting was 7.23 ± 1.21 minutes. This time was shortened as the surgical procedure progressed.
Discussion
The LESS technique was first attempted and reported about 10 years ago. 5,6 Due to limitations in the ergonomic surgical equipment that was available at that time, the rates of surgical success and reproducibility were very low, which hampered the widespread general use of the LESS technique. However, the development of various single port devices, flexible laparosopes, and other instruments has reignited interest in the LESS technique. In the urological field, LESS nephrectomy was described for the first time by Rane et al 7 during the 2007 World Congress of Endourology Meeting; this operation involved the use of the R-port (Advanced Surgical Concepts, Dublin, Ireland). Thereafter, many surgeons used this technique to treat various urological diseases, which led to a number of reports on its usefulness and safety. 8 Initially, several terms were used to describe laparoscopic surgery through a single incision site, namely natural orifice transluminal endoscopic surgery, single port access, and LESS. However, in 2008, the Laparoendoscopic Single-Site Surgery Consortium for Assessment and Research proposed that the term “LESS” should be used. 9
In 2009, Desai et al 10 described their first 100 cases of LESS surgery, all of which involved the R-port. They reported that in the study period, the 100 cases of LESS surgery accounted for 15% of all laparoscopic surgery cases; conversion to conventional laparoscopic surgery was needed for three cases; additional ports were installed in three cases; and conversion to open surgery was needed for four cases. White et al 11 also described their first 100 cases of LESS surgery using the R-port in 2009. They reported that six cases had to be converted to conventional laparoscopic surgery due to intraoperative bleeding, failure to progress, and/or inadequate exposure of the operation field. Subsequently, in 2010, Jeon et al 12 described their first 50 cases of LESS and robotic LESS surgery using a homemade single-port device composed of a wound retractor and a surgical glove; and Han et al 13 described 14 cases of LESS nephrectomy that were performed by using the same homemade single-port device. Both reports indicated that all surgeries had been successfully performed without having to convert to open surgery or conventional laparoscopic surgery. The need for the homemade single-port device arose, because the Korean Food and Drug Administration did not approve the use of the R-port or the Uni-X single laparoscopic port system (Pnavel Systems, Morganville, NJ) in Korea. They stated that the homemade single-port device has several advantages: Additional entrapment bags are unnecessary in small specimens; extraction can be readily and rapidly performed by using one finger of the device; intra-abdominal smoke can be removed by using the trocar valve; and the tamponade effect of the wound retractor can prevent port-site bleeding and subcutaneous emphysema.
With regard to the 70 LESS surgery cases described here, the surgery was successfully performed without having to install additional ports in 97.14% of the patients. In addition, the symptoms improved after surgery and complications did not develop. LESS surgery is associated with several advantages. First, only one incision is involved, which elevates patient satisfaction in terms of esthetic outcome and reduces pain after surgery. Indeed, in the present study, the postoperative VAPS scores revealed a substantial reduction of pain after surgery; and 84% of the patients stated that they were very satisfied by the operation. Second, one incision suffices for bilateral surgery, as the contralateral side can be accessed by simply changing the position of the patient or the direction of the operators. Third, the operative time needed for LESS is reasonable. In the present study, the mean operative time was 96 minutes, which is considerably shorter than the mean operative times needed for the LESS surgeries previously reported (Table 3). Fourth, patients recover and return to normal life rapidly. In the present study, all patients were able to take food on the day of surgery and returned to routine life on average 3.54 ± 1.84 days after surgery.
Ryu et al only reported retroperitoneal LESS cases.
C-LESS = conventional LESS; R-Less = robotic LESS.
Compared with commercial single-port devices, homemade single-port devices composed of a wound tractor and a surgical glove have several advantages. First, they allow the laparoscope and instruments to be freely moved in a limited space. Second, the elasticity of the surgical glove minimizes the interference of the instruments with the laparoscope. In fact, the space of homemade single-port devices may be larger than commercial port devices. These advantages may make it easier to control the instruments. Third, in complex surgeries, additional surgical instruments can be inserted by cutting off extra fingers from the glove. Indeed, the ability to add trocars means that traction using an additional rigid instrument can be applied when the lesion is located in the upper kidney pole and, thus, is covered with the liver or the spleen. Fourth, the cost is low compared with that of commercial single-port devices (R-port vs. homemade single-port device; 550,000 KRW vs. 350,000 KRW, as ∼468.6 USD vs. 298.2 USD in Korea). 14 The shortcomings of the single-port device are that it takes some time to construct the device during surgery. Surgical glove tear and the interference of the instruments, which may be minimized as compared with commercial port devices, are also major problems of homemade single-port devices. These two disadvantages resulted from longer distance of the homemade single-port device than the commercial port device. In our early cases, instruments were trapped in the abdomen wall and ring of wound retractor when they are inserted through a trocar. Those lead to an indigent posture to operator and assistants. In addition, we had difficulty in removal of intra-abdominal smoke. Since opening the trocar valve is not effective, a suction device should be used to remove intra-abdominal smoke. Nevertheless, the many advantages of homemade single-port devices mean that effective and safe LESS surgery can be performed even when commercial products are not available. This is borne out by our study.
Conclusion
LESS surgery using a homemade single-port device composed of a wound retractor and a surgical glove has the advantage that it is minimally invasive and can be readily performed by using flexible instruments. Our study describing the use of this system in the urological field showed that it is associated with high levels of patient satisfaction and good surgical outcomes. Under the condition without ready-made ports, LESS surgery utilizing homemade single-port devices showed the possibility of a feasible new treatment option that could suggest being scar free. To compare the safety and effectiveness of this system with that of conventional laparoscopic surgery, studies on more patients are required.
Footnotes
Disclosure Statement
No competing financial interests exist.